Purpose
To evaluate the effect of size and accommodative characteristics of fixation targets on the distant angle of deviation in patients with intermittent exotropia in the context of interobserver and intraobserver variability of the prism cover test.
Design
Cross-sectional observational study.
Methods
Settings: Institutional. Patients: Sixty subjects with intermittent exotropia. Observation: Prism cover tests were performed by 2 independent examiners. The distant angle of deviation was measured with 4 different targets at 6 m. The targets varied in size and accommodative characteristics: black-on-white optotypes with a visual angle of 50 minutes of arc (MOA; large figure) and 10 MOA (small figure) and green lights with a visual angle of 50 MOA (large light) and 10 MOA (small light). Main Outcome Measures: Interobserver variability, intraobserver variability, test-retest reliability using different targets, and the influence of factors on the magnitude of absolute test–retest variability.
Results
The 95% limits of agreement of the prism cover test between different targets (± 3.0 to 6.0 prism diopters [PD]) were similar to the intraobserver variability (± 3.9–4.8 PD) and slightly smaller than the interobserver variability (± 6.3–6.5 PD). The only factor strongly correlated to the magnitude of interobserver variability was the magnitude of target-related intraobserver variability.
Conclusions
The size and accommodative characteristics of a target do not cause significant variability beyond the natural variability of the prism cover test for distance in intermittent exotropia. Differences less than 6 PD from one prism cover test measurement are likely to represent test–retest variability.
The quantitative angle of strabismus is measured by the prism cover test, with the subject fixating on an accommodative target. Accommodative targets are required for good fixation during measurement of strabismus to control accommodation, but too-small targets may overstimulate accommodation, which also is affected by target size and detail. Although accommodation is considered to be important in the measurement of esotropia or near deviation in exotropia, its effect on distant measurements of exotropia is less well known. The influence of different targets on the angle of exodeviation, beyond the natural variability of the prism cover test, is unclear. The aim of this study was to evaluate the effects of size and accommodative characteristics of fixation targets on the distant angle of deviation in patients with intermittent exotropia. Results were analyzed in the context of interobserver and intraobserver variability.
Methods
Patients
The subjects of our study were consecutive patients younger than 15 years who visited our clinic for intermittent exotropia and were fully cooperative with the prism cover test while fixating on a target. We noted patient characteristics, including age, gender, best-corrected visual acuity, refractive errors, deviation at distance and near, type of exotropia according to the Burian classification, constancy of deviation (intermittent or constant), and fixation dominance. Constant deviation was defined as divergence for 100% of waking hours. Eye dominance was determined by repeated alternating cover–uncover testing of each eye more than 3 times, which invariably revealed a fixation shift to a dominant fixating eye after uncovering the occluder during the tropic phase of exotropia. Patients were excluded if best-corrected visual acuity was worse than 20/20 in either eye or if they had refractive errors exceeding −6.00 diopters (D; myopia) or +3.00 D (hyperopia), anisometropia > 1.50 D, astigmatism > 1.50 D, exodeviations ≥ 50 prism diopters (PD), A-pattern exodeviation (downgaze–upgaze) ≥ 10 PD, V-pattern exodeviation (upgaze–downgaze) ≥ 15 PD, dissociated vertical deviation, vertical deviation > 5 PD, a history of strabismus surgery, paralytic or restrictive exotropia, ocular disease other than strabismus, systemic disorders such as congenital anomalies, or neurological disorders.
Ophthalmologic Examination
All patients underwent a complete ophthalmologic examination. Refractive errors were determined using cycloplegic refraction with 1% cyclopentolate hydrochloride, and these are reported as spherical equivalent values. Patients with hyperopia were given spectacles with lenses of approximately +1.00 to +1.50 D less than the full cycloplegic hyperopic refraction. Sensory status was evaluated using the Randot stereoacuity test (Stereo Optical Co, Inc, Chicago, Illinois, USA) and the Distance Randot stereotest (Stereo Optical Co, Inc, Chicago, Illinois, USA). A stereoacuity of 100 seconds of arc or better was defined as good. Accommodative amplitudes were measured by the minus lens method at 6 m.
Prism Cover Test
Alignment measurements were made by the prism cover test at distance and near fixation by 2 independent examiners. The standard set of plastic prisms (Richmond products, Inc, Albuquerque, New Mexico, USA) was used for all measurements. The individual prisms increased in power from 1 to 2 PD in 1-PD increments, from 2 to 20 PD in 2-PD increments, and from 20 to 45 PD in 5-PD increments. For the prism cover test, the examiners placed a plastic prism in the frontal plane position before one eye and alternately occluded the eyes. The base-in prism power was increased gradually until the direction of refixation moved outward. The prism power then was reduced until no further refixation movement of the fellow eye was seen. The prism magnitude that neutralized the deviation, or the median value of consecutive prisms between which refixation movements reversed direction, was recorded. Prisms were not stacked or split, because patients with deviations of ≥ 50 PD were excluded. To eliminate the effect of fatigue, patients underwent a full dissociative cover–uncover test before entering the examination. A total of 3 prism cover test sessions were performed by 2 independent examiners (H.K.Y., J.-M.H.). Each session was performed at least 15 minutes apart but within 1 hour of each other, and each examiner was masked to the other’s measurements. The targets used in distance measurements varied in size and accommodative characteristics: (1) a black-on-white optotype 4, which subtended a visual angle of 50 minutes of arc (MOA), equating to a Snellen optotype of 20/200 with background illuminance (260 cd/m 2 ; large figure); (2) a green light (260 cd/m 2 ) with a visual angle of 50 MOA (large light); (3) a black-on-white optotype 4, which subtended a visual angle of 10 MOA equating to a Snellen optotype of 20/40 with background illuminance (260 cd/m 2 ; small figure); (4) a green light (260 cd/m 2 ) with a visual angle of 10 MOA (small light). Each target measurement was performed at least 15 minutes apart but within 1 hour of each other, and the order of the tests was randomized for each subject.
First session by examiner A (A1): Prism cover test was performed at 6 m by examiner A. The distant angle of deviation was measured with 4 different targets.
Second session by examiner B: Prism cover test was performed at 6 m and 0.33 m by another examiner (examiner B) with accommodative targets equating to a Snellen optotype of 20/40 at both distance and near. Near measurements were taken for the classification of exotropia type. To minimize the lasting effect of proximal fusion, the third session was performed at least 1 hour later.
Third session by examiner A (A2): Distant prism cover test measured with the 4 different targets was repeated by examiner A.
Main Outcome Measures
Primary outcome measures were as follows. First, interobserver variability was calculated between the 2 independent examiners for the distant prism cover test with an accommodative target of Snellen optotype 20/40. Second, intraobserver variability was calculated for each of the 4 targets. Finally, the test–retest reliability between the 4 targets and intraclass correlation coefficients were calculated. This estimates the absolute agreement and reliability of single ratings measured by different targets.
Secondary outcome measures included the influence of factors on the magnitude of absolute test–retest variability, which was examined in linear regression models. The magnitude of target-related intraobserver variability was defined as the absolute range of the test–retest values. The association of various factors on the magnitude of interobserver variability and target-related variability was investigated, including the magnitude of angle deviation (based on the average value of measurements), gender, age, refractive errors, spectacle wearing, type of exotropia, constancy, fixation dominance, distance and near stereoacuity, and accommodative amplitudes.
Statistical Analysis
Statistical analyses were performed using SPSS software for Windows version 15.0 (SPSS, Inc, Chicago, Illinois, USA) and the MedCalc statistical packages version 11.3 (MedCalc Statistical Software, Mariakerke, Belgium). The absolute difference between tests was calculated for each pair of measurements with the 95% limit of agreement and 95% confidence intervals. Agreement between measurements was represented in Bland–Altman plots. The influence of variable factors on the magnitude of absolute test–retest variability was examined in logistic regression models to account for correlation between different examiners and between different targets for the same subject. The magnitude of absolute test–retest differences was changed into a 2-level categorical variable indicating less than or more than the half-width of the 95% limit of agreement. P values less than .05 were considered statistically significant.
Results
Patients and Ophthalmologic Examination
A total of 60 subjects completed all 3 sessions of prism cover test measurements. Subjects ranged in age from 4 to 15 years with a mean (standard deviation) age of 7.7 years (2.8 years); 26 subjects (43.3%) were male. The mean (standard deviation) cycloplegic refractive errors of both eyes were −0.70 D (1.45 D; range, −6.00 to +1.75 D), and 32 patients (53.3%) wore spectacles. Fifty-five patients (91.7%) had basic exotropia and 5 patients (8.3%) had convergence insufficiency exotropia, defined as exotropia that is greater by 10 PD or more at near than at distance. Exodeviation was constant at distance in 36 patients (60.0%) and at near in 9 patients (15.0%), whereas the remaining subjects showed intermittent deviation. Fixation dominance was equal in both eyes of 33 subjects (55.0%), dominant in the right eye of 12 subjects (20.0%), and dominant in the left eye of 15 subjects (25.0%). Good stereoacuity was found in 5 patients (8.3%) at distance and in 38 patients (63.3%) at near.
Interobserver VARIABILITY
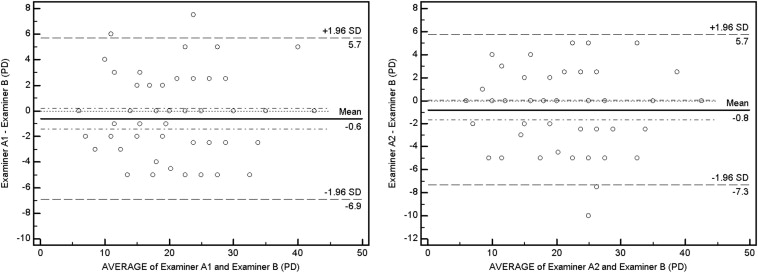
The mean (standard deviation) values of the distant angle of exodeviation measured with an accommodative target (Snellen equivalent of 20/40) at 6 m by examiner A and B were 21.5 PD (7.9 PD; range, 6 to 42.5 PD) and 22.1 PD (8.0 PD; range, 6 to 42.5 PD), which were not significantly different. Test and retest results of these measurements were compared between the 2 independent examiners. The 2 measurements by examiner A (A1, A2) each were compared with the results of examiner B. The deviations were identical in 20.0% (A1 vs B) and 26.7% (A2 vs B) of each examination and were within 5 PD in 96.7% and 96.7%, respectively. Intraclass correlation coefficients (95% confidence interval) of the 2 measurements by examiner A (A1, A2) compared with the results of examiner B were 0.916 (0.864 to 0.949) and 0.906 (0.848 to 0.943), respectively. The 95% limit of agreement of each measurement is represented on the Bland–Altman plots in Figure 1 . The half-width of the 95% limit of agreement was 6.3 PD and 6.5 PD for the 2 independent examiners, respectively. The Bland–Altman plots suggest that the magnitude of the test–retest differences did not depend on the angle of deviation, showing consistent variability across the graph, except for magnitudes less than 10 PD, which were less variable than at magnitudes of 10 PD or more. Also, there was no overall tendency for either examiner to test higher or lower than the other.
Intraobserver VARIABILITY
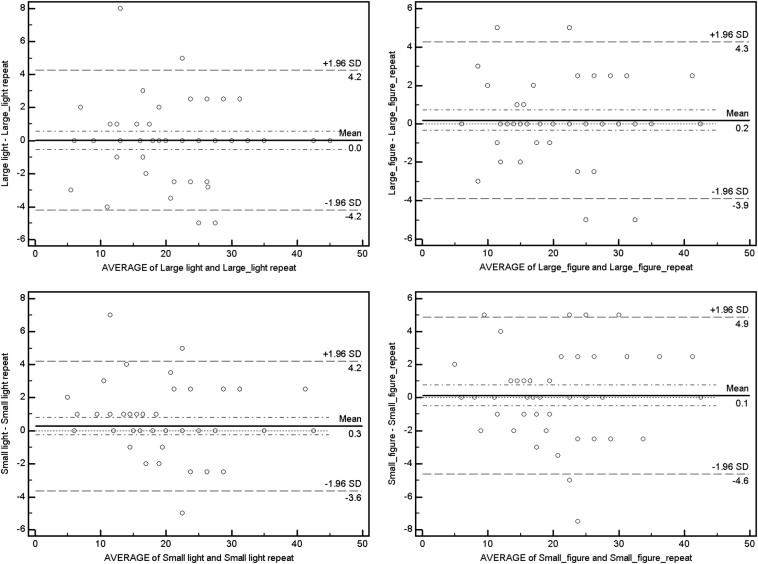
Test and retest results for the large light, large figure, small light, and small figure by examiner A were identical in 53.3%, 53.3%, 48.3%, and 31.7% of all subjects, respectively, and within 5 PD in 98.3%, 100%, 98.3%, and 98.3%, respectively. Intraclass correlation coefficients (95% confidence interval) of the large light, large figure, small light, and small figure were 0.964 (0.940 to 0.978), 0.965 (0.942 to 0.979), 0.966 (0.943 to 0.979), and 0.952 (0.921 to 0.971), respectively. The 95% limit of agreement of the repeatability of each target is represented on the Bland–Altman plots in Figure 2 . The Bland–Altman plots suggest that the magnitude of variability was independent of the angle of deviation, showing consistent variability across the graph. The half-width of the 95% limit of agreement was 4.2 PD, 4.1 PD, 3.9 PD, and 4.8 PD, respectively. There was no overall tendency for the retest values to be higher or lower than the initial test values.
Test–Retest Reliability of Different Target Measurements
Test and retest results using the large light, large figure, small light, and small figures were identical in 6.7% of subjects with all 4 targets in both sessions and were within 5 PD in 78.3%. The overall intraclass correlation coefficient of repeated examinations with 4 different targets was 0.955 (95% confidence interval, 0.937 to 0.992). Table shows the intraclass correlation coefficient matrix of all pairs of measurements using different targets at 6 m, together with the half-width of the 95% limit of agreement for each target pair. The half-width of the 95% limit of agreement ranged from 3.0 to 6.0 PD. The large light and small figure pair demonstrated the greatest variability (4.3 to 6.0 PD). However, it was within the range of interobserver variability using conventional accommodative targets (small figure), of which the half-width of the 95% limit of agreement was 6.3 to 6.5 PD. All the other measurement pairs showed no significant differences in angular deviation.
| Limits of Agreement a (PD) and Interitem Correlation Matrix of Single-Measure Pairs b | Intraclass Correlation Coefficient b (95% CI) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Target | Large Light | Large Figure | Small Light | Small Figure | Large Light Repeat | Large Figure Repeat | Small Light Repeat | Small Figure Repeat | |
| Large light | 1.000 |
|
|
|
|
|
|
| 0.955 (0.937 to 0.992) |
| Large figure |
| 1.000 |
|
|
|
|
|
| |
| Small light |
|
| 1.000 |
|
|
|
|
| |
| Small figure |
|
|
| 1.000 |
|
|
|
| |
| Large light repeat |
|
|
|
| 1.000 |
|
|
| |
| Large figure repeat |
|
|
|
|
| 1.000 |
|
| |
| Small light repeat |
|
|
|
|
|
| 1.000 |
| |
| Small figure repeat |
|
|
|
|
|
|
| 1.000 | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


