Purpose
To evaluate the diagnostic value of tear osmolarity and several ocular surface parameters in screening for ocular surface alterations in ocular graft-vs-host disease (GVHD) patients.
Design
Case-control study.
Methods
Sixty-three patients with ocular GVHD and 74 healthy participants were screened for ocular surface changes using the Ocular Surface Disease Index (OSDI), tear osmolarity, Schirmer test, tear break-up time (TBUT), and fluorescein corneal staining. The severity of ocular GVHD was diagnosed according to the National Institutes of Health (NIH) grading system. The diagnostic sensitivity and specificity and cutoff values were determined for each ocular parameter using a receiver operating characteristic (ROC) curve and area under the curve (AUC) analysis. Significance was defined at P < .05.
Results
The tear osmolarity, corneal staining score, and OSDI score gradually increased as the severity of ocular GVHD increased, and Schirmer value gradually decreased as the GVHD grade increased in severity. The Schirmer test showed greatest diagnostic sensitivity and specificity for ocular GVHD (92.1% sensitivity, 85.7% specificity, cutoff = 9 mm), followed by the TBUT (87.3% sensitivity, 75.0% specificity, cutoff = 6 s), tear osmolarity (98.4% sensitivity, 60.7% specificity, cutoff = 311 mOsm/L), corneal staining score (66.7% sensitivity, 82.1% specificity, cutoff = 2), and OSDI score (77.8% sensitivity, 66.1% specificity, cutoff = 20.8).
Conclusions
Multiple diagnostic modalities should be used to detect ocular surface changes in GVHD patients. The severity of ocular GVHD can be effectively monitored using tear osmolarity; however, additional studies are required.
Dry eye disease (DED), or keratoconjunctivitis sicca (KCS), is one of the most common complications of ocular graft-vs-host disease (GVHD) after patients undergo allogeneic hematologic stem cell transplantation. The prevalence of ocular GVHD varies greatly, ranging from 60% to 90%. Chronic GVHD arises when primarily donor-derived immunocompetent cells are activated by host tissue antigen and initiate inflammation in numerous target organs. Sustained inflammation in the eye damages the conjunctiva, lacrimal glands, and meibomian glands by inducing fibrosis. If the inflammation is left untreated, then the ocular surface will be permanently and irrecoverably damaged. Therefore, detecting inflammation during the early stage of ocular GVHD is a valuable tool for practitioners.
Several tools exist to diagnose ocular surface deterioration, including subjective symptom questionnaire, tear break-up time (TBUT), Schirmer test, and fluorescein corneal staining. However, these methods are limited by their lack of objectivity and specificity and by their interobserver variation. In 2005, a working group at the National Institutes of Health (NIH) developed minimal criteria by consensus for the clinical diagnosis of chronic GVHD (cGVHD). The guidelines proposed that a mean Schirmer score of less than 5 mm or an acute case of KCS with a Schirmer score of 6–10 mm is sufficient to diagnose ocular cGVHD in patients with at least 1 other organ affected. However, use of the Schirmer test in isolation is considered unreliable.
Tear osmolarity has been shown as the single best marker of disease severity and is a central mechanism in the pathogenesis of ocular surface damage in DED. Recent technological improvements now enable the tear osmolarity test in the office setting with minimal invasiveness. Tear osmolarity is able to reliably detect ocular surface deterioration caused by both nonimmune and immune-associated DED. Therefore, the purpose of this study was to evaluate whether tear osmolarity and ocular surface parameters could serve as reliable markers for diagnosing and monitoring the severity of ocular GVHD.
Methods
This case-control study included 63 subjects diagnosed with ocular GVHD following allogeneic hematologic stem cell transplantation and 74 age-matched subjects as healthy controls. Institutional Review Board approval was obtained, and the study protocol followed the guidelines of the Declaration of Helsinki. Informed consent was obtained from all participants.
All patients received prophylaxis, management, and supportive care for GVHD. The primary treatment for patients with classic acute GVHD (aGVHD) comprised methylprednisolone (2 mg/kg) or an equivalent dose of prednisone. The treatment for steroid-refractory aGVHD varied, as described previously. Treatment of classic chronic GVHD also varied but followed general guidelines, as described previously. Patients with limited disease received topical immunosuppressants, and those with extensive disease were administered calcineurin inhibitors along with systemic steroids.
Inclusion criteria were as follows: ocular GVHD patients diagnosed based on the NIH definition (low Schirmer test value [≤5 mm at 5 min] or newly diagnosed KCS with a moderate Schirmer test value [6–10 mm at 5 min]), exhibiting disease manifestations in at least 1 other organ. Ocular examination was performed by cornea and external eye specialists (N.K.S. and H.K.Y.). Exclusion criteria included active ocular infection or inflammation not associated with dry eye, drug toxicity, and eyelid abnormalities. Subjects using contact lenses, artificial tears within 12 hours of examination, topical steroids, or topical anti-inflammatories, and those with a history of ocular surgery or trauma, were also excluded. Patients using any systemic medication that could interfere with tear production, such as β-blockers, diuretics, benzodiazepines, hormones, and antihistamines, were excluded, except for patients administered systemic immunosuppressive and corticosteroid treatment for systemic GVHD.
Each participant underwent a thorough ophthalmic examination. The following objective tests for DED were performed in order in this single-visit study: Ocular Surface Disease Index (OSDI) questionnaire, tear osmolarity, Schirmer test without anesthesia, slit-lamp examination of the ocular surface to assess TBUT, and corneal fluorescein staining. A 5-minute interval or longer was allotted between the tests, except between the questionnaire and tear osmolarity measurement. Subjective symptoms were graded on a numerical scale from 0 through 4 using the OSDI score as follows: 0, none of the time; 1, some of the time; 2, half of the time; 3, most of the time; and 4, all of the time (from 0 to 100). Tear osmolarity was measured using a handheld device (TearLab Osmolarity System; TearLab Corp., San Diego, CA) to simultaneously collect and analyze the electrical impedance of a 50-nL tear sample from the inferior lateral meniscus. A 5-minute Schirmer test was performed using sterile strips without anesthesia. The Schirmer strip was placed at the notch of the inferior fornix and removed 5 minutes later, and the point of maximum wetting was measured. A Schirmer value of ≤5 mm was considered abnormal. The TBUT was measured by placing a sodium fluorescein strip at the lower tarsal conjunctiva. Each patient was asked to blink, and the time before the corneal defect appeared in the stained tear film was recorded as the TBUT. A TBUT of ≤5 seconds was considered abnormal. For corneal fluorescein staining, the entire cornea was examined with a slit lamp using a yellow barrier filter and cobalt blue illumination. Corneal staining was graded according to the recommendations of the National Eye Institute (NEI) industry workshop report on clinical trials in dry eyes. Both eyes were measured one at a time, and the more severe of the bilateral measurements was used in the analysis.
Normal distribution of the data was verified using the Kolmogorov-Smirnov test. Descriptive statistics for continuous variables are reported as the mean (range). The continuous variables (age, tear osmolarity, Schirmer test, TBUT, and OSDI score) were compared using the Mann-Whitney test, and the categorical variable (sex and corneal staining score) was analyzed using the χ 2 test. The severity of ocular GVHD was staged according to the NIH criteria. Trends were analyzed according to the ocular GVHD stage using the Jonckheere test. The distributions of osmolarity and each grade of ocular GVHD severity, as defined by NIH criteria, were displayed in a box plot. The correlation between the tear osmolarity and each variable was determined using the Spearman correlation. A P value of <.05 was considered statistically significant.
Results
The causative hematologic diseases in the patient population (n = 63) included acute myeloblastic leukemia (n = 25, 39.7%), acute lymphocytic leukemia (n = 12, 19.0%), myelodysplastic syndrome (n = 10, 15.9%), chronic myeloblastic leukemia (n = 1, 1.6%), severe aplastic anemia (n = 8, 12.7%), multiple myeloma (n = 2, 3.2%), and other (n = 5, 7.9%). The mean duration between transplantation and study visit was 425.5 ± 194.3 days. All included patients had chronic systemic GVHD affecting organs other than the eyes, and 44 (69.8%) had a history of acute GVHD before 100 days following undergoing allogeneic hematologic stem cell transplantation. Fifty-five patients (87.3%) received immunosuppressive and/or corticosteroid medication at a minimal dose to control systemic GVHD.
The distributions in the age, sex, underlying etiology, tear osmolarity, Schirmer value, TBUT, corneal staining, and OSDI score are summarized in Table 1 . Female participants were significantly more predominant in the control group compared to the ocular GVHD group. The ocular GVHD group showed a significantly lower Schirmer value and TBUT, and a significantly higher tear osmolarity, corneal staining score, and OSDI score, than the control group. Cicatrical conjunctival changes were present in 2 subjects (11.8%) with Grade 2 (n = 17) ocular GVHD and 5 subjects (38.5%) with Grade 3 (n = 13) ocular GHVD patients.
| GVHD Group | Control Group | P Value | |
|---|---|---|---|
| Number of eyes | 63 | 74 | |
| Sex (male) | 36 (57.1%) | 21 (28.4%) | .0007 |
| Age (y) | 41 (28–50) | 36 (30–48) | .9261 |
| Hematologic diagnosis | |||
| Acute myeloblastic leukemia | 25 (39.7%) | NA | NA |
| Acute lymphocytic leukemia | 12 (19.0%) | NA | NA |
| Myelodysplastic syndrome | 10 (15.9%) | NA | NA |
| Chronic myeloblastic leukemia | 1 (1.6%) | NA | NA |
| Severe aplastic anemia | 8 (12.7%) | NA | NA |
| Multiple myeloma | 2 (3.2%) | NA | NA |
| Other a | 5 (7.9%) | NA | NA |
| Tear osmolarity (osm) | 300 (295–310) | 291 (281–300) | <.0001 |
| Schirmer test (mm) | 5 (4–5) | 13 (10–22) | <.0001 |
| TBUT (s) | 3 (1–5) | 9 (5–10) | <.0001 |
| Corneal staining score | 7 (2–12) | 1 (1–4) | <.0001 |
| OSDI score | 18 (9–29) | 6 (2–13) | <.0001 |
a Other: chronic lymphocytic leukemia, diffuse large B cell lymphoma, peripheral T cell lymphoma, NK/T cell lymphoma, non-Hodgkin lymphoma.
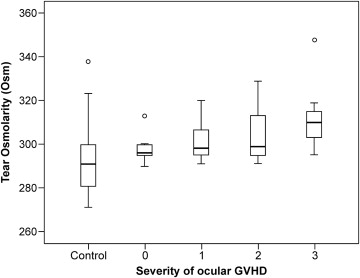
In the ocular GVHD group, the tear osmolarity, corneal staining score, and OSDI score gradually increased as the ocular GVHD severity increased. By contrast, the Schirmer value gradually decreased as the GVHD grade increased in severity ( Table 2 ). In the box plots of the osmolarity distribution in the healthy participants and in those with varying severities of ocular GVHD following allogeneic hematologic stem cell transplantation ( Figure 1 ), the tear osmolarity increased as the GVHD severity increased. Tear osmolarity was significantly and negatively correlated with the Schirmer value (r = −.511, P < .0001) and TBUT (r = −.422, P < .0001) and positively correlated with the corneal staining (r = .475, P < .0001) and OSDI scores (r = .289, P = .0006; Figure 2 ).
| Ocular GVHD Group (n = 63) | |||||
|---|---|---|---|---|---|
| Ocular GVHD Severity by NIH Criteria | |||||
| 0 | 1 | 2 | 3 | P for Trend | |
| Number | 14 | 19 | 17 | 13 | |
| Tear osmolarity (osm) | 296 (295–300) | 298 (295–308) | 299 (295–313) | 310 (303–315) | .0007 |
| Schirmer test (mm) | 6 (4–9) | 5 (3–5) | 5 (5–5) | 4 (3–5) | .0403 |
| TBUT (s) | 3 (1–6) | 4 (3–7) | 3 (1–5) | 2 (1–4) | .1135 |
| Corneal staining score | 1.5 (1–9) | 3 (1–7) | 8 (2–12) | 14 (10–15) | <.0001 |
| OSDI score | 4 (0–10) | 11 (9–16) | 25 (20–27) | 31 (28–37) | <.0001 |

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


