In their recent article, Kubaloglu and associates reported a favorable result with the insertion of a single 210-degree arc length intrastromal corneal ring (ICR) for the treatment of pellucid marginal degeneration (PMD). They join a number of others advocating the use of ICRs for the correction of PMD. The same month, another article appeared describing the use of a high-power toric intraocular lens for treatment of PMD.
The diagnosis of PMD and its distinction from keratoconus has been an ongoing discussion in the cornea and topography arena. For most, this is nothing more than an academic exercise with little clinical significance, because most view these two entities as different points on a clinical continuum. The distinction, regardless of whether it is real, becomes important when one advocates a specific treatment method that may not be applicable for both patient populations.
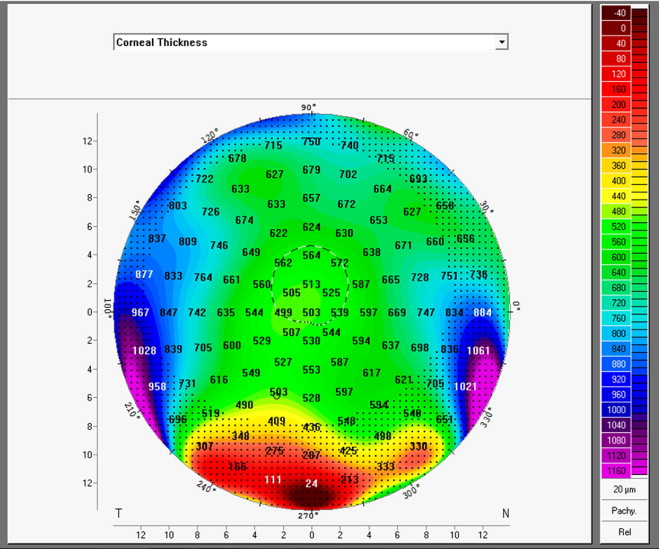
The use of curvature maps to diagnose PMD is limited and prone to artifact, and we have suggested the use of a full corneal thickness map to separate better these two entities. The classic description of PMD was a corneal thinning disorder characterized by an inferior band of thinning 1 to 2 mm from the inferior limbus associated with a flat vertical meridian and a sharp change in curvature or shape at or immediately above the band of thinning. A review of the preoperative thickness map in this article reveals typical findings fairly typical of keratoconus with central or paracentral apical thinning and no inferior band. This should be compared with the much rarer pattern seen in classic PMD, where there is a clear band of thinning running horizontally 1 to 2 mm from the inferior limbus ( Figure ).