Purpose
To study the influence of blepharospasm on dry eye disease by analyzing the clinical features, tear cytokine, and treatment response of patients with dry eye disease accompanied by benign essential blepharospasm.
Design
Prospective case series study.
Methods
Forty adults with a diagnosis of benign essential blepharospasm (BEB) and dry eye disease (DED) were consecutively recruited. Forty subjects with dry eye disease only and 40 healthy adults were recruited as eligible controls. A tear specimen was collected from all participants for cytokine analysis. The patients with benign essential blepharospasm were treated with botulinum neurotoxin type A. The main outcome measures were the following: (1) Ocular Surface Disease Index (OSDI) questionnaire; (2) clinical features, including tear break-up time (BUT), Schirmer І test, and fluorescein staining; (3) conjunctival impression cytology; and (4) multiplex cytokine immunobead assay.
Results
The symptoms of DED + BEB patients were significantly different from those of DED controls and healthy controls. Cytokine analysis in tear fluid also showed that tumor necrosis factor-α, interleukin (IL)-1β, IL-6, IL-2, IL-17, and vascular endothelial growth factor levels were significantly increased in DED + BEB patients. In treatment, botulinum neurotoxin type A injection effectively relieved blepharospasm in all of the DED + BEB patients. Moreover, in this group of patients, OSDI decreased significantly after the botulinum neurotoxin type A injection, and BUT was increased as well.
Conclusion
BEB may participate in the progress of inflammation in DED + BEB patients. Botulinum neurotoxin type A injections could effectively relieve the symptoms of DED + BEB patients and improve their ocular surface condition.
Dry eye disease (DED) is defined as a multifactorial disease of the tears and the ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability, with potential damage to the ocular surface. It is associated with the synergy of increased osmolarity of the tear film and inflammation of the ocular surface.
Benign essential blepharospasm (BEB) refers to a pattern of bilateral orbicularis oculi dystonia leading to involuntary closure of the eyelids. The main symptoms of blepharospasm are grumbling facial expression, fluttering of eyelids, an increase in the frequency of blinking, and chronic involuntary contractions that eventually affect both eyes. In addition to uncoordinated contraction of the eyelid protractors and eyelid retractors, observational data show that a number of patients with blepharospasm also suffer from dry eye disease to various degrees. The recent study by Park and associates also showed that the production, distribution, and drainage of tears in patients were affected by blepharospasm. In addition, neurotoxin injections improved dry eye symptoms in patients with essential blepharospasm.
Typical subjective discomfort symptoms of dry eye disease (including burning sensation, grittiness, or dryness of the eyes and photophobia) occur in 40%-60% of patients before or at the onset of BEB. In recent years, many researchers have attempted to interpret the synergic pathologic mechanism of a combination of DED and BEB. However, no major advancement has been achieved.
The aim of this study was to investigate the influence of blepharospasm on dry eye disease. In this study, we compared the symptoms and clinical features of patients with DED accompanied by BEB with those of controls with dry eye disease only and unrelated healthy controls. We collected tear specimens from each subject to investigate differences in cytokine expression in tear fluid between these 3 groups to elucidate the underlying mechanism of BEB. Furthermore, the curative effects of an appropriate dose of botulinum neurotoxin type A injections in patients with DED accompanied by BEB were investigated in the study.
Methods
Study Design
This was a prospective case series study performed at Zhongshan Ophthalmic Center, Sun Yat-sen University, China. The patients were prospectively enrolled from January 1, 2011 through October 31, 2011. The study was approved by the ethics committee of Zhongshan Ophthalmic Center, Sun Yat-Sen University. Informed consent for the study was obtained at the time of enrollment. The study adhered to the tenets of the Declaration of Helsinki.
Eligibility
Forty Chinese adults with a diagnosis of benign essential blepharospasm and dry eye disease (Group 3) were consecutively recruited from Zhongshan Ophthalmic Center. The diagnosis of BEB was made according to published standard criteria. Patients with neurologic abnormalities in addition to dystonia and patients with features suggesting dopa-responsive dystonia, myoclonus-dystonia, or secondary dystonias were excluded. Subjects with ocular surface disease, such as keratitis or conjunctivitis, were also excluded. Diagnoses were confirmed by the senior neurologist with extensive experience in movement disorders. Forty subjects with the diagnosis of dry eye disease (Group 2) and 40 unrelated healthy participants (Group 1) were recruited as controls, matched for age and sex.
Further inclusion criteria included the presence of typical symptoms of dry eye disease (dryness, burning, foreign body sensation, ocular pain, photophobia, or easily fatigued eye) and a markedly reduced tear break-up time and Schirmer І test according to the dry eye criteria by Lemp and Pflugfelder and associates. All of the patients diagnosed with DED or DED + BEB were not administered any topical or other DED treatments during the study period.
Assessments
For the diagnosis of dry eye disease and the evaluation of symptoms, each participant’s subjective reports were evaluated after objective observation using a validated Chinese-translated version of the Ocular Surface Disease Index questionnaire (OSDI). The patients in Group 3 were assessed with OSDI again at 1 week after neurotoxin administration. Total OSDI scores were calculated as previously recommended by Schiffman and associates.
Immediately after completing the questionnaire, all subjects underwent a thorough ophthalmologic examination of the anterior segment. Ophthalmologic evaluation of each participant was performed by the same specialist. Ocular examinations consisted of tear break-up time (BUT), the Schirmer І test, and fluorescein staining.
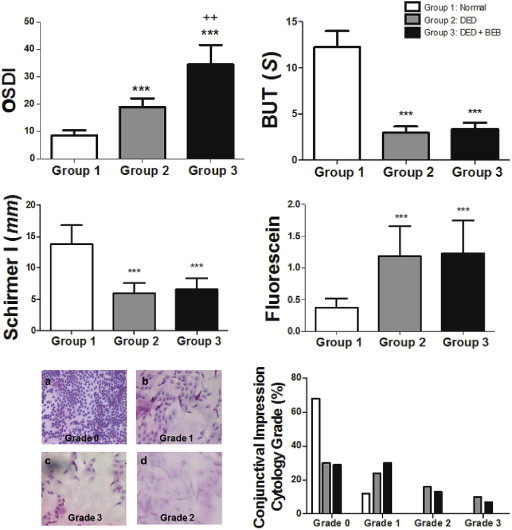
For fluorescein staining, fluorescein strips were wetted with a standardized drop volume of nonpreserved saline solution. The cornea was examined 3 minutes after the last instillation by light passed through a cobalt-blue filter and examined through a biomicroscope containing a Wratten #12 barrier filter. The results were recorded on a cornea diagram as shown in Figure 1 . Punctate staining was recorded using a standardized grading system of 0-3 for each of the 5 areas.
Tear BUT was used to evaluate the stability of the tear film by measuring the time required for the film to break up after complete blinking. BUT was measured by contacting the inferior conjunctiva with a commercially available fluorescein test strip. Subjects were instructed to blink 3 times, followed by gazing straight ahead without blinking. The tear film was observed using a yellow filter under wide lighting. The interval between the last blink and the appearance of the first corneal dry spot was measured. The procedure was repeated 3 times, and the mean value was recorded.
The Schirmer I test (with anesthesia) quantifies tear production. One minute after instillation of the topical anesthetic drops (0.5% proxymetacaine; Alcaine, Alcon, Fort Worth, Texas, USA), a Schirmer strip (filter paper) was placed on the lower conjunctiva between the lateral and the external third. The distance that the tears traveled on the filter paper was measured after 5 minutes. A measured distance less than 5 mm with anesthesia was considered abnormal and indicative of an aqueous-deficient state.
Impression cytology was performed in all subjects. Sheets of cellulose acetate filter paper (type VC, 0.10 μm, VCWP 04700; Millipore Corp, Bedford, Massachusetts, USA) were used to collect cells from the superior and inferior bulbar conjunctiva. The specimens were stained using the procedure previously described by Tseng and examined through a light microscope. Between 0 and 3 points were added from each of the following parameters to calculate the impression cytology (IC) score: the morphology of the epithelial cells; cell-to-cell contact; grade of squamous metaplasia (nucleus-to-cytoplasm ratio); appearance of nuclear chromatin (pyknosis, “snakes,” fragmentation); keratinization; the distribution, number, and morphology of goblet cells; the number and type of inflammatory cells; and mucous aggregation. A total of 0-7 points was typical for normal cell morphology, 8-14 points for slightly pathologic, 15-21 points for moderately pathologic, and 22-30 points for intense pathologic changes.
Multiplex Cytokine Immunobead Assay
Tears were collected before any other test and at a minimum of 10 minutes after the patient had completed the questionnaire. Unstimulated tear samples were collected nontraumatically from the external canthus of open eyes in each participant, avoiding an additional tear reflex as much as possible. Glass capillary micropipettes (Microcaps 2 μL; Drummond Scientific, Broomall, Pennsylvania, USA) were used to collect 10 μL of tears. Each sample was then collected in a sterile collection tube at 4 C and stored at −80 C until assayed. The samples were obtained from the right eye and left eye of each individual and were not pooled.
Cytokine levels in tear samples were determined by a Human Multi Analyte Profiling Base Kit A (Fluorokine MAP; LUH000; R&D Systems, Wiesbaden, Germany) using a Luminex 200 detector (Luminex, Austin, Texas, USA) according to the manufacturer’s instructions. Briefly, tear samples were added to wells containing an appropriate cytokine bead mixture that included human monoclonal antibodies specific for interleukin (IL)-1β, IL-2, IL-6, IL-8/CXCL8, IL-10, IL-17, tumor necrosis factor (TNF)-α, and vascular endothelial growth factor (VEGF) and incubated overnight at 4°. Washed beads were further incubated with biotin-labeled anti-human cytokine antibodies for 1 h at room temperature followed by incubation with streptavidin-phycoerythrin for 30 minutes. Samples were analyzed using Luminex 200 and Statlia software (Brendan Technologies Inc, Carlsbad, California, USA). Standard curves of known concentrations of recombinant human cytokines were used to convert median fluorescence intensity (MFI) to cytokine concentration in pg/mL. Only the linear portions of the standard curves were used to quantify cytokine concentrations.
Botulinum Neurotoxin Type A Injection for Treatment of Benign Essential Blepharospasm and Dry Eye Disease Patients
The group of 40 Chinese patients with DED accompanied by BEB received treatment with botulinum neurotoxin type A injections. By diluting 100 U of the botulinum neurotoxin type A (Allergan, Inc, Irvine, California, USA) in 2 mL of saline that included no preservatives (0.9% NaCl) before use, a solution with a working concentration of 5 U botulinum neurotoxin type A/0.1 mL was obtained. The dose of botulinum neurotoxin type A per injection site was 2.5 U. The injection locations are presented in Figure 2 . To prevent drug interactions, no other drugs were used during the study.

Examinations After Treatment
According to the procedures above, the posttreatment examinations, including the OSDI questionnaire, tear film BUT, Schirmer I test (with anesthesia), fluorescein staining, and impression cytology, were conducted 1 week after the botulinum neurotoxin type A injections. In addition, the severity of the contractions in the eyebrow and eyelid were recorded before botulinum neurotoxin type A injection and 1 week later. The classification of severity was based on Cohen’s blepharospasm evaluation scale from 0-4: 0 for none; 1 for increased blinking caused by external stimuli; 2 for mild, noticeable fluttering that is not incapacitating; 3 for moderate, very noticeable spasm that is mildly incapacitating; 4 for severely incapacitating spasm (unable to drive, read, etc). Moreover, tears of 6 patients after treatment were collected for multiplex cytokine immunobead assay.
Statistical Analysis
The data are presented as the arithmetic mean ± standard deviation. Comparisons of sex and symptoms were performed with the χ 2 test. Student t test or analysis of variance (ANOVA) with Tukey post hoc test was used for other statistical comparisons. P ≤ .05 was considered statistically significant. All statistical tests were performed using GraphPad Prism 5.0 software (Graph-Pad Prism, Inc, San Diego, California, USA; http://www.graphpad.com ).
Results
A total of 239 eyes of 120 patients were included in the study after the exclusion of ineligible subjects. The baseline characteristics of the enrolled participants were similar among the 3 groups ( Table 1 ).
| No. of Patients | No. of Eyes | Sex (Female/Male) | Age (y) (Mean ± SD) | |
|---|---|---|---|---|
| BBEB + DED | 40 | 79 | 26/14 | 57.8 ± 8.5 |
| Control | ||||
| DED | 40 | 80 | 24/16 | 58.1 ± 9.2 |
| Normal | 40 | 80 | 24/16 | 56.6 ± 7.9 |
Although patients with DED accompanied by BEB (Group 3) and dry eye controls (Group 2) differed from the healthy control group (Group 1) in multiple parameters (tear BUT, Schirmer I test score, fluorescein staining score, and OSDI score) ( P < .001), no evident differences were found in either the quantitative outcomes or the clinical features between Group 3 and Group 2 ( Figure 3 ). However, the OSDI score was significantly higher in Group 3 than in Group 2 (34.50 ± 7.12 vs 19.00 ± 3.19; P = .002<.01) ( Figure 3 ), especially regarding the presence or severity of photophobia and easily fatigued eye ( Figure 4 ).