Substantial evidence exists to support the concept that the respiratory system functions as an integrated unit. Pathophysiological processes that involve the upper airway generally occur in conjunction with lower airway diseases, and diffuse inflammation often affects mucosal surfaces of the middle ear, nose, sinuses, and tracheobronchial tree simultaneously. Support for this relationship can be found in epidemiological studies, in shared pathophysiological mechanisms, and in observed interactive treatment effects. This model and its implications are discussed.
Over the past decade there has been an increasing awareness of the interrelationship between inflammatory diseases of the upper and lower airway. Both epidemiological and physiological data suggest that the respiratory tract, from the middle ear mucosa, through the nose and sinuses, and into the pulmonary tree, behave as an integrated unit. Pathophysiological processes that affect one component of this integrated system often concurrently impact other portions of the airway, and over time, isolated disease in one area can expand to involve other areas also. This interdependence of the upper and lower respiratory tracts has been explored in numerous studies and clinical reviews, and has led to the concept of the unified airway, a model for understanding and framing inflammatory processes that affect the respiratory system.
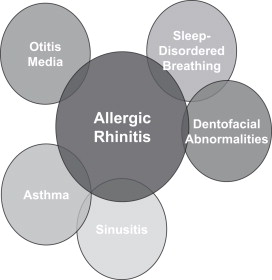
In this unified airway model, the respiratory tract is considered to be an integrated system and to behave as an organized, functional unit ( Fig. 1 ). Both local inflammatory processes and systemic mediators promote reactions throughout this system, and pathophysiological mechanisms activated by this inflammation can stimulate effects in all components of this unified airway. The presence and severity of disease processes within the upper and lower airways are linked closely, and exacerbations of disease in one component of the airway are likely to encourage worsening of airway disease diffusely .
The discussion of the relationship between the upper and lower airways has historical roots that go back almost a century. In 1920, Keller noted that among patients who had lower respiratory disease, 86% of those individuals also reported concurrent nasal symptoms. He observed that among patients who had nasal congestion, the decreased ability of the nasal airway to appropriately condition inspired air could lead to increased asthma symptoms such as wheezing and cough. From the 1920s through the 1980s, however, little was written on the relationship of nasal function and asthma, and certainly not in an attempt to integrate the behavior of these two components of the respiratory system.
The interest in the integrated function of the upper and lower respiratory tracts has increased in the past decade. In one recent international multidisciplinary consensus meeting, the interrelationship between the diseases of allergic rhinitis and asthma was examined thoroughly, and numerous epidemiological and pathophysiological links were found tying these two common conditions. In fact, the coexistence of these two processes was felt to be so frequent that this panel recommended that “when considering a diagnosis of rhinitis or asthma, an evaluation of both the upper and lower airways should be made” .
In examining the relationship between various disease processes, and in exploring the interrelationship between those processes, three criteria have been proposed that should be satisfied in order support this relationship . This model has been used in exploring both the relationship between chronic rhinosinusitis and gastroesophageal reflux disease , and the relationship between allergic rhinitis and chronic rhinosinusitis . This model also can be adapted to explore the relationship between upper and lower airway diseases. Three criteria in support of a unified airway would be:
- 1.
Patients with upper airway diseases such as rhinitis and rhinosinusitis should have a higher prevalence of lower respiratory diseases such as asthma; the corollary, increased prevalence of upper respiratory diseases among patients with lower respiratory diseases, also should be present.
- 2.
Interrelated pathophysiological mechanisms between upper and lower airway diseases should exist to explain the interaction of these two disease processes.
- 3.
Treatment of one portion of the unified airway should improve symptoms in a separate portion of the respiratory system.
These three principles will be explored throughout this issue, and can be used to evaluate the relevance of the unified airway model to otolaryngologists and other physicians. Some introductory comments will place the discussion into perspective, and will begin to examine these three principles in the integration of upper and lower airway disease.
Epidemiological relationships
Corren published a landmark paper examining the relationship between rhinitis and asthma. In this article, he not only looked at the coexistence of these two common respiratory diseases, but also discussed the temporal relationship of the onset of asthma, frequently preceded by the presence of allergic rhinitis. Corren noted that 78% of patients who have asthma are bothered with symptoms of rhinitis, both allergic and nonallergic. In addition, 38% of patients who have rhinitis have asthma, with the true prevalence perhaps being even higher. Corren emphasized this relationship again in a recent review, pointing out that recognition of the relationship between these two processes allows improved opportunities for treatment and prevention of respiratory disease.
A large-scale epidemiological study was conducted using a Danish general practice database to examine the temporal relationship between asthma and allergic rhinitis among patients presenting to primary physicians over a 1-year period . In this study, the history of almost 8000 patients who presented with one or both of these diseases was reviewed for the coexistence or preceding presence of upper and lower respiratory symptoms. Among this group of patients, both allergic rhinitis and asthma first developed within the same year in 25% of the sample. In addition, in more than 75% of these patients, the two diseases developed within 2 years of each other. This study would suggest that the development of respiratory symptoms in one part of the unified airway is linked closely with the expression of symptoms in another part of the airway, at least temporally.
Numerous examples of this epidemiological relationship can be cited. A Finnish twin cohort study examined 11,000 patients to evaluate whether the presence of allergic rhinitis would predispose patients to the development of asthma . In this 15-year study, patients who had allergic rhinitis had a fourfold increase of developing asthma when compared with a control population that was not allergic. Similar findings also were reported by Guerra in a large Tucson database and by Settipane with Brown University undergraduates . In each of these studies, individuals who had allergic rhinitis demonstrated a threefold increase in the development of asthma over a 20-year period when compared with their nonallergic counterparts. These longitudinal investigations all support the concept that inflammation in the upper airway can be a predisposing factor in the development of lower airway disease, and that the respiratory tract as a whole functions as a unified mechanism.
Pathophysiological mechanisms
Several mechanisms have been postulated to explain the observed relationship between diseases of the upper and lower airway. Several of these mechanisms are more of historical interest, although a growing body of evidence suggests that common inflammatory processes appear to be involved in diffuse airway inflammation. Three of these potential mechanisms include (1) the nasobronchial reflex, (2) the loss of nasal protection of the lower airway, and (3) shared inflammation throughout the respiratory tract.
The nasobronchial reflex
Argument for the presence of a nasobronchial reflex dates back almost a century, when Sluder proposed that nasal irritation could cause bronchospasm and lead to the development of bronchial asthma. This hypothesis led to a series of studies beginning in the 1960s that attempted to demonstrate the existence of this purported reflex. The study that often has been cited as providing primary support for this mechanism was conducted by Kaufman and Wright , and was reported in 1970. In this study, silica particles were applied directly to the nasal mucosa in subjects without asthma. Measurement of pulmonary function in these subjects was reported to demonstrate rapid and significant increases in lower airway resistance, leading to the speculation that a direct reflex was stimulated between the nose and the lungs. Subsequent studies showed that this effect could be blocked through the administration of atropine or with resection of the trigeminal nerve .
Since these experiments in the late 1960s, additional support for this presumed nasobronchial reflex has not been demonstrated. In fact, a series of studies cited in Corren’s 1997 review of the unified airway failed to replicate the effects of nasal stimulation in causing rapid bronchoconstriction. In addition, in animal models in which nasal stimulation has been conducted with thermal, chemical, and mechanical stimuli, no reflex changes in ventilation or oxygenation have been demonstrated . Although delayed changes can be seen in the lung from 30 minutes to four hours after antigen challenge of the nose , immediate reflex changes in pulmonary function cannot be demonstrated consistently. These findings suggest that mechanisms other than a direct reflex arc may be responsible for the observed relationship between upper and lower airway disease.
Loss of nasal protection of the lower airway
Another proposed mechanism that has been offered to explain changes in pulmonary function with nasal disease has been the loss of the protective function of the nose in situations of mouth breathing. The study often cited to support this hypothesis was reported by Shturman-Ellstein and colleagues in 1978. In this trial, patients who had exercise-induced asthma were allowed to exercise under three conditions: spontaneous breathing, nasal breathing, and mouth breathing. Results of this study demonstrated that not only did mouth breathing worsen bronchospasm among this group of subjects, nasal breathing appeared to have a protective effect. The conclusions would appear to suggest that nasal breathing can have a beneficial effect on the lower airway through conditioning inspired air for delivery to the lungs.
Despite the conclusions reported in this study, confirmation of this relationship has not been reported. In fact, recent studies suggest that stimulation of the nose with noxious challenges, such as cold, dry air, can improve the ability of the nasal mucosa to warm and humidify inspired air . In addition, occluding the nose in subjects with cat allergy was not shown to increase bronchospasm among these individuals . Again, the observed relationship between the upper and lower airways does not appear to be explained through a mechanism of nasal airway protection.
Shared inflammation
The primary hypothesis that links the upper and lower airways mechanistically employs a model of shared airway inflammation throughout the respiratory system. The respiratory mucosa in the middle ear, the nose and sinuses, and the lower respiratory tract is structurally and physiologically uniform, having a pseudostratified columnar epithelium that is involved in active transport of mucus and particulate matter. Disorders of the respiratory mucosa present with a similar inflammatory response, common to diverse diseases such as rhinitis, rhinosinusitis, and asthma . Inflammatory mediators released in diseases throughout this respiratory system are identical, and involve T cell cytokines such as interleukin (IL)-4, IL-5, and IL-13, and cellular populations, particularly eosinophils .
Studies by Braunstahl and colleagues have shown that stimulation of one portion of the airway mucosa with antigen will result in system-wide inflammatory changes within a matter of hours. Placement of antigen directly onto the bronchial mucosa using bronchoscopy has been shown to induce nasal inflammation in patients who have allergic rhinitis. In addition, reciprocal induction of bronchial inflammation with careful nasal antigen stimulation has been demonstrated using a similar model . These studies suggest that inflammatory crosstalk, or immune communication through the respiratory tract, is responsible for system-wide changes that induce an up-regulation of airway inflammation. Braunstahl discusses the concept as nasobronchial interaction .
Other studies confirm the interplay of inflammatory processes in the upper and lower airways. Inflammation throughout the respiratory system appears to be present in patients who have disease even isolated to one portion of the system. Significantly higher numbers of eosinophils can be seen in the nasal mucosa of asthmatic patients, even those who do not have any symptoms of rhinitis . Furthermore, nasal antigen challenge can increase bronchial hyper-responsiveness to methacholine challenge, even without the presence of unstimulated changes in pulmonary function . Ongoing antigenic stimulation of the respiratory tract therefore could provide a cumulative augmentation of airway inflammation, resulting in the observed progression of airway inflammation from allergic rhinitis to asthma.
Because both allergic rhinitis and asthma are inflammatory conditions of the airway, and because common pathophysiological processes appear to be involved in these two processes, it would appear that mechanistic support for the unified airway model is found in the observation of system-wide inflammatory airway effects. Inflammation appears to be the hallmark of chronic airway disease, and this inflammation does not appear to be limited to any one specific component of the respiratory system.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


