This article discusses the development, evaluation, and growth of telemedicine in Alaska. Store-and-forward telemedicine has been used to deliver ear, nose, and throat (ENT) care to rural Alaska since 2002. It has proved valuable in the treatment of many conditions of the head and neck, and it is particularly well suited for the diagnosis and treatment of ear disease. Usage has grown steadily as telemedicine has become widely accepted. Store-and-forward telemedicine has been shown within the Alaska Native Health System to improve access for care and reduce wait times, as well as decrease travel-associated costs for patients.
- •
Store-and-forward telemedicine is well suited to the specialty of otolaryngology.
- •
Clinician involvement in selecting medical devices, creating protocols, and improving and modifying software are key to the success of a telemedicine program.
- •
Referring providers in Alaska believe that the use of telemedicine improves both clinical outcomes and patient satisfaction.
- •
The combination of high-quality images of the tympanic membrane and tympanometry data allows a diagnosis to be established in most telemedicine cases involving ear disease.
- •
Consultants using telemedicine should always have the options of recommending a traditional face-to-face encounter when appropriate care cannot be delivered solely through the telemedicine encounter.
- •
For facial trauma and facial plastics, review of images before seeing the patient has proved invaluable for consulting ear, nose, and throat (ENT) surgeons.
- •
A telemedicine system must have robust processes for initial and ongoing training, technical and clinical support, and technology assessment.
Historically, Alaska Native and Canadian First Nations populations have been burdened with a high prevalence of otitis media and associated morbidity. The incidence of ambulatory care visits related to otitis media for American Indian and Alaska Native children is twice that for all US infants, and the placement rate for tympanostomy tubes in these children younger than 5 years of age was 20 times higher in Alaska compared with the continental United States. In addition, Alaska has an ongoing shortage of physicians, nurses, and allied health professionals, especially in rural and remote areas. The ratio of physicians to population is less than the national average (2.05 MDs per 1000 population in Alaska vs 2.38 in the United States) and Alaska has the sixth lowest physician/population ratio in the nation. The lack of access to medical specialty care, coupled with the high prevalence of ear disease, created a powerful motivator to develop innovative ways to extend the reach of physicians into rural Alaska.
The ear, nose, and throat (ENT) Department at the Alaska Native Medical Center (ANMC) initiated a telemedicine program in 1999 to help provide comprehensive ENT care. The ENT Department resides within ANMC, a 150-bed, level II trauma center in Anchorage, Alaska, that provides specialty and tertiary care for the 130,000 Native Alaskans throughout the state. Most Alaska Natives live outside Anchorage in small communities and many live in remote villages only accessible by air travel. The ENT Department provides otolaryngology clinics at the Anchorage facility (daily) and at field clinics held at 6 regional hospitals (every 2–6 months). Patients living in rural Alaska need to travel to the regional hospital or Anchorage for the specialty clinic services. The need to service this remote population was the driving force to implement a better alternative for care delivery.
The technology
Store-and-forward telemedicine (electronic consultation) is well suited to augmenting otolaryngology services. Store-and-forward telemedicine is an asynchronous communication that allows the sender to take the necessary time to collect data from the patient and then send the case, which the consulting physician can later read and respond to when time is available. This method is convenient for the sender and receiver, and allows them to best use their clinical time. Store-and-forward telemedicine supports, replaces, or works with existing methods of communication. For example, scanned documents can replace faxes, and can be easier to find than paper faxes. Electronic data capture and keyboard entry removes the need for faxes and scans altogether. A store-and-forward case may remove the need for a telephone call.
Store-and-forward telemedicine (electronic consultation) has advantages compared with videoconferencing telemedicine, including that there is no need to synchronize the referring and consulting providers’ time, no need to schedule a session using a videoconferencing network and bridge, low bandwidth requirements, minimal technical support needs, documentation of multimedia data for future reference, the potential for electronic data integration into electronic health records, and tracking of cases for time studies and administrative purposes.
The ENT Department uses the Alaska Federal Health Care Access Network (AFHCAN) tConsult store-and-forward software developed by the Alaska Native Tribal Health Consortium (ANTHC) as the primary telemedicine communication tool. The department’s physicians provided clinical advisory expertise during the software development process and served as one of the early deployment sites. The tConsult software is touch screen compatible, color coded for easy navigation, requires minimal training, and integrates with multiple biomedical devices such as the video otoscope, digital camera, self-administered screening audiometer, and tympanometer ( Fig. 1 ). The software provides both a client-server model (for easy capture of data in clinics with poor or intermittent connectivity) and a Web-based interface for a patient-centric consultant display. The software supports secure client-to-server and server-to-server connectivity for a wide range of telecommunications infrastructure. There are a variety of software features that accommodate clinical workflow practices: cases can be sent to individuals or groups, consultants can be advertised locally or shared throughout an enterprise, and cases can be managed immediately or tagged for further work at a later time. Clinical guidelines for diagnosis, treatment, and triage can also be integrated into the software.
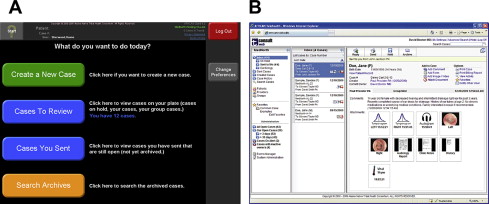
Cases are generated at remote village clinics or regional hospitals by health care providers using an AFHCAN telemedicine cart that includes tConsult software, biomedical peripherals, wireless network capability, and power management hardware ( Fig. 2 ). In Alaska, most of these telemedicine carts are equipped with an audiometer, digital camera, dental camera, electrocardiogram, scanner, spirometer, stethoscope, tympanometer, video otoscope, and vital sign monitor. The ENT Department recognized the need early in the development process of the AFHCAN program for a high-quality video otoscope to visualize and capture images of the tympanic membrane (TM) and related structures. A comprehensive evaluation was conducted on the available video otoscopes, with the conclusion that the highest quality images could be obtained by using the AMD/Welch Allyn 300S Imaging and Illumination platform. Continued use of this video otoscope led to best practices on image acquisition documented as a user’s manual. In time, it was recognized that some blurry images captured by providers were caused by improper focus, leading to the development of a focus tool used for prefocusing the equipment.

The ENT Department also identified the need for tympanometry to be used in the field to supplement visualization of the TM. A review was conducted to identify an appropriate tympanometer that was easy to use and was reliable in the typical remote clinic setting. This combined audiometer/tympanometer was integrated into the AFHCAN telemedicine cart and has since been a useful tool for ear and hearing assessment. Similar reviews were conducted to choose the most appropriate digital camera for dermatologic and facial imaging.
The ENT Department continues to work closely with the ANTHC Telehealth Department to review and identify the best equipment for store-and-forward telemedicine applications. The need for a systematic, objective, and collaborative approach for selecting appropriate medical peripheral devices cannot be overemphasized because these tools become the eyes and ears for specialist operating at great distances from the patient.
Validation and clinical buy-in
AFHCAN telemedicine carts were placed in all of the ENT Department examination rooms early in the project. Staff were introduced and trained on the telemedicine software and instructed on the use of the digital cameras and video otoscopes. Physicians initially used the equipment mostly for preoperative and postoperative images of the TMs and facial lesions. Later, the equipment was adapted for intranasal and laryngeal imaging. The carts were used as image acquisition stations for clinical documentation and archiving. The system was especially useful for patient education (eg, highlighting TM disorders and explaining the related middle ear problems). The staff quickly became experts on the hardware, software, and imaging techniques. They became comfortable receiving cases from the rural referring providers, could act as a resource for referring providers for matters related to image acquisition and case creation, and, most importantly, began to think creatively about the possible clinical applications of the technology. In retrospect, engaging the consultant providers in this way was a critical step in the development of the ENT telemedicine effort.
Although the benefits of video-otoscopy seemed obvious, there was little evidence to support its use as a means of providing clinical care. An initial study was conducted to determine whether TM images could be reliably used to substitute for in-person ENT care, comparing video-otoscopy with the in-person microscope examination for tympanostomy tube follow-up. Forty patients who had tympanostomy tube placement in both ears were independently examined in person by 2 otolaryngologists and imaged locally by an expert telemedicine trainer/imager using a video otoscope and telemedicine software package. The 2 physicians later reviewed images at 6 and 12 weeks. For both physicians, the intraprovider concordance (agreement) between the in-person examination and the corresponding image review was high for each of the physical examination findings. The otolaryngologists were confident in their diagnosis, and confidence increased when cases with poor images were excluded ( Table 1 ).
| “Please Rate how Confident you are in the Diagnosis/Assessment Using Telemedicine in this Case” | ||||||
|---|---|---|---|---|---|---|
| [Blank] | 1 = Not Confident at all | 2 | 3 = Somewhat Confident | 4 | 5 = Very Confident | |
| Provider AA | 0 | 5 | 7 | 14 | 33 | 21 |
| Provider BB | 1 | 2 | 4 | 10 | 23 | 40 |
| Total | 1 | 7 | 11 | 24 | 56 | 61 |
| (1%) | (4%) | (7%) | (15%) | (35%) | (38%) | |
| “Please Rate how Confident you are in the Diagnosis/Assessment using Telemedicine in this Case” | ||||||
|---|---|---|---|---|---|---|
| [Blank] | 1 = Not Confident at all | 2 | 3 = Somewhat Confident | 4 | 5 = Very Confident | |
| Provider AA | 0 | 1 | 4 | 12 | 33 | 21 |
| Provider BB | 2 | 0 | 2 | 5 | 22 | 40 |
| TOTAL | 2 | 1 | 6 | 17 | 55 | 61 |
| (1%) | (1%) | (4%) | (12%) | (39%) | (43%) | |
In a later study, TM imaging was performed by Community Health Aide/Practitioners (CHAP) on 35 patients in remote Alaska. The patients were then flown to the regional facility where they were examined in person by 2 otolaryngologists. Images were later reviewed at 8 and 14 weeks. Similar to the first study, intraprovider concordance for physical examination findings was high ( Fig. 3 ): tube in, 94% to 97% (κ = 0.89–0.94); tube patent, 94% to 97% (κ = 0.89–0.94); drainage, 90% to 96% (κ = 0.04–0.38); perforation, 90% to 96% (κ = 0.61–0.82); granulation, 97% to 100% (κ = 0.49–1.0); middle ear fluid, 88% to 96% (κ = 0.28–0.71); retracted, 83% to 91% (κ = 0.26–0.58). Although there were differences in the findings for the patients in person and later through images, this intraprovider agreement approximated the level of agreement found between 2 providers both seeing the patient in-person, which is the gold standard.
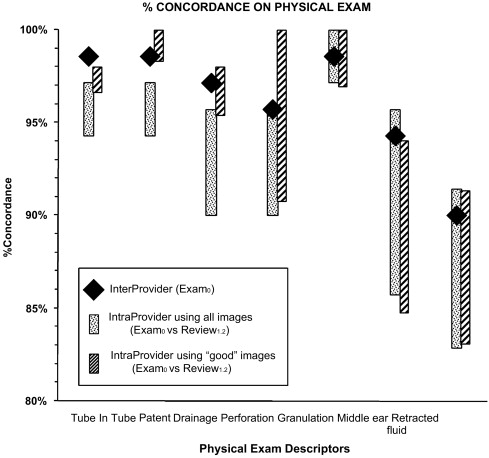
The overall conclusions drawn from these studies were that (1) the differences between viewing images and viewing TM in person were no different than the differences observed between 2 providers both viewing the patients in person, and (2) the results did not vary when images were taken in ideal conditions by an expert or when the images were taken by local providers in the remote village clinics.
Validation and clinical buy-in
AFHCAN telemedicine carts were placed in all of the ENT Department examination rooms early in the project. Staff were introduced and trained on the telemedicine software and instructed on the use of the digital cameras and video otoscopes. Physicians initially used the equipment mostly for preoperative and postoperative images of the TMs and facial lesions. Later, the equipment was adapted for intranasal and laryngeal imaging. The carts were used as image acquisition stations for clinical documentation and archiving. The system was especially useful for patient education (eg, highlighting TM disorders and explaining the related middle ear problems). The staff quickly became experts on the hardware, software, and imaging techniques. They became comfortable receiving cases from the rural referring providers, could act as a resource for referring providers for matters related to image acquisition and case creation, and, most importantly, began to think creatively about the possible clinical applications of the technology. In retrospect, engaging the consultant providers in this way was a critical step in the development of the ENT telemedicine effort.
Although the benefits of video-otoscopy seemed obvious, there was little evidence to support its use as a means of providing clinical care. An initial study was conducted to determine whether TM images could be reliably used to substitute for in-person ENT care, comparing video-otoscopy with the in-person microscope examination for tympanostomy tube follow-up. Forty patients who had tympanostomy tube placement in both ears were independently examined in person by 2 otolaryngologists and imaged locally by an expert telemedicine trainer/imager using a video otoscope and telemedicine software package. The 2 physicians later reviewed images at 6 and 12 weeks. For both physicians, the intraprovider concordance (agreement) between the in-person examination and the corresponding image review was high for each of the physical examination findings. The otolaryngologists were confident in their diagnosis, and confidence increased when cases with poor images were excluded ( Table 1 ).
| “Please Rate how Confident you are in the Diagnosis/Assessment Using Telemedicine in this Case” | ||||||
|---|---|---|---|---|---|---|
| [Blank] | 1 = Not Confident at all | 2 | 3 = Somewhat Confident | 4 | 5 = Very Confident | |
| Provider AA | 0 | 5 | 7 | 14 | 33 | 21 |
| Provider BB | 1 | 2 | 4 | 10 | 23 | 40 |
| Total | 1 | 7 | 11 | 24 | 56 | 61 |
| (1%) | (4%) | (7%) | (15%) | (35%) | (38%) | |
| “Please Rate how Confident you are in the Diagnosis/Assessment using Telemedicine in this Case” | ||||||
|---|---|---|---|---|---|---|
| [Blank] | 1 = Not Confident at all | 2 | 3 = Somewhat Confident | 4 | 5 = Very Confident | |
| Provider AA | 0 | 1 | 4 | 12 | 33 | 21 |
| Provider BB | 2 | 0 | 2 | 5 | 22 | 40 |
| TOTAL | 2 | 1 | 6 | 17 | 55 | 61 |
| (1%) | (1%) | (4%) | (12%) | (39%) | (43%) | |
In a later study, TM imaging was performed by Community Health Aide/Practitioners (CHAP) on 35 patients in remote Alaska. The patients were then flown to the regional facility where they were examined in person by 2 otolaryngologists. Images were later reviewed at 8 and 14 weeks. Similar to the first study, intraprovider concordance for physical examination findings was high ( Fig. 3 ): tube in, 94% to 97% (κ = 0.89–0.94); tube patent, 94% to 97% (κ = 0.89–0.94); drainage, 90% to 96% (κ = 0.04–0.38); perforation, 90% to 96% (κ = 0.61–0.82); granulation, 97% to 100% (κ = 0.49–1.0); middle ear fluid, 88% to 96% (κ = 0.28–0.71); retracted, 83% to 91% (κ = 0.26–0.58). Although there were differences in the findings for the patients in person and later through images, this intraprovider agreement approximated the level of agreement found between 2 providers both seeing the patient in-person, which is the gold standard.
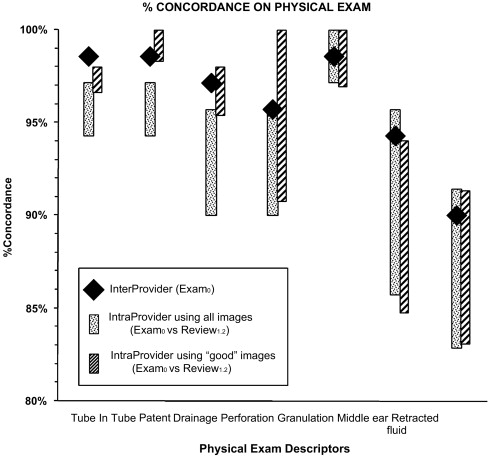
The overall conclusions drawn from these studies were that (1) the differences between viewing images and viewing TM in person were no different than the differences observed between 2 providers both viewing the patients in person, and (2) the results did not vary when images were taken in ideal conditions by an expert or when the images were taken by local providers in the remote village clinics.
Uses
Uses for telehealth at ANMC have grown significantly since the first cases were received in March 2002 ( Fig. 4 ). The ENT Department at ANMC has now responded to 9559 specialty telehealth consultation requests up to and including the most recent reporting date (12/31/2009). These cases were involved in the care delivery to 5751 Alaska Natives, and the involvement of more than 500 providers who created the telehealth cases. The most prevalent ICD9 primary diagnostic codes associated with the consultation requests were 384.2 (Perforation of tympanic membrane), 381.1 (Chronic serous otitis media), and 382.9 (Unspecified otitis media), accounting for approximately 33% of all cases.
The ENT Department has developed a process for responding to telehealth consultations in which a single provider has the daily responsibility to respond to that day’s influx of telehealth consultation requests. The responsibility is rotated between providers, but this process allows the Department to turn around almost 75% of all telehealth cases in the same workday on which they are sent to ANMC from remote sites, and a 90% response rate within 24 hours ( Fig. 5 ). This rapid turnaround time has continuously improved since 2002 because of process improvement within the ENT Department, and improved capabilities and features within the AFHCAN software to minimize the time involvement of ENT providers. The process is efficient enough to provide a 60-minute response rate to almost 30% of all cases, at times producing a specialty consultation response before the patient has left the remote clinic.
Providers that created cases to send to the ENT Department were asked to evaluate the system through a series of questions built into the AFHCAN software. These results, summarized in Table 2 , indicate that more than 90% of providers sending consultation requests to the ENT Department believe that the system improves the quality of care for the patient and helps them communicate with the specialists, and find the software easy to use. A slightly smaller percentage, but still more than 5 of every 6 providers, believes that the system improves patient satisfaction and is satisfied and comfortable with the technology.
| “Please Rate the Following Statement”: | Agree or Strongly Agree (%) |
|---|---|
| Telemedicine will improve the quality of care for this patient (n = 248) | 93 |
| Telemedicine helps me communicate with a doctor (n = 282) | 92 |
| The software is easy to use (n = 266) | 91 |
| I am comfortable creating a telemedicine case (n = 319) | 87 |
| Telemedicine improved patient satisfaction (n = 245) | 87 |
| I am satisfied with how the equipment worked (n = 241) | 86 |
| Telemedicine makes my job more fun (n = 284) | 83 |
| The telemedicine system played a role in educating this patient (n = 260) | 67 |
Clinical applications
The Alaska experience has shown that store-and-forward telemedicine using digital images has multiple applications in the diagnosis and treatment of ear disease. Care has been provided to large numbers of patients with otitis media, TM perforations, myringitis, otitis externa, and hearing loss. Store-and-forward telemedicine has also proved useful for managing lesions of the oral cavity and oropharynx, laryngeal disorders, and problems related to facial plastics and facial trauma. In addition, this technology is being used increasingly for case management, facilitating triage, and helping to eliminate scheduling mistakes and loss of information.
Otitis Media
A good-quality image of the TM is often sufficient to diagnose acute or serous otitis media. Adequate focus, illumination, field of view, and color balancing before imaging are critically important. The validation studies referenced earlier indicated that images alone were, at times, insufficient when assessing problems related to middle ear pressure and TM mobility. An integrated tympanometer was added to the telemedicine cart and has proved to be a valuable addition, because the combination of images of the TM and tympanometry allows for diagnosis and treatment planning in most cases. Obstruction of the ear canal with cerumen, debris, or drainage prevents imaging in a minority of cases, and these need to be examined in a traditional face-to-face manner.
A recommendation for placement of pressure-equalizing tubes (PETs) rests on multiple factors, including the individual patient history, the appearance of the TM, audiologic and tympanometric data, and knowledge of current guidelines for when PETs are indicated. This information can be packaged into a store-and-forward telemedicine case for consideration by the consultant. In addition, through the collaborative efforts of clinicians and software developers, accepted clinical guidelines for PET placement have been incorporated into the software to seamlessly assist referring providers in following guidelines when referring patients. The interactive nature of store-and-forward telemedicine also makes it easy to request additional information on cases when necessary. Because the decision to place PETs often depends on the changes in clinical features with time (the appearance of a retracted TM, for example), the image archive that can be created as a result of serial store-and-forward cases on a given patient can be useful in monitoring for clinically relevant changes.
TM Perforations
We generally recommend repair of TM perforations for all otherwise healthy patients, beginning around age 6 years. Several factors influence the decision to offer elective tympanoplasty, including the patient history, the hearing and speech development status, the tympanometry results, and the appearance of both ears. In most cases, all of these factors can be effectively communicated and assessed using store-and-forward telemedicine. It is now routine in our practice to schedule elective tympanoplasty based on a store-and-forward telemedicine case, meeting the patient for the first time the day before surgery at the preoperative assessment and counseling appointment. A retrospective assessment of this practice (discussed later) indicates that both the operation needed and the operative time can be estimated as accurately from a store-and-forward telemedicine case as it can from a face-to-face encounter. Patient satisfaction with this practice has been high, with patients always having the option of foregoing telemedicine and choosing instead a traditional face-to-face consultation. Postoperative follow-up can also be readily accomplished using telemedicine, and patients from distant locations can be followed closely and for extended periods of time if necessary.
The experience using store-and-forward telemedicine for chronic ear disease brings up an important point: a clinician can decide at any point that a patient must be seen for an in-person examination, assessment, and counseling before a treatment decision is made. Even in these cases, the use of telemedicine provides background information and historical data for review before the patient encounter, making the in-person examination more focused and productive. In more complex cases in which imaging and ancillary studies are needed, arrangements for these can be made before the encounter.
Hearing Loss
Store-and-forward telemedicine is an effective tool for the assessment of previously undiagnosed hearing loss. The combination of history, images of the TM, audiogram, tympanometry, and, at times, otoacoustic emissions (OAEs) in almost all cases identifies conductive, neurosensory, or mixed hearing loss. For conductive losses, the cause is usually readily apparent and treatment can be planned. For neurosensory losses, those needing further evaluation can be identified and triaged, as in significant asymmetry. One of the most gratifying uses for store-and-forward telemedicine has been providing medical clearance for hearing aid fitting. In the past, many Native Alaskan elders in remote locations were unable to access hearing rehabilitation services and suffered from progressive hearing loss and its associated social isolation. Many are now assessed by a regional audiologist in their village, medically cleared using telemedicine, and subsequently fitted with a hearing aid, all within their village.
Not all remote regions in Alaska have the services of an audiologist, and a complaint of hearing loss cannot be addressed without some objective assessment of hearing. An automated audiometer has been integrated into the telemedicine cart and made available to clinics and providers who are unable to access the services of an audiologist. Although this device does not differentiate neurosensory from conductive losses, it does provide enough information to assist the consultant in making initial treatment and triage recommendations, and has proved to be a valuable addition to the AFHCAN system.
Facial Plastics and Reconstruction
Facial plastic surgeons have known for many years that standardized facial images are critical for documentation, planning, and follow-up of facial lesions and their treatment. Given the complex anatomy of the facial soft tissues and the difficulty that the referring provider often has in describing lesions, an image is probably the most important information that can be provided to the surgeon. We routinely require that images of facial lesions or deformities be sent for our review with the initial request for consultation. Whether the lesions are traumatic or neoplastic in nature, initial triage decisions and treatment planning can be completed before seeing the patient. For some traumatic soft tissue lesions, we have been able at times to advise the treating physician how best to close the wound, preventing the need for patient transfer. Readily available software paint programs can be used to mark images, detailing the specific steps for wound closure for the treating physician. When transfer is required because of the complexity of the lesion or the anticipated repair, the resources needed, such as operating room time, ancillary studies, or equipment, can all be arranged in advance. When image review is used in this way, the chance of finding that a facial lesion is more complex than had originally been described (too complex for an office procedure, for example) has been eliminated. For maxillofacial trauma, software integrating history, digital photography, and radiologic images has been found to be invaluable in triage and treatment planning before transfer of a remotely located patient.
Disorders of the Oral Cavity, Pharynx, and Larynx
Telemedicine is a useful tool for the diagnosis and management of diseases affecting the oral cavity, nasopharynx, pharynx, and larynx. In most cases using existing technology, a skill examiner can capture a high-quality image of a lesion at any of these sites. A portfolio of these images can be useful not only for establishing a diagnosis and treatment plan but also for following disease progression or treatment effect. For example, serial imaging of laryngeal carcinoma throughout treatment has been found by the author to greatly enhance patient education and compliance as well as disease documentation. Imaging the upper aerodigestive tract presents unique challenges. The medical devices needed to capture the highest quality images (dental camera for oral cavity and oropharynx and chip-in-tip flexible laryngoscope for hypopharynx and larynx) are expensive and, because of their high cost, not yet widely available. As these devices proliferate and high-quality images become more readily available, telemedicine applications will become more attractive for these anatomic regions. Capturing the dynamic function of the larynx is essential to diagnose many disorders. Although real-time video teleconferencing has been shown to be effective for this purpose, it requires the simultaneous availability of the patient and providers as well as significant bandwidth. Store-and-forward applications with the capability to asynchronously transfer short (up to 1 minute) video files may offer a more efficient solution. In addition, more intensive training and quality control is required if a nonotolaryngologist will be obtaining images of the nasopharynx or larynx.
Audiologist role
The audiologist can play a critical role in establishing a telemedicine program. Our program has had audiologists in the field who champion telemedicine by adopting the technology, expanding their clinical skills, communicating with the ENT Department, recruiting patients, creating cases, and following up with physician recommendations. Telemedicine allows audiologists to send images, clinical data, and hearing tests on both new and follow-up patients.
The partnership with audiologists proved successful in several ways. Regional ENT clinics were conducted every 2 months and clinics were so full that the typical wait time for scheduling a patient was 4 to 6 months. Regional audiologists began to use telemedicine to present referred patients to the consulting otolaryngologist. Appropriate triage and treatment decisions were made by the otolaryngologist; decisions that frequently obviated the need for the in-person encounter. This made in-person appointments available for other patients. A 16-year retrospective study (1992–2007) of new patient referrals to ENT specialty clinics at the Norton Sound Regional Hospital in Nome, Alaska, revealed that waiting times decreased from an average of 4.2 months before telemedicine to 2.9 months in the first 3 years with telemedicine, and then to 2.1 months in the next 3 years with telemedicine. Before telemedicine, 47% of new patient referrals waited 5 months or more to see an ENT specialist in person, but this decreased to 3% of all new patient referrals once telemedicine had been running for 6 years.
An audiologist can also travel to underserved areas and deliver otolaryngology services if they are empowered with telemedicine technologies. In a study conducted by ANMC and ANTHC, a traveling audiologist visited remote village clinics and created telemedicine cases that included clinical histories, images, audiograms, tympanograms, otoacoustic emission testing, and/or other documents. The otolaryngology consultants reviewed the cases and made treatment and triage recommendations. This system is ongoing for care delivery and has been in operation for the past 6.5 years, during which 67 trips have been made to 14 villages, providing 262 clinic service days. The mean patient encounter time is 32.7 minutes. Most patients received services for problems related to ears and hearing. Almost all patients had audiological testing by receiving tympanometry (90%), audiometry (68%), both (66%), or OAE testing (10%). Treatment plans or clinical intervention resulting from the audiology encounter and store-and-forward otolaryngology consultation are shown in Fig. 6 . The 1987 patient encounters resulted in referral for surgery or special diagnostic testing (27%), referral for monitoring (26%), starting of medications (19%), referral to regional ENT clinic (13%), and referral to another specialty (6%). Approximately 26% of patients did not need to see the otolaryngologist and were triaged out of the specialty clinic.
The total cost to run this project was estimated at $175,000. Travel was avoided for 87% of encounters, resulting in travel cost savings in airfares of $697,090. These services were provided at a significantly lower cost and with fewer burdens to the patients compared with the standard referral system. This efficient care delivery model may be applicable to other specialties.
Surgical planning
Telemedicine cases can be simple, moderate, or complicated. The decision process may result in the patient being reassured, treated, sent for additional testing, or referred to see the ENT specialist in person. Some telemedicine cases are direct referral cases for ENT surgery.
An analysis of a sampling of otologic cases led to the conclusion that store-and-forward telemedicine is as effective as in-person evaluation for planning elective ear surgeries such as tympanoplasty and mastoidectomy. In this study, 45 ear surgeries recommended through telemedicine evaluation were compared with a matched set of 45 surgeries recommended through the standard in-person evaluation process. The surgeries included tympanoplasty with or without canalplasty, mastoidectomy, stapes surgery, and myringoplasty. Telemedicine and in-person evaluation accurately predicted the surgery 89% and 84% of the time, respectively. The average difference of actual time and estimated time for the surgical procedures performed was virtually indistinguishable ( Fig. 7 ) and not statistically different between the 2 groups: 32 minutes for the telemedicine evaluation group and 35 minutes for the in-person evaluation group. Otologic surgeons are able to determine the needed surgery and required operative time as accurately as when patients were seen during a traditional in-person encounter.
Educational content
One of the advantages of store-and-forward telemedicine is the automated collection of images and other multimedia. Recently, the ENT Department collected 28,000 otoscope and digital camera images from telemedicine cases. The best clinical images were reviewed, rated, and into a rich library collection. These images are now being used to develop educational content such as computer-based training for the clinical curricula of various health care providers.
Technology assessment, training, and support
With more than 14,000 store-and-forward cases per year, the Alaska telemedicine system is mature and well integrated into the health delivery system. However, constant work is required to maintain and grow a telemedicine program. New medical devices with potential for use in telemedicine regularly enter the market. A formal process that uses clinical, technical, and software expertise to assess these products is essential; a poor technology decision can devastate a telemedicine program. Technology assessment is resource and knowledge intensive, and is best accomplished by dedicated centers. These centers can assist other programs with their technology decisions. Training and support are also critical ongoing needs. Provider turnover and changes in medical practice and technology are features of the health care environment. Without a robust training and support plan, even the best-conceived telemedicine plan deteriorates and fails as these factors evolve with time.
Impact of this system
The telemedicine system in Alaska is one of the world’s most extensive networks, providing increased access, saved travel costs, and improved quality. The AFHCAN has been in use since 2001 and has resulted in almost 70,000 store-and-forward clinical cases to date. With an ever-growing usage pattern now reaching 14,000 cases per year, this system is involved in care delivery to more than 12,000 Alaskans each year and is now considered an integral part of the day-to-day health care delivery system in the Alaska Tribal Health Systems (ATHS). More than 70% of all consultations prevent patients from having to travel to see specialists, resulting in statewide savings estimated at $3 million to $4 million annually in avoided patient travel costs (airfares). Specific to the ENT Department, 73% of all consultations prevent patient travel, and this has generally been consistent since the program was first adopted in 2002 ( Fig. 8 ). A smaller, but significant, portion of telehealth cases (9% for ENT, 8% for all telehealth cases) cause patient travel, which is to be expected because disease states and various health issues are identified through telehealth, possibly at a much earlier and more easily treated stage in the disease state.
Continued usage of the system depends on many other factors, most notably the subsidies for connectivity provided through the Universal Service Fund subsidies for health care. Alaska also has a supportive reimbursement environment, with most insurers willing to reimburse for telehealth. It is still a struggle to show value to one segment of the health care industry when often the advantages are accrued by a different segment. For example, if payers do not cover travel for patients, the significant savings in patient travel for the health care system do not translate into direct benefits for that particular segment of the industry. This difficulty is perhaps the biggest challenge facing telehealth and the AFHCAN program, justifying the value of telehealth in an environment in which system impacts are less relevant than the direct bottom line impact for individual payer plans and programs.
Programs such as AFHCAN offer great promise for improving access to timely care for patients in remote communities across the Unites States and in many other countries. The success of these programs depends on many factors, perhaps the most important being relevance to the provider community that it serves. The single most important measure of the AFHCAN program is that clinicians not only continue to use it but more clinicians use it with more patients every year.
The authors have nothing to disclose.
References
- 1. Hamman C., and Keeler F.: Eye, ear, nose and throat infections in natives of Alaska. Northwest Med 1957; 56: pp. 423
- 2. The McGroth report: a documentation on the study and prevention of upper respiratory disease. Washington DC: State of Alaska, US Government Printing Office, 1962.
- 3. Baxter J.D.: Otitis media in Inuit children in the eastern Canadian Arctic—an overview—1968 to date. Int J Pediatr Otorhinolaryngol 1999; 49: pp. S165-S168
- 4. Bruneau S., Ayukawa H., Proulx J.F., et al: Longitudinal observations (1987-1997) on the prevalence of middle ear disease and associated risk factors among Inuit children of Inukjuak, Nunavik, Quebec, Canada. Int J Circumpolar Health 2001; 60: pp. 632-639
- 5. Hodgins S.: Health and well-being challenges in Nunavik: health conditions, determinants, and lines of action. Kuujjuaq (QC): Department of Public Health, Nunavik Regional Board of Health and Social Services, 1996.
- 6. Singleton RJ, Holman RC, Plant RL, et al. Otitis media outpatient visits and tympanostomy tube placement rates in young American Indian and Alaska Native children: what are the trends? Abstract in: 2nd International Meeting on Indigenous Child Health. Montreal, April 20–22, 2007.
- 7. Health Resources and Services Administration Web site. US Department of Health and Human Services, 2009.
- 8. Alaska Center for Rural Health : Alaska’s allied health workforce: a statewide assessment. Anchorage (AK): University of Anchorage, 2001.
- 9. Smart D.R., and Sellers J.: Physician characteristics and distribution. Chicago: American Medical Association, 2008.
- 10. Kokesh J., Ferguson A.S., and Patricoski C.: Telehealth in Alaska: delivery of health care services from a specialist’s perspective. Int J Circumpolar Health 2004; 63: pp. 387-400
- 11. Ferguson A.S.: Video otoscope testing. Final report. Alaska Native Health Board. Anchorage (AK): University of Alaska Anchorage, 1998.
- 12. AFHCAN. User’s manual. Video otoscope, AMD-300S (Welch Allyn/AMD) Document ID: Pub-112. Anchorage (AK): Alaska Native Tribal Health Consortium, 2006.
- 13. Patricoski C., Ferguson A.S., and Tooyak A.: A focus tool as an aid to video-otoscopy. J Telemed Telecare 2003; 9: pp. 303-305
- 14. Patricoski C., and Ferguson A.S.: Which tympanometer is optimal for an outpatient primary care setting? J Fam Pract 2006; 55: pp. 946-952
- 15. Patricoski C., Kokesh J., Ferguson S., et al: A comparison of in-person examination and video otoscope imaging for tympanostomy tube follow-up. Telemed J E Health 2003; 9: pp. 331-344
- 16. Kokesh J., Ferguson A.S., Patricoski C., et al: Digital images for postsurgical follow-up of tympanostomy tubes in remote Alaska. Otolaryngol Head Neck Surg 2008; 139: pp. 87-93
- 17. Norton Sound Health Corp, data on wait time reduction. (Report).
- 18. Kokesh J., Ferguson A.S., Patricoski C., et al: Traveling an audiologist to provide otolaryngology care using store-and-forward telemedicine. Telemed J E Health 2009; 15: pp. 758-763
- 19. Kokesh J., Ferguson A.S., and Patricoski C.: Pre-operative planning for ear surgery using store-and-forward telemedicine. Otolaryngol Head Neck Surg 2010; 143: pp. 253-257
- 20. Hudson H.E.: Rural telemedicine: lessons from Alaska for developing regions. Telemed J E Health 2005; 11: pp. 460-467
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


