Stereotactic neurosurgery originated from the pioneering work of Horsley and Clarke, who developed a stereotactic apparatus to study the monkey brain in 1908. Spiegel and Wycis applied this technology to the human brain in 1947, which ultimately lead to the development of multiple stereotactic neurosurgical devices during the 1950s. It was Lars Leksell of Sweden, however, who envisioned stereotactic radiosurgery. Leksell developed the gamma knife to treat intracranial lesions in a noninvasive fashion. His work stimulated worldwide interest and created the field of stereotactic radiosurgery.
Stereotactic radiosurgery evolved from the pioneering work reported in 1908 by Horsley, a neurophysiologist and neurosurgeon, and his associate Clarke, a mathematician. Horsley and Clarke developed a tool that could localize an intracranial structure in three dimensions, enabling the insertion of a needle electrode for studying a desired locale within the monkey brain. These early investigators developed a stereotactic atlas of the monkey brain based on a cartesian coordinate system relative to landmarks (the inferior orbital rim and internal auditory canal) on the monkey’s skull. Similar to today’s stereotactic head frames, their stereotactic apparatus was fixed to the monkey’s skull. Using this apparatus, Horsley and Clarke were the first to describe the stereotactic destruction of an intracranial target using electrode electrocoagulation. Despite the fact that Clarke patented the use of this device in humans, it was never applied outside the animal model.
Spiegel, a neurologist and director of experimental neurology at Temple Medical School in Philadelphia, began developing the first stereotactic device for human use. Spiegel and colleagues, a neurosurgeon who worked in Spiegel’s laboratory as a medical student, reported on their human stereotactic apparatus in 1947. Their device was fixed to the patient’s head in much the same way as Horsley and Clarke’s simian model; however, intraoperative radiographs were used for localizing intracranial structures during the procedure. By 1952, Spiegel and Wycis had developed a stereotactic atlas of the human brain, and they coined their technique stereoencephalotomy. Their methods paved the way for functional human stereotactic neurosurgery. By this time, it was understood that sectioning the extrapyramidal system could be used to treat movement disorders such as Parkinson’s disease; however, open neurosurgical operative mortality was quite high at the time. Russell Meyers, a neurosurgeon at the University of Iowa and a leader in functional neurosurgery for movement disorders, reported that his open neurosurgical techniques carried a 15.7% mortality rate. By 1958, Spiegel and colleagues were reporting the operative mortality for stereotactic surgery for movement disorders to be 2%. Their methodology and reduced mortality rate were met with enthusiasm by the worldwide neurosurgical community. Multiple stereotactic apparatus designs were developed in the 1950’s, and it was estimated that nearly 25,000 functional stereotactic procedures were done worldwide before the introduction of L-dopa therapy for movement disorders.
Lars Leksell is known as the father of stereotactic radiosurgery for his pioneering work applying the stereotaxic technique to radiation delivery. Leksell was born in Fassberg, Sweden, in 1907, and attended medical school at the Karolinska Institute. By 1935, he began his neurosurgical training under Herbert Olivecrona, and ultimately succeeded him as chairman of neurosurgery in 1961. Leksell understood that much of the morbidity and mortality associated with neurosurgery during this time was a consequence of invasive procedures, and therefore, he dreamed of developing a minimally invasive approach to treat intracranial lesions. Building on the principles produced by Horsley and Clarke and applied by Spiegel and Wycis, Leksell developed his arc-centered stereotactic apparatus for intracerebral surgery in 1947. The device enabled the precise placement of a needle or electrode into a desired location within the human brain. Leksell first described the concept of stereotactic radiosurgery in 1951. The initial device used a collimated x-ray beam (gamma rays) that could move along the semicircular arch of his stereotactic apparatus to strike an intracranial target. Leksell discussed the potential of using stereotactic radiosurgery to produce a lesion within the human brain, and noted the technology might be well-suited for functional neurosurgery. As exciting as the concept was, the effect of radiation on the central nervous system was poorly understood. Further research was needed, and Leksell developed a feline stereotactic radiosurgical device to determine the effects on the cat brain.
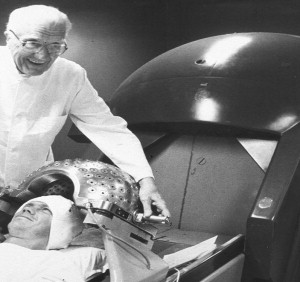
During the late 1950s and early 1960s Leksell searched for an ideal form of radiant energy convenient for clinical stereotactic radiosurgery. Physicists Liden and Larrson of Uppsala University in Sweden were integral in the development of a system that used a cyclotron to direct proton beams at a target. These physicists determined in the animal model that a sharply delineated stereotactic lesion was produced with high-energy protons. In 1960, Leksell and colleagues performed their first human stereotactic proton beam operation (a bilateral anterior capsulotomy) at the Gustaf Werner Institute in Uppsala. About the same time, Woodruff and colleagues at University of California at Berkeley introduced a similar cyclotron-based radiosurgery system and began irradiating pituitary lesions. The cyclotron ultimately was determined to be too cumbersome and impractical for clinical use. Leksell eventually settled on gamma rays as a practical compromise for stereotactic radiosurgery. The first gamma unit was installed in the Sophiahemmet Hospital in Stockholm, Sweden, in 1968. The device used 179 sources of cobalt-60 distributed with collimators to create a sharply circumscribed disc-shaped lesion, and the device initially was intended for use during functional neurosurgery. The second gamma unit was installed at the Karolinska Hospital in Stockholm, Sweden, in 1974 ( Fig. 1 ). This updated version was designed specifically for stereotactic radiosurgery and produced a more practical spherical radiation field. Plain radiographs and air encephalography typically were used to identify the target during these early procedures. In 1972, Steiner and colleagues applied angiography to radiosurgery when treating the first arteriovenous malformation.
Target localization improved dramatically when CT was used in conjunction with the stereotactic apparatus, as reported by Bergstom and Grietz in 1976. Leksell described the application of CT during radiosurgery and noted the technique enabled rapid and accurate target localization. With the advent of better imaging methods, solid tumors became radiosurgical targets. Leksell and Jernberg’s rationale for treating vestibular schwannomas with radiosurgery is detailed in his A Note on the Treatment of Acoustic Tumours . Leksell discussed how Harvey Cushing referred to the cerebellopontine angle as the bloody angle, and that a noninvasive modality to treat these tumors was needed. Furthermore, he quoted Pool, who stated complete acoustic tumor removal was “ not only one of the most exacting and laborious, but also one of the most dangerous and unpredictable operations in the entire neurosurgical repertoire.” Leksell further discussed the evolution of vestibular schwannoma surgery and the operative morbidity and mortality reported by vestibular schwannoma surgeons of the time (Pool, Olivecrona, House, and Hitselberger). He discussed that despite improving mortality rates, incomplete tumor removal was common and often had unsatisfactory long-term results. Leksell believed stereotactic radiosurgery was a logical approach to decrease the morbidity and mortality associated with vestibular schwannoma surgery.
From 1968 to 1982, Leksell treated 762 patients who had stereotactic radiosurgery using the Gamma Knife (Elekta, Stockholm, Sweden), and over half of these patients had arteriovenous malformations or benign tumors, including 94 vestibular schwannomas. By 1985, Leksell and colleagues reported the potential application of MRI to radiosurgery, pointing out the many advantages of this detailed imaging modality. Today CT, MRI, and angiography are used commonly during radiosurgical planning.
After 4.5 years of intensive regulatory review, the first Gamma Knife unit was installed in the United States at the University of Pittsburgh in 1987 under the leadership of Lunsford, a neurosurgeon. Lunsford’s effort paved the way for the installation of Gamma Knife units throughout the United States. The first updated model C Gamma Knife unit was installed in Krefeld, Germany, in 1999. This unit included sophisticated treatment planning software and an automated positioning system (APS) that was less cumbersome and time-consuming than the model B manual trunnion system. The APS offered more conformal dose plans and less radiation exposure to personnel. The model C Gamma Knife is the most commonly used unit throughout world today. The latest version of the Gamma Knife, the Leksell Gamma Knife Perfexion was introduced in 2006 and the first unit became operational at the Timone University Hospital of Marseille, France. The Perfexion is reported to have a wider treatment range, enabling the collision-free management of hard-to-reach targets in a shorter period of time.
Although Leksell considered employing linear accelerator (LINAC) technology for stereotactic radiosurgery, technical and accessibility limitations led him to use gamma rays. The first report using a LINAC- based radiotherapy system was in 1983 by Betti and Derechinsky. Their early device employed several isocentric fixed radiation fields arrayed on different planes, and the patient’s head then was rotated around a horizontal lateral axis. Shortly thereafter, Colombo and colleagues reported their technique based on multiple converging arc irradiations. Hartman and colleagues reported a similar technique in 1985. It was Lutz and Winston, however, who created the technology to quantify and calculate dosimetry and improve the accuracy of the LINAC- based system. Most commercially available LINAC systems today are an evolution of Lutz and Winston’s original work. Since linear accelerators were more available and less expensive, the LINAC became a popular radiosurgery system. Sophisticated and easy-to-use dosimetry planning software has been produced, and starting in the mid-to-late 1980s, the Brigham and Women’s Hospital in Massachusetts and the University of Florida began treating patients with their LINAC stereotactic radiotherapy systems. Today, over 150 LINAC radiotherapy systems are in use worldwide, and many different models are emerging to meet the needs of this increasingly popular form of radiotherapy.
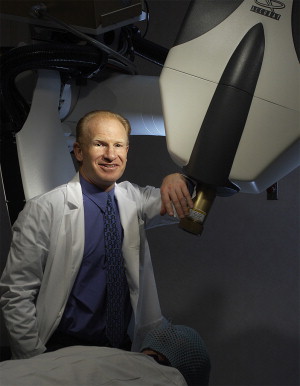
Perhaps the most innovative LINAC based system developed in recent years was produced by Adler and colleagues, a neurosurgeon at Stanford University (Stanford, California) ( Fig. 2 ). In 1997, Adler introduced the Cyberknife (Accuray Incorporated, Sunnyvale, California) at the 12th meeting of the World Society of Stereotactic Functional Neurosurgery. Cyberknife is a frameless stereotactic radiotherapy system that mounts a lightweight (130 lb) 6 mV linear accelerator on a highly mobile robotic arm. This revolutionary design incorporates a real-time guidance system, which obviates the need for rigid fixation as used in frame base systems. Cyberknife determines the location of the skull or spine in the coordinate frame of the radiation delivery system by comparing digitally reconstructed CT phantoms obtained from the patient’s treatment planning images with real-time oblique radiographs obtained during the procedure. If needed, fiducials may be implanted within the target and used during image registration. The dose placement accuracy has been determined to compare favorably with frame-based systems. When the patient (target) moves, the system detects the change, and the robot makes appropriate adjustments to maintain accurate targeting. It is also possible, through sophisticated infrared tracking, to accommodate target movement during respiration. This innovative system has enabled stereotactic radiotherapy to be expanded to include the head, spine, chest, abdomen, and pelvis.