Purpose
To investigate the prevalence and incidence of glaucoma in a large health maintenance organization (HMO) in Israel.
Design
A population-based retrospective cohort study, conducted using electronic medical database.
Methods
Collected data included personal and medical characteristics. setting : Maccabi Healthcare Services, the second-largest HMO in Israel, insuring 2 million members and serving 25% of the population with a nationwide distribution. study population : Maccabi members from January 2003 to December 2010. main outcome measures : Prevalence and incidence of glaucoma according to the International Classification of Diseases, 9th revision, Clinical Modification diagnostic codes.
Results
A total of 15 708 prevalent glaucoma patients were identified among active members of Maccabi in December 2010. A total of 15 332 (97.6%) were 40 years or older, with a point prevalence of 2.2%. Prevalence of glaucoma was strongly associated with age, ranging from 0.28% at age 40–50 to 9.2% among elderly aged 80 or above. The 5 most prevalent diagnoses were open-angle glaucoma (1.61%), exfoliation glaucoma (0.20%), unspecified glaucoma (0.17%), angle closure (0.11%), and normal tension glaucoma (0.06%). We identified 6674 incident glaucoma patients diagnosed between 2003 and 2010. The observed incidence density rate among 40+-year-old members was 1.84 (1.79–1.88) new cases per 1000 person-years. Median age at diagnosis was 64 years old. The risk of glaucoma was similar between sexes up to age 70 years, and was significantly ( P < .01) higher in men in older ages.
Conclusions
Glaucoma affects nearly 10% of the elderly population in Maccabi, with the highest risk of diagnosis at age 70–74. Since glaucoma leads to irreversible vision loss, the present estimates of morbidity should be of significant concern.
Glaucoma is the second-leading cause of blindness worldwide, with a prevalence depending mainly on ethnicity and age. Owing to the aging population in the western world, glaucoma is expected to present a challenge to the health care system in terms of diagnosis and treatment. Glaucoma is a treatable disease in which irreversible optic nerve damage and progression can be prevented in most cases if diagnosed in time. Thus, assessing prevalence and incidence of this disease is crucial for the health care authorities in order to prepare strategic plans for early diagnosis, early prevention, and appropriate treatment of the disease.
There are over 50 population-based studies that determine the prevalence of glaucoma and only a few about incidence. These studies varied widely in terms of the eye examination methods and case definitions used, in particular the criteria adopted for defining glaucomatous nerve damage.
This study investigates the prevalence and incidence of glaucoma in Maccabi Healthcare Services, the second-largest Health Maintenance Organization (HMO) in Israel, insuring more than 2 million members. We are unaware of previous reports about the epidemiology of glaucoma in Israel. This study provides unique real-world data from a large, complete, and unselected population, providing important information about all types of glaucoma disease.
Methods
This population-based retrospective cohort study was conducted using the electronic medical database of Maccabi Healthcare Services, a large HMO in Israel. The study investigated the prevalence and incidence of all types of glaucoma in Maccabi. The study protocol was approved prospectively by the Assuta Health System’s institutional review board, located in Tel-Aviv, Israel.
Settings
The Israeli National Health Insurance Law, in effect since January 1995, sets forth the state’s responsibility to provide health services for all residents of the country. The law stipulates that a standardized basket of medical services will be supplied by health care organizations. The 4 nonprofit HMOs in Israel are publicly funded and are obligated to insure every citizen who chooses to join one of them, free of any preconditions and irrespective of age, sex, or medical history. Patients unable to afford copayments are not denied access; instead, government subsidies ensure that care is provided based on need, not ability to pay.
The study was conducted in Maccabi Healthcare Services, the second-largest HMO in Israel, insuring 25% of the total population with a nationwide distribution. Since the mid-1990s, all Maccabi Healthcare Services caregivers have been computerized and connected to the central database using the same system. Maccabi Healthcare Services databases contain longitudinal data on the entire membership population (currently, a population of 2 million individuals). All patients have a single national identity number, which enables access to information from other national databases. The membership is representative of the sex and age distribution of Israel (median age among Maccabi members is 31 years; in the general Israeli population: 33 years). There are 420 ophthalmology outpatient clinics in Maccabi, staffed by 300 senior ophthalmologists (approximately 50% of the nation’s registered ophthalmologists) that completed at least 5 years of ophthalmology residency and passed the Israeli board examinations. Of note is that in Israel treating eye diseases is exclusive to physicians, while other eye care givers, such as optometrists, are not allowed to diagnose and treat any ophthalmology problems.
Study Population
Included in the study were all patients that were diagnosed with glaucoma (ICD9-CM codes 365.1–365.9) in either 1 eye or both eyes between January 1, 2003 and December 31, 2010. The index date was defined as the first date of definite glaucoma diagnosis. To increase internal validity, case definition required at least 2 physician diagnoses on 2 separate visits as well as a referral for a visual field (VF) examination. Patients with the diagnosis of ocular hypertension or any other preglaucoma conditions were not included in the present study. All diagnoses observed in less than 1% of glaucoma patients (eg, glaucoma associated with disorders of the lens, glaucoma associated with other ocular disorders, congenital glaucoma, pigmentary glaucoma, glaucoma associated with ocular trauma, glaucoma associated with ocular inflammation, glaucoma plateau-iris, corticosteroid-induced, glaucoma associated with vascular disorders) were grouped into 1 category of “Other.” For data collection we used a personal identity number for a cross-linkage of Maccabi data sets to collect information on demographics, diagnosis, prescriptions, purchases, medical tests, and procedures, as well as visits to physicians including ophthalmologists.
Statistical Analysis
We examined frequency of visits to ophthalmologists among the general population in Maccabi to assess screening rates for glaucoma. Age- and sex-specific point prevalences of glaucoma among active Maccabi members were calculated for December 31, 2010. We have also calculated glaucoma incidence density rates for the years 2003–2010 after excluding members diagnosed with glaucoma prior to 2003 (n = 7395) as well as members with less than 5 years of continuous membership in Maccabi (n = 1759) before diagnosis, to ensure selection of newly developed cases.
For incident cases of glaucoma, only the time until diagnosis contributed to the number of patient-years at risk. The 5-year cumulative incidence rate was assessed using the following equation: 5-year incidence = 1 − e −5∗IR (IR is the incidence density rate and e is the base of the natural logarithm).
The observed incidence was also validated using Leske’s method for estimating incidence from prevalence in diseases that are irreversible and nonfatal. The association between increasing age and glaucoma was analyzed with χ 2 trend test and χ 2 independence test. SPSS software (version 19.0; SAS Institute, Cary, North Carolina, USA) supported the analyses.
Results
Among the general population of patients aged 40 or above in Maccabi, 43% visited an ophthalmologist at least once in the prior 2 years, 51% at least once in the prior 3 years, and 61% in the prior 5 years ( Table 1 ). The frequency of visits increased with age up to 85 years old. Women visited ophthalmologists more than men ( P < .01). Gonioscopy was documented and billed for at least 69% of patients.
| Age Group | At Least 1 Visit to Ophthalmologist | |||||
|---|---|---|---|---|---|---|
| Last 2 Years | Last 3 Years | Last 5 Years | ||||
| Men (95% CI) | Women (95% CI) | Men (95% CI) | Women (95% CI) | Men (95% CI) | Women (95% CI) | |
| 40–49 | 25.2% (24.9–25.4) | 33.0% (32.7–33.2) | 32.4% (32.1–32.6) | 41.5% (41.2–41.7) | 42.0% (41.7–42.2) | 52.3% (52.0–52.5) |
| 50–59 | 34.8% (34.5–35.1) | 43.4% (43.1–43.7) | 43.6% (43.3–43.9) | 52.9% (52.6–53.2) | 54.6% (54.3–54.9) | 63.9% (63.6–64.2) |
| 60–69 | 51.6% (51.3–52.0) | 59.3% (58.9–59.6) | 61.0% (60.6–61.3) | 68.8% (68.4–69.1) | 69.9% (69.5–70.2) | 77.3% (77.0–77.6) |
| 70–79 | 66.2% (65.7–66.8) | 69.6% (69.1–70.0) | 75.6% (75.1–76.0) | 78.3% (77.9–78.7) | 82.1% (81.7–82.5) | 84.9% (84.5–85.2) |
| 80–84 | 67.3% (66.2–68.4) | 64.4% (63.4–65.3) | 77.2% (76.3–78.1) | 75.4% (74.6–76.2) | 84.8% (84.0–85.5) | 83.7% (83.1–84.4) |
| 85+ | 58.8% (57.4–60.2) | 50.4% (49.4–51.5) | 71.5% (70.4–72.6) | 63.4% (62.5–64.3) | 80.7% (79.7–81.6) | 75.4% (74.6–76.2) |
| Total 40+ | 37.9% (37.7–38.0) | 45.6% (45.5–45.8) | 46.9% (46.7–47.1) | 55.3% (55.2–55.5) | 56.4% (56.2–56.6) | 65.3% (65.1–65.4) |
Glaucoma Prevalence
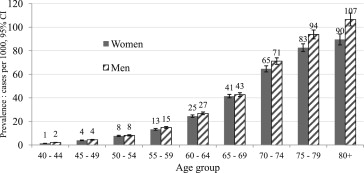
A total of 15 708 glaucoma patients were identified among active members of Maccabi ( Table 2 ). A total of 15 332 (97.6%) of these patients were aged 40 years or above, with a point prevalence of 22 cases per 1000. Figure 1 shows the age- and sex-specific prevalence. Prevalence did not differ by sex, and was strongly and significantly ( P trend < .01) associated with increasing age, ranging from 3 cases per 1000 at age 40–50 to 92 per 1000 at age 80+.
| N | % of Total | |
|---|---|---|
| Age | ||
| <40 | 376 | 2% |
| 40–45 | 255 | 4% |
| 45–49 | 498 | 3% |
| 50–54 | 813 | 5% |
| 55–59 | 1289 | 8% |
| 60–64 | 2156 | 14% |
| 65–69 | 1897 | 12% |
| 70–74 | 2896 | 18% |
| 75–79 | 2333 | 15% |
| 80+ | 3195 | 20% |
| Total | 15 708 | 100% |
| Sex | ||
| Women | 8149 | 52% |
| Men | 7559 | 48% |
| Total | 15 708 | 100% |
| Diagnosis year | ||
| <2003 | 7572 | 48% |
| 2003–2006 | 3725 | 24% |
| 2007–2010 | 4411 | 28% |
| Total | 15 708 | 100% |
| Pathology | ||
| Open-angle | 11 120 | 71% |
| Exfoliation glaucoma | 1368 | 9% |
| Unspecified glaucoma | 1200 | 8% |
| Angle closure | 743 | 5% |
| Low-tension glaucoma | 391 | 2% |
| Other | 886 | 6% |
| Total | 15 708 | 100% |
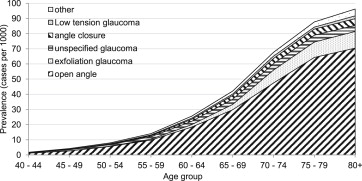
The prevalence of all glaucoma types increased with age. The 5 most prevalent glaucoma types among the Maccabi population aged 40 or older were open-angle glaucoma (OAG), exfoliation glaucoma (XFG), unspecified glaucoma, angle closure glaucoma, and normal tension glaucoma (NTG), with prevalence rates of 16.1, 2.0, 1.7, 1.1, and 0.6 cases per 1000, respectively ( Figure 2 ). The prevalence rate of OAG increased from 1 case per 1000 at age 40–44 to 70 cases per 1000 at age 80+. XFG prevalence rate increased dramatically with age, rising from 0.02 cases per 1000 at age 40–50 to 11 cases per 1000 at age 80+, and among patients aged 65+ this is the second most prevalent glaucoma type (after OAG). OAG comprised 71% of all glaucoma cases, with a similar proportion in all age groups ( Table 3 ). XFG, the second most prevalent type of glaucoma, rarely appeared before 50 years of age and its proportion of all glaucoma cases increased with age up to 12%–13% at 70 years or older.
| Open Angle | Exfoliation Glaucoma | Unspecified | Angle Closure | Low Tension Glaucoma | Other | P Value a | |
|---|---|---|---|---|---|---|---|
| <40 | 51% | 0% | 14% | 2% | 4% | 29% | <.001 |
| 40–44 | 67% | 1% | 14% | 1% | 5% | 12% | |
| 45–49 | 63% | 0% | 17% | 4% | 4% | 11% | |
| 50–54 | 71% | 1% | 13% | 4% | 4% | 7% | |
| 55–59 | 70% | 4% | 11% | 5% | 3% | 6% | |
| 60–64 | 72% | 6% | 9% | 5% | 3% | 5% | |
| 65–69 | 71% | 8% | 8% | 6% | 2% | 5% | |
| 70–74 | 70% | 13% | 6% | 5% | 2% | 4% | |
| 75–79 | 73% | 12% | 5% | 4% | 2% | 4% | |
| 80+ | 73% | 12% | 4% | 4% | 2% | 5% |
a P value for association between age and glaucoma type was computed after collapsing age groups <40 with 40–44 and 45–49, owing to small (<5) number of exfoliation glaucoma cases at these ages.
Incidence
We identified a total of 6674 incident glaucoma patients who were first diagnosed between 2003 and 2010. Ninety-three percent of our incident cases had a normal eye examination prior to the eye examination at the time of diagnosis. The observed incidence density rate of definite glaucoma (not including ocular hypertension and probable glaucoma) among 40+-year-old members was 1.84 (95% CI: 1.79–1.88) per 1000 person-years ( Table 4 ). The incidence density rate without VF referral was 2.64 per 1000 person-years. Median age at diagnosis was 64 years. Figure 3 shows the age- and sex-specific incidence density rates. The risk of glaucoma was similar between sexes up to age 70 years, and is significantly ( P < .01) higher in men in older ages. Stratification by type of glaucoma pathology showed significantly increased risk for men in OAG as well as XFG ( Figure 4 ). A decline in incidence was observed in both sexes starting from age 75 years old. The decline is non-statistically significant in men but significant in women aged 75–79 vs women aged 70–74 years old ( P < .01). Table 5 details the distribution of glaucoma types among incident cases by age.
| Age Group (y) | No. of Cases | Person-Years at Risk | Incidence Density Rate | 5-Year Incidence (%) | 1-Year Incidence (%) | |
|---|---|---|---|---|---|---|
| Men | <40 | 140 | 4 440 527 | 0.03/1000 | 0.016% | 0.003% |
| 40–44 | 141 | 396 216 | 0.36/1000 | 0.178% | 0.036% | |
| 45–49 | 194 | 337 543 | 0.57/1000 | 0.287% | 0.057% | |
| 50–54 | 323 | 304 195 | 1.06/1000 | 0.530% | 0.106% | |
| 55–59 | 468 | 217 859 | 2.15/1000 | 1.068% | 0.215% | |
| 60–64 | 543 | 139 974 | 3.88/1000 | 1.921% | 0.387% | |
| 65–69 | 545 | 111 303 | 4.90/1000 | 2.419% | 0.488% | |
| 70–74 | 541 | 68 818 | 7.86/1000 | 3.854% | 0.783% | |
| 75–79 | 295 | 39 672 | 7.44/1000 | 3.650% | 0.741% | |
| 80+ | 165 | 29 019 | 5.69/1000 | 2.803% | 0.567% | |
| Women | <40 | 117 | 4 645 681 | 0.03/1000 | 0.013% | 0.003% |
| 40–44 | 128 | 416 821 | 0.31/1000 | 0.153% | 0.031% | |
| 45–49 | 215 | 364 164 | 0.59/1000 | 0.295% | 0.059% | |
| 50–54 | 293 | 337 927 | 0.87/1000 | 0.433% | 0.087% | |
| 55–59 | 446 | 242 590 | 1.84/1000 | 0.915% | 0.184% | |
| 60–64 | 514 | 161 489 | 3.18/1000 | 1.579% | 0.318% | |
| 65–69 | 599 | 129 770 | 4.62/1000 | 2.281% | 0.461% | |
| 70–74 | 521 | 85 217 | 6.11/1000 | 3.011% | 0.610% | |
| 75–79 | 305 | 66 702 | 4.57/1000 | 2.260% | 0.456% | |
| 80+ | 181 | 48 864 | 3.70/1000 | 1.835% | 0.370% | |
| Overall | <40 | 257 | 9 086 208 | 0.03/1000 | 0.039% | 0.003% |
| 40–44 | 269 | 811 105 | 0.33/1000 | 0.348% | 0.033% | |
| 45–49 | 409 | 701 707 | 0.58/1000 | 0.576% | 0.058% | |
| 50–54 | 616 | 642 121 | 0.96/1000 | 0.925% | 0.096% | |
| 55–59 | 914 | 460 449 | 1.99/1000 | 1.786% | 0.198% | |
| 60–64 | 1057 | 301 462 | 3.51/1000 | 2.809% | 0.350% | |
| 65–69 | 1144 | 241 073 | 4.75/1000 | 3.928% | 0.473% | |
| 70–74 | 1062 | 154 035 | 6.89/1000 | 5.724% | 0.687% | |
| 75–79 | 600 | 106 374 | 5.64/1000 | 6.012% | 0.562% | |
| 80+ | 346 | 77 882 | 4.44/1000 | 7.516% | 0.443% | |
| Total | 6674 | 12 582 419 | 0.53/1000 | 0.513% | 0.053% | |
| Total among 40+ | 6417 | 3 496 211 | 1.84/1000 | 1.734% | 0.183% | |
| Total among 55+ | 5123 | 1 341 277 | 3.82/1000 | 3.538% | 0.381% |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


