This article presents basics of ultrasound technology for the office, evaluation technique, thyroid and parathyroid imaging, ultrasound for neck lymphatics, office-based head and neck ultrasound biopsy, and therapeutic applications of head and neck ultrasound.
Ultrasound for the head and neck surgeon
Ultrasound has increasingly moved from being a modality confined to the radiology department to an active diagnostic and therapeutic aid available to the head and neck at the point of patient care. Ultrasound as a modality offers several advantages, including small size, low cost of instrumentation, steadily improving resolution, and lack of ionizing radiation and can readily be incorporated into a surgeon’s algorithm for determining risk of malignancy in lymph nodes and thyroid nodules. The clinical application of ultrasound for head and neck surgeons continues to evolve with increasing levels of information derived from the technology, increasing numbers of practitioners becoming familiar with ultrasound, and a rapidly expanding volume of literature. A PubMed search from January 1, 2000, to January 1, 2010, revealed 1800 articles regarding the use of ultrasound in the head and neck (almost 5 articles per day).
The use of ultrasound has become increasingly sophisticated with 2-D imaging as well as Doppler flow, which help characterize vascular patterns, in particular for hyperechoic foci within the thyroid gland to distinguish vessels from cystic masses. Addition of advanced ultrasound techniques, such as elastography, increases ultrasound specificity in detecting thyroid malignancy. Increasingly, there are ultrasound-related courses and didactic training for practicing physicians. Formal ultrasonography head and neck curricula exist, for example, in the postgraduate medical education head and neck ultrasound course of the American College of Surgeons. In order to optimize safety and accuracy of ultrasonography in an otolaryngology practice, systematic application of the modality with full knowledge of the strengths and weaknesses of the modality must be appreciated.
Basics of ultrasound technology for the office
There are many clinical ultrasound systems available for clinical use in the office and at the bedside. Small size, portability, and affordability of this equipment have made it more available and attractive to clinical practice. System requirements can be viewed as basic and advanced. More advanced components may require increasing levels of training for accurate use. Table 1 lists basic and advanced requirements for office-based ultrasound systems.
| Component | Basic | Advanced |
|---|---|---|
| Ultrasound machine | 1. High frequency (7.5–14 MHz) 2. A and B modes 3. Color-coded duplex (enhances differentiation of cystic areas and vascularity) | 1. 3-D ultrasound 2. Elastography |
| Education | 1. American College of Surgeons course 2. American Academy of Otolaryngology | 1. Radiological Society of North America 2. American Association of Clinical Endocrinologists |
Basics of ultrasound technology for the office
There are many clinical ultrasound systems available for clinical use in the office and at the bedside. Small size, portability, and affordability of this equipment have made it more available and attractive to clinical practice. System requirements can be viewed as basic and advanced. More advanced components may require increasing levels of training for accurate use. Table 1 lists basic and advanced requirements for office-based ultrasound systems.
| Component | Basic | Advanced |
|---|---|---|
| Ultrasound machine | 1. High frequency (7.5–14 MHz) 2. A and B modes 3. Color-coded duplex (enhances differentiation of cystic areas and vascularity) | 1. 3-D ultrasound 2. Elastography |
| Education | 1. American College of Surgeons course 2. American Academy of Otolaryngology | 1. Radiological Society of North America 2. American Association of Clinical Endocrinologists |
Evaluation technique: an anatomic approach
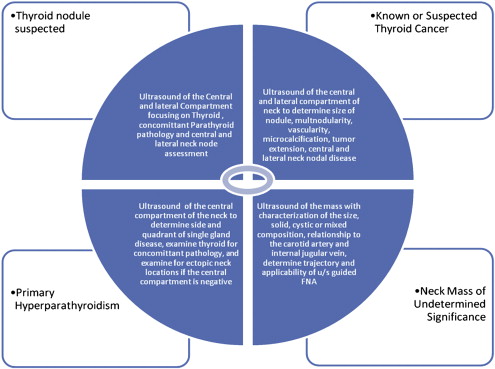
Development of a systematic approach to performing head and neck office-based ultrasonography is paramount in order to adequately assess pathology and not miss potentially important clinical findings. Fig. 1 outlines a systematic approach to head and neck ultrasonography and represents only one organizational scheme. The examination should include the central or visceral compartment of the neck in both longitudinal and transverse planes. Within the central compartment, attention is directed at the endocrine organs (thyroid and parathyroid), trachea, esophagus, and paratracheal and prelaryngeal and pretracheal lymph nodes. In the postoperative neck of well-differentiated thyroid cancer patients, accurate reporting of size, location, and character of lymph nodes is important to assess for disease progression. The lateral neck must also be evaluated in patients with thyroid cancer; failure to do so results in poor sensitivity of the examination in detection of lymphadenopathy.
Thyroid ultrasound
With respect to the thyroid gland, the dimensions of both lobes and the isthmus should be assessed and recorded, which requires assessment in the longitudinal and transverse planes. Size, location, and echo characteristics should also be recorded. Vascular patterns surrounding nodules from Doppler flow may provide etiologic clues. Any calcifications should be noted and preferably recorded as static images. A pattern of microcalcification in a nodule significantly increases the risk that the nodule may be malignant. In the multinodular thyroid gland, ultrasound is particularly helpful in recognizing areas within the gland that are at higher risk of malignancy, such as nodules greater than 1 cm and those possessing hypervascularity and microcalcification. Limitations of ultrasound in thyroid assessment include assessment of substernal extent of the gland, predicting airway invasion, distinguishing coexistent lymph node from parathyroid pathology, and lack of definitive pathologic characteristics in the context of a multinodular gland. Table 2 lists common characteristics of thyroid malignancy on ultrasound.



