Purpose
To estimate the expected incremental lifetime cost of treatment of keratoconus compared to the expected cost of the treatment of myopia.
Design
Cost estimate from the patient’s perspective using a Markov decision model.
Methods
We modeled a hypothetical cohort of people with clinically significant incident keratoconus as defined by the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) Study. We included costs of clinic visits, fitting fees, contact lenses, surgical procedures, and complications. Survival curves of corneal transplants and associated complications were modeled using data from the 2007 Australian Graft Registry. Medical treatment regimens after surgery were defined by expert opinion.
Results
The expected value of the lifetime cost of the treatment of keratoconus over myopia was $25 168 with a standard deviation of $16 247 and a median of $17 596. The factors that most influenced the lifetime cost were the probability of initial corneal transplant and a subsequent regraft. The cost of routine care had relatively little influence on the lifetime cost of care.
Conclusions
The expected lifetime cost of treatment of keratoconus represents a significant cost to patients and payors. While the cost of routine care for keratoconus is not trivial, the primary factor influencing changes in the cost of care for keratoconus is the probability of corneal transplant. Combined with the significantly impaired vision-related quality of life and the relatively young onset of disease, the economic burden of the treatment of keratoconus represents a significant public health concern.
Keratoconus is described as a noninflammatory, progressive ectasia of the cornea leading to a conical protrusion of the cornea and progressive, myopic, irregular astigmatism. The presentation is typically bilateral but asymmetric. The incidence has been reported to be approximately 1 in 2000, and the prevalence is estimated to be 54.5 per 100 000. Keratoconus has a significant impact on vision-related quality of life (VRQoL), with a substantial number of keratoconus patients experiencing a continuing decline in their VRQoL over time. Since the onset of keratoconus is typically in puberty or early adulthood with continuation of the disease into prime earning and child-rearing years, this loss of quality of life represents an important public health burden.
Early in the disease, glasses or soft contact lenses may correct the vision adequately, but as the disease progresses, rigid gas-permeable contact lenses are considered the treatment of choice. Ultimately, 15% to 60% of keratoconus patients undergo penetrating keratoplasty (PK) when contact lenses become intolerable or can no longer provide adequate visual correction. In 2004, keratoconus accounted for 15.1% of the more than 30 000 corneal transplants performed in the United States.
While previous studies focused on the clinical characteristics of keratoconus and its impact on quality of life, there have been no studies concerning the economic burden this chronic disease represents for patients and payors. In this paper, we estimate the lifetime economic burden of keratoconus in terms of medical services using a decision analytic method.
Methods
We constructed a Markov decision model using TreeAge Pro (Version 1.0.2; Williamsport, Massachusetts, USA) to estimate the overall cost to a person with clinically significant keratoconus. We assumed that the simulated cohort had baseline characteristics similar to those of patients in the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) Study. This was a 16-center, longitudinal observational study of 1209 patients with keratoconus. The characteristics of the patients enrolled in the CLEK Study and its findings have been described in detail elsewhere.
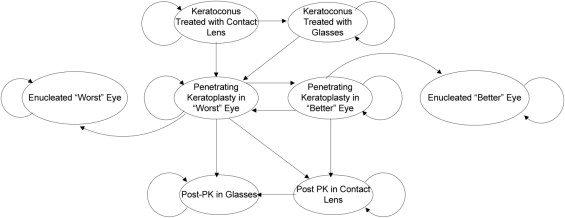
The Markov model is an analytic tool that allows an investigator to estimate the costs and consequences of a disease process. A cohort of people with a particular condition is subjected to recurring risks and costs over a period of time, representing a “Markov cycle.” In this model, each cycle represents 1 year after the diagnosis of clinically significant keratoconus. In each cycle, a proportion of the cohort die of causes not related to keratoconus, according to published census estimates. The remaining cohort members experience events typically encountered by people with keratoconus—for example, development of contact lens discomfort, a change in prescription, a switch to glasses, or ultimately, a corneal transplant. The probability that these events occur is taken from the CLEK Study or published sources. A simplified bubble diagram representation can be seen in the Figure .
We estimated the Markov model using a microsimulation approach. This approach allows us to assume that the Markov cohort is heterogeneous and that each cohort member could experience disparate events. The “cohort participants” were randomly assigned characteristics based upon the expected distribution in the CLEK Study sample. Participants then proceeded through the model on an individual basis. Relying on the data from the CLEK Study, each “participant” is permitted the opportunity to face a worsening of his or her disease (ie, a worsening of corneal steepness or visual acuity). The probability of this is assigned by a random function based upon the binomial distribution (ie, if there was a 40% probability that there will be a 1-diopter steepening of the cornea in a year, then there is a 40% chance that the “participant” would face a worsening of disease). In estimating the model, we used a 2-stage process. We began with a set of model parameters and had a simulated cohort of 1000 participants proceed through them. We then re-sampled the model parameters (each from an a priori distribution) and had the cohort proceed through the model again using the new set of parameters. We continued this process for 500 re-samplings, with all 1000 participants proceeding through the model each time, for a total of 500 000 iterations.
Modeling the Costs of the Treatment of Keratoconus Over a Patient’s Lifetime
We assumed that all persons entering the model had clinically significant keratoconus in both eyes as defined by the CLEK Study and had not had a previous PK in either eye. Reflecting the CLEK sample, the majority (96.5%) of patients were assumed to have been initially treated primarily with contact lenses, with the rest being treated only with glasses. The probability of the need for a penetrating keratoplasty in a given year was estimated using logistic regression and previously published predictors (corneal curvature, high-contrast best-corrected visual acuity, contact lens comfort, and age). We assumed that the “worse” eye would be the first to require a surgical procedure. In addition, we assumed that the maximum number of corneal transplants that a person could receive would be 5, following the evidence provided in the 2007 Australian Graft Registry.
To estimate the cost of an annual examination, fitting, and contact lenses we conducted a survey of the CLEK Study clinics. Six of 22 clinics (27%) responded to the survey, a copy of which can be found in the Technical Appendix to this report (Supplemental Material available online at AJO.com ). Based upon the reports from CLEK participants, we assumed that a patient with vision or contact lens comfort issues would see an eye care practitioner up to 3 times over the course of a year.
Participants Undergoing Penetrating Keratoplasty
Survival curves based on the 2007 Australian Graft Registry were constructed to estimate the expected length of graft survival after PK and the probability of associated complications. In the model, we began by assuming that a PK was performed on only one eye each year and that the annual probability was based upon the risk factors identified in the CLEK study. We further assumed that the PK was performed only on the eye with the worst visual acuity or highest corneal curvature. Once the PK was completed, we assumed that the previous “worst” eye became the “best” and vice versa, so the probability of a contralateral transplant was then based upon the characteristics of the new “worst” eye.
The probability of rejection was based upon the Graft Registry survival curves, and serial regrafts were performed based upon the probability of rejection from that source. Other complications that could arise from a PK included a rise in intraocular pressure (IOP) or a pooled “other” category. Unique survival curves to each graft were used depending on which complication, if any, occurred.
For patients who underwent PK, the primary health states they enter are defined by the form of correction they experience following healing: glasses or contact lens. All patients began in the “post-PK contact lens” state and progressed to glasses if they became contact lens intolerant. As can be seen in the Figure , we also include a health state for enucleation. This is only included in the model for the sake of completeness. No “participants” enter this health state during the first cycle, as it is reserved for those patients who experience serial rejection of grafts and require multiple regrafts. We assumed a possibility of 1% on regrafts that the surgeon and patient would determine that future grafts are futile and choose to remove the eye. Note of course that the possibility of this occurrence is far less than 0.5%.
Incremental Costs
Our basis for assessing excess cost was comparison to the cost of treating a typical myopic patient. Thus the costs of correction with glasses or soft contact lenses or annual eye care visits were not included in the estimates of the cost of keratoconus. Costs of procedures were determined by using Medicare allowable for physician and anesthesia codes from the Healthcare Common Procedure Coding System, ambulatory surgery center fees, and appropriate medical treatment. We relied on expert opinion to establish regimens of medications and durations of procedures. The costs of drugs and duration were assumed to be the average wholesale price. Costs were discounted at a rate of 3%.
The influence of model assumptions on the estimate of lifetime costs of care for keratoconus was tested using 1-way sensitivity analysis. The perspective in these analyses was that of the payor. We did not distinguish whether the payor was the patient or an insurer. The consequence of this perspective is that only direct medical expenses are reported. We did not consider loss of productivity or the impact of the disease on quality of life. A more detailed explanation of the methods and assumptions can be found in the Technical Appendix (Supplemental Material available online at AJO.com ).
Results
The results of the model are summarized in Table 1 . Over average disease duration of 37 years, providing care for a person with keratoconus cost $24 168 more than providing care for a person with myopia. Over half of this ($13 944) is the expected cost of undergoing PK and addressing the postsurgical complications. The expected cost of regular ophthalmologic or optometric care was $10 224, or 42.3% of the total cost of care.
| Mean | Median | Standard Deviation | |
|---|---|---|---|
| Total cost | $24 168 | $16 247 | $17 596 |
| Cost of nonsurgical treatment | $10 224 | $9987 | $2732 |
| Age of death (years) | 77 | 77 | 0.37 |
| Time with disease (years) | 37 | 37 | 0.4 |
| Number of penetrating keratoplasties in worse-seeing eye | 1.14 | 0.48 | 1.15 |
| Number of penetrating keratoplasties in better-seeing eye | 0.43 | 0 | 0.9 |
Probabilistic Sensitivity Analyses (Second Order Monte Carlo Simulation)
The results of our sensitivity analyses are provided in Table 2 . We tested those parameters that were thought to have significant influence over the total lifetime cost of keratoconus.
| Parameter | Base Case Value of Parameter | Parameter Value in Sensitivity Analysis | Percentage Change Lifetime Cost from Baseline |
|---|---|---|---|
| Cost of 1 contact lens | $111 | $18 | (17%) |
| $300 | 30% | ||
| Cost of penetrating keratoplasty | $7600 | $6800 | 1% |
| $10000 | 18% | ||
| Discount rate | 3% | 1% | 58% |
| 5% | (25%) | ||
| Probability of complication after penetrating keratoplasty | 48% | 25% | (3%) |
| 75% | 7% | ||
| Probability of regraft | Function | 20% | 5% |
| 0% | (23%) | ||
| Yearly probability of requiring a penetrating keratoplasty | Function | 1% | (15%) |
| 10% | 212% |
The parameters that have the greatest influence on the lifetime cost of keratoconus are the probability of requiring a PK and the discount rate used in the model. Relatively small changes in each of these parameters result in a change in the lifetime cost in excess of 50%. Of course, of these only the probability of PK has clinical significance.
In the base case analysis, we found that, on average, a person with keratoconus required approximately 1.6 PKs over his or her lifetime and had a median of approximately 0.5 PK. The Australian registry data, which reported a median corneal graft survival for a keratoconus patient as 19 years, appears quite similar to data from a recent US study.
Results
The results of the model are summarized in Table 1 . Over average disease duration of 37 years, providing care for a person with keratoconus cost $24 168 more than providing care for a person with myopia. Over half of this ($13 944) is the expected cost of undergoing PK and addressing the postsurgical complications. The expected cost of regular ophthalmologic or optometric care was $10 224, or 42.3% of the total cost of care.
| Mean | Median | Standard Deviation | |
|---|---|---|---|
| Total cost | $24 168 | $16 247 | $17 596 |
| Cost of nonsurgical treatment | $10 224 | $9987 | $2732 |
| Age of death (years) | 77 | 77 | 0.37 |
| Time with disease (years) | 37 | 37 | 0.4 |
| Number of penetrating keratoplasties in worse-seeing eye | 1.14 | 0.48 | 1.15 |
| Number of penetrating keratoplasties in better-seeing eye | 0.43 | 0 | 0.9 |
Probabilistic Sensitivity Analyses (Second Order Monte Carlo Simulation)
The results of our sensitivity analyses are provided in Table 2 . We tested those parameters that were thought to have significant influence over the total lifetime cost of keratoconus.
| Parameter | Base Case Value of Parameter | Parameter Value in Sensitivity Analysis | Percentage Change Lifetime Cost from Baseline |
|---|---|---|---|
| Cost of 1 contact lens | $111 | $18 | (17%) |
| $300 | 30% | ||
| Cost of penetrating keratoplasty | $7600 | $6800 | 1% |
| $10000 | 18% | ||
| Discount rate | 3% | 1% | 58% |
| 5% | (25%) | ||
| Probability of complication after penetrating keratoplasty | 48% | 25% | (3%) |
| 75% | 7% | ||
| Probability of regraft | Function | 20% | 5% |
| 0% | (23%) | ||
| Yearly probability of requiring a penetrating keratoplasty | Function | 1% | (15%) |
| 10% | 212% |
The parameters that have the greatest influence on the lifetime cost of keratoconus are the probability of requiring a PK and the discount rate used in the model. Relatively small changes in each of these parameters result in a change in the lifetime cost in excess of 50%. Of course, of these only the probability of PK has clinical significance.
In the base case analysis, we found that, on average, a person with keratoconus required approximately 1.6 PKs over his or her lifetime and had a median of approximately 0.5 PK. The Australian registry data, which reported a median corneal graft survival for a keratoconus patient as 19 years, appears quite similar to data from a recent US study.
Discussion
We are aware of no other previous work attempting to quantify the lifetime economic burden of keratoconus. We must look at other papers on the economic impact of visual impairment to put these findings in context. In a recent report, Rein and associates estimated the economic impact of visual problems in 2007 as $51.4 billion. Their work focused on 5 vision-related diseases—age-related macular degeneration, cataract, diabetic retinopathy, glaucoma, and refractive error—for 2 age groups: 40 to 64 years, and 65 years and older. As keratoconus usually manifests in young adults, we might reference our findings to refractive errors within the younger group. Not surprisingly, as this is the condition with the highest prevalence, refractive error had an annual cost of $3.67 billion. The authors estimated that approximately 18 000 000 people are treated for refractive error, which makes the average annual individual cost $200. This is in contrast to our annual cost of $653 for keratoconus. Keep in mind that our estimate was over and above the cost of the routine vision care.
Our estimate had extremely high uncertainty associated with it. This was seen in both our large standard deviation and the sensitivity of our estimate to the need for a PK. This variation in yearly cost makes it difficult for keratoconus patients to budget for the treatment of the disease and increases the need for health insurance coverage for the condition. It is precisely to address such uncertainty that medical insurance is purchased, and it is an important benefit for people with keratoconus. The cost of PK and follow-up to surgery is covered under most major medical policies, and in many cases the cost of routine care is as well. However, as keratoconus is a long-term chronic condition, this means that patients with the disease must face restrictions due to pre-existing conditions. This is yet another stress associated with their condition that people with keratoconus must face, and one that might be resolved with the recent passage of the Patient Protection and Affordable Care Act, which restricts exclusions due to pre-existing conditions.
We found that the factors that have the greatest influence on cost were the annual risk of a PK and the discount rate. In our model the annual risk of PK was estimated based upon data from the CLEK Study and the Australian Graft Registry. On a whole, the average incidence of PK among CLEK participants was approximately 2%. Not surprisingly, we found that increasing this to 10% substantially increased the lifetime cost of care and that reducing it to 1% significantly reduced this cost, although it seems unlikely that either of these extremes represents the “true” population incidence of PK among people with keratoconus. Similarly, we found that onset of clinically significant disease at age 18 substantially increased lifetime costs, resulting from the higher probability of early PK reflected in the model and the study population. It is true that diagnosis of keratoconus in early life is common, but it was found that with CLEK participants aggressive treatment was postponed until later in life. While changes in the discount rate influenced the overall costs, this reflects the choice of policymakers rather than clinicians or investigators. A 3% rate is that recommended by most authorities in the United States, and the sensitivity to this rate reflects the value placed on future health benefits. Should policymakers choose to place a lower value on future health than is typically seen today, the cost of keratoconus will not be viewed as more important than diseases with more proximal impact. Should the opposite be true, then keratoconus would increase in public health importance.
One of the greatest limitations of the model is the estimated age of diagnosis of clinically significant keratoconus of a patient. We assumed that the age of onset was the average age of the enrolled patients in the CLEK Study at 40.2 years. At first glance, this may appear too old an age of onset given that the first manifestations of keratoconus can occur as early as puberty; however, the patients that we attempted to model were those with clinically significant disease and not those with only the first manifestations that are easily treated with rigid contact lenses. The patients in the CLEK Study would also have a much higher probability of early PK than a group with a much earlier age of onset, so we decided to use the average age of individuals in the study. It is of course true that an earlier manifestation of the disease results in significant cost to a patient, representing nearly double the estimated lifetime cost.
The second limitation is the lack of other literature to determine external validity of our model. We make assumptions in the model based on parameters obtained from the literature, physician consultations, and our own estimations; however, whether this economic model truly follows the natural history of the disease remains to be seen. In the interim, it is up to the reader to determine the face validity of our model and estimates. Similarly, our model did not consider alternative treatments for advanced disease such as Intacs corneal implants, Descemet stripping endothelial keratoplasty, and collagen cross linking. We did not include these options as data on cost, effectiveness, and long-term consequences of these procedures is not currently available. As such evidence does enter the literature, it will be possible to use our model as a basis for determination of the economic impact of these innovations. Finally, we relied on Australian data for estimating graft survival. There are unfortunately no American studies of similar magnitude. Interestingly, the survival rates of corneal grafts for keratoconus were lower in a recent small-scale study in Iowa. By taking the approach we did, we took a more conservative approach to cost estimation, and also relied on the strongest possible evidence.
With a mean lifetime cost of $25 168, it can be seen that the cost of care for keratoconus represents a major burden to people with the condition and their insurers. When combined with the impact of keratoconus on VRQoL, we can see that this chronic disease presents a major burden to those who suffer from it, in spite of its limited impact on quality of life. In addition to the clinical and biological interest this disease presents to investigators, future studies should also focus on reducing these twin burdens borne by people with the disease.
The CLEK Economic Evaluation Project was supported by a grant from the National Eye Institute ( 1 R03 EY017150-01 , PI: Kymes). The Department of Ophthalmology at Washington University School of Medicine benefits from an unrestricted grant from Research to Prevent Blindness , New York, New York, and a core grant from the National Eye Institute , Bethesda, Maryland. Dr Kymes receives consulting fees from Allergan, Genentech, Pfizer, and TreeAge Software. Involved in conception and design (R.R., S.K., J.W., M.G.); analysis and interpretation (R.R., S.K., J.W.); writing the article (R.R., S.K.); critical revision of the article (S.K., J.W.); final approval of the article (R.R., S.K., J.W., M.G.); data collection (R.R., S.K., J.W., M.G.); provision of materials, patients, or resources (R.R., S.K., M.G.); statistical expertise (S.K., M.G.); obtaining funding (S.K., M.B.); literature search (R.R., J.W.); and administrative, technical, or logistical support (S.K., M.G.). The Washington University Human Research Protection Office (HRPO) reviewed this project and determined that it does not involve activities that are subject to Institutional Review Board (IRB) oversight. The Declaration of Helsinki and all U.S. federal laws as well as Missouri state laws were adhered to while conducting this project.
The authors gratefully acknowledge the assistance of Dr Andrew Huang for his advice on penetrating keratoplasty.
The Lifetime Economic Burden of Keratoconus: Technical Appendix
The purpose of this appendix is to provide the details of the model used in our paper. With this information, a reader should be able to replicate the model when given the same data. For others, it should also provide insight into how the results were obtained. If this is deemed insufficient to a reader, questions should be directed to kymes@vrcc.wustl.edu . A copy of the decision tree (in TreeAge Pro format) is available by request to kymes@vrcc.wustl.edu .
Definition of Eye 1 and Eye 2
In order to keep track of both eyes in the model, “Eye 1” was defined as the worst eye (ie, the eye most likely to get a penetrating keratoplasty [PK]) and the first to get the PK. “Eye 1” was also always the eye with the oldest PK. Eye 2 was defined as the eye with a better visual acuity (VA), lower corneal curvature, and better contact lens comfort in year 0. It was also always the second to require a PK. When a regraft was performed in “Eye 1” and when a PK was performed in “Eye 2,” “Eye 1” would become “Eye 2” since it was now the most recent PK. When an enucleation was performed in the model, the eye that was enucleated was defined as “Eye 2.” All parameters and trackers in the model follow these definitions and contain either a “1” or “2” in the parameter name to represent the corresponding eye. For example, “Years_PK1” tracks the number of years since a PK has been performed in “Eye 1.” However, if “Eye 1” becomes “Eye 2” after a regraft in “Eye 1,” the value of “Years_PK1” is transferred to “Years_PK2.”
Logic of Model
The Markov model in TreeAge Pro was created to determine the overall cost to a patient with clinically significant keratoconus over his or her lifetime. There are 13 health states in the model. Although the model is set to run for 50 years, the mean survival of a patient is approximately 37 years, which is appropriate given that the average age of the Collaborative Longitudinal Evaluation of Keratoconus (CLEK) Study was 40.2 years (Kymes, unpublished CLEK data, 2008). In all but the last health state, “Death,” the first decision is whether the person lives or dies. At the beginning of each cycle, the tracker variables, Age, curvature1, curvature2, comfort1, comfort2, VA1, and VA2, all progress according to preset parameters. The details of these can be seen in the section “Parameters obtained from the CLEK data.” In the post-PK health states, these parameters change with each cycle, but the values become irrelevant to the costs and probabilities in the model as they are only used in predicting the first PK. Also, throughout the model branches were kept to a maximum of 2 to make it easier to create distributions around probabilities. The PK is always performed at the beginning of the cycle.
Initial States
The first 2 health states, “Contact lenses (CL)” and “Glasses,” are where the cohort begins. The proportions that go into either are described in the section “Parameters obtained from the CLEK data.” Subsequently, based on the parameters of age, comfort (if wearing contact lenses), curvature, high contrast, best-corrected visual acuity, and the yearly changes of these as determined by Gordon and associates, 1 the person may require a PK. Finally, if the person was in the “Contact Lenses” health state, he or she will be fitted up to 3 times, which only 10% of the CLEK participants exceeded in a given year (Kymes, unpublished CLEK data, 2008). If unable to be fitted, the person will move to the “Glasses Only” health state. If a person is in the glasses health state, the patient is assumed to be unable to be fitted with contact lenses and will go back to the “Glasses Only” health state if the person does not undergo a PK.
PK in Eye 1 States
The next 2 health states are “PK in Eye 1” and “PK in Eye 1 wearing glasses.” These are 2 surgical health states and assume that the person is undergoing a PK in Eye 1 at the beginning of the year. The former health state assumes the person can currently be treated with contact lenses, and the latter assumes that the person can be treated with glasses only. The first complication encountered is enucleation, which is assumed to be a possible complication only after the first regraft. When an enucleation takes place, all values associated with Eye 1 are transferred to Eye 2 as described above in the “Definition of Eye 1 and Eye 2.”
The next branch is refractive surgery, which has been shown to be protective of grafts in the first year. 2 A tracker, “refraction,” is set to 1, and an associated modifier is applied to subsequent survival rates through the year. Subsequently, a person can have a complication. The order of complications is “rejection,” “rise in intraocular pressure (IOP),” and “Other complication.” Tracker values are applied if the complications took place. The person then had the option of undergoing a regraft of the same eye. The survival of the graft was based upon which complication, if any, had occurred as defined by the tracker variable. If there was a rise in IOP, glaucoma surgery was another branch, assuming there was no regraft performed on the eye. As in the previous 2 health states, a patient was fitted up to 3 times with contact lenses in the contralateral eye unless the patient was wearing glasses only. If there had been a regraft performed, the person would go back to the “PK in Eye 1” health states. If not, the person would continue on to the “Post-PK in Eye 1” states.
Post-PK in Eye 1 States
These 2 states are identical in logic to the initial health states except that after the “No death” branch, there is a branch for “Regraft of Eye 1.” The regraft proportion is based upon which, if any, complications had been present and how many prior grafts had been performed. 2 If there is no regraft in Eye 1, there is a branch for a PK in Eye 2 that is based on the same parameters as for Eye 1 but with values unique to this eye. We assumed that there would not be 2 PKs performed in a given year, and that a surgery would be performed in Eye 1 first. If there is no PK, contact lenses could again be fitted up to 3 times in Eye 2 if in the “Post-PK in Eye 1” state and not the “Post-PK in Eye 2 Wearing Glasses” state.
Enucleation Post-PK in Eye 2 States
These 2 states represent a person who has had an enucleation in Eye 2 but no surgery in Eye 1. The health states are identical to the initial health state except that the terminal nodes return to these 2 health states if a PK is not performed that year. If a PK is to be performed, the person goes to the health state of “Enucleation in Eye 2 and With New PK/Regraft in Eye 1,” which is where a person has had an enucleation in Eye 2 but is now having a PK in the other eye, Eye 1.
PK in Eye 2 State
This health state represents a year in which a person has had a PK in Eye 1 and is now getting a PK or regraft in Eye 2. It should be noted that Eye 2 could have been Eye 1 at one point, but since it is now the eye with the most recent PK, it is defined as Eye 2. This health state is identical to the “PK in Eye 1 Wearing Glasses” state, with a few notable differences. After the branches describing the complications after a PK in Eye 2, the person has the option to have a regraft first in Eye 2 and then Eye 1. Again, only 1 surgery is assumed to be performed per year. When a regraft is performed in Eye 1, it becomes Eye 2, and all values associated with Eye 2 become associated with Eye 1. A regraft will send the person back to the health state “PK in Eye 2.” An enucleation will send the person to the health state “Enucleation in Eye 2 and Post-PK in Eye 1.” If there is no regraft, no contact lens fitting will be required as it is assumed that a contact lens will be used to treat the patient instead of glasses. The patient would then go to the health state “Post-PK in 2 Eyes.”
Post-PK in 2 Eyes
This health state represents a year in which a patient has had a PK in both eyes. It is assumed that a regraft would happen in Eye 1 first and if not in Eye 1, then in Eye 2. If there is a regraft in Eye 1, then all values associated with Eye 2 would then be associated with Eye 1. Persons requiring a regraft will go to the “PK in 2 Eyes” health state, and those not requiring a regraft will remain in the “Post-PK in 2 Eyes” health state.
Enucleation in Eye 2 and With New PK/Regraft in Eye 1
This health state represents a year in which a person has had an enucleation in Eye 2 and is having a PK performed in Eye 1. A second enucleation is not an option in this health state. Complications of rejection, a rise in IOP, subsequent glaucoma surgery, and “other complication” are represented. It is also possible to require a regraft in Eye 1. The person remains in this state if he or she requires another regraft or, if not, goes to the state “Enucleation in Eye 2 and Post-PK in Eye 1.”
Enucleation in Eye 2 and Post-PK in Eye 1
This health state represents a person who has had an enucleation in Eye 2 and has had a PK in Eye 1. Regraft of Eye 1, no regraft of Eye 1, and death are the only options here. The person can remain in this health state if not requiring a regraft or return to the state “Enucleation in Eye 2 with New PK/Regraft in Eye 1.”
Death
This health state represents a person who has died. The person remains in this health state for the rest of the model, accruing no additional costs.
Parameters Obtained From the CLEK Data 1
We looked at patients with a curvature of less than 48.5 diopters (D), 3 data points, and contacts in each eye. Expected values are shown below, but a triangular distribution (for probabilities) or normal distribution (for the rest of the parameters) was used in the model.
Age
The age of the patients was found to be 40.2 years, with a standard deviation of 9.7.
pGlasses_at_start
This is the probability that a patient is unable to be treated with contact lenses from the beginning of the model. In the first year, approximately 6 out of 170 were unable to be treated with contact lenses.
pContact1, pContact2, pContact3
These parameters are the probability that a patient could be treated with contact lenses throughout the year. Since 89.86% of patients visited a provider 3 or fewer times, 3 is the maximum number of visits per year we assumed in the model. The values of the pContacts were once assumed to be different when creating the model, but for simplicity the average value (99.5%) of the change in number of patients only wearing glasses was used for each value.
Comfort1, Comfort 2
In the CLEK Study, patients rated the comfort of their contact lenses on a 5 point scale: “1 = very comfortable,” “2 = quite comfortable,” “3 = comfortable,” “4 = somewhat irritating,” and “5 = very irritating.” The value of the comfort was assumed to be the same in both eyes. The expected value was found to be 2.4, and the standard deviation was 1.2.
Curvature1, Curvature2
The values of “Curvature1” and “Curvature2” were the worst and best curvatures, respectively. The means were 46.6 D and 44.8 D, respectively.
VA1, VA2
The values of “VA1” and “VA2” were the worst and best high-contrast best-corrected visual acuities, respectively. The Bailey-Lovie charts were used. The means were 50.6 and 52.9, respectively.
Change_curv1, Change_curv2, Change_VA1, Change_VA2, Change_comfort1, Change_comfort2
These parameters represented the change in curvature, best-corrected visual acuity, and comfort yearly. The “1” represented the worst eye and the “2” represented the best eye. The means were 0.207, .0148, -0.119, -0.117, -0.023, -0.035, respectively.
pPK, pPK_glasses
These were the probabilities of a PK in any given year. The work previously done by Gordon and associates 1 provided the parameters predictive of PK. The values for this model were obtained by logistic regression analysis. pPK used the parameters comfort, curvature, age, visual acuity, change in comfort, change in curvature, and change in visual acuity. pPK_glasses predicted PK for a person only wearing glasses and used the parameters curvature, age, visual acuity, change in curvature, and change in visual acuity. The formula used was:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


