Systemic and odontogenic etiologies of chronic rhinosinusitis, although rare, are an integral consideration in the comprehensive management of patients with sinonasal disease. Proper knowledge and timely recognition of each disease process, with referrals to appropriate consultants, will facilitate treatment, because many of these conditions require both local and systemic therapy. In some instances, medical therapy plays a pivotal role, with surgery being a supplemental treatment technique. We review the most commonly encountered systemic etiologies of chronic rhinosinusitis and odontogenic sinusitis, including clinical presentation, diagnosis, management, and treatment outcomes.
Key points
- •
Cystic fibrosis and primary ciliary dyskinesia result in pansinusitis and inspissated, thick mucopurulent secretions. Surgical therapy requires extended procedures to achieve antrostomies or ventilation and to treat obstructive polyposis.
- •
Patients with sinonasal sarcoidosis tend to present with nasal crusting, anosmia, and epistaxis. The nasal mucosa of the septum and turbinates may demonstrate nodules.
- •
Vasculitides present with lower respiratory tract disease. Medical therapy is the mainstay of therapy, with surgery indicated for severe symptoms, recurrent infections, and anatomic obstruction.
- •
Odontogenic sinusitis should be suspected in any patient with unilateral maxillary sinusitis with a longstanding history of maxillary dental problems or a recent history of a maxillary dental procedure.
- •
Otolaryngologists should personally review imaging studies to look for any bony dehiscence or anomalous connections between the maxillary sinus and the oral cavity.
Introduction
Although the majority of cases are largely attributed to local factors (ie, anatomic, allergic, immunologic, infectious), chronic rhinosinusitis (CRS) may also be caused by systemic or odontogenic disease. It is thus important for otolaryngologists to be aware of systemic and odontogenic etiologies of CRS, and to approach the management of these patients from a multidisciplinary standpoint. A thorough history, with special attention to comorbidities and medical conditions, should be elicited from each patient. Because all of these conditions have manifestations in multiple organ systems, consultations with other specialists should be sought in each case. In this review, we discuss the most common systemic diseases with distinguishing sinonasal manifestations, including cystic fibrosis (CF), sarcoidosis, vasculitides, primary ciliary dyskinesia (PCD), and odontogenic sinusitis.
Introduction
Although the majority of cases are largely attributed to local factors (ie, anatomic, allergic, immunologic, infectious), chronic rhinosinusitis (CRS) may also be caused by systemic or odontogenic disease. It is thus important for otolaryngologists to be aware of systemic and odontogenic etiologies of CRS, and to approach the management of these patients from a multidisciplinary standpoint. A thorough history, with special attention to comorbidities and medical conditions, should be elicited from each patient. Because all of these conditions have manifestations in multiple organ systems, consultations with other specialists should be sought in each case. In this review, we discuss the most common systemic diseases with distinguishing sinonasal manifestations, including cystic fibrosis (CF), sarcoidosis, vasculitides, primary ciliary dyskinesia (PCD), and odontogenic sinusitis.
Systemic etiologies of chronic rhinosinusitis
Cystic Fibrosis
CF is a relatively common autosomal-recessive genetic disorder involving a derangement in the gene encoding the CF transmembrane conductance regulator ( CFTR ). The most common mutation is ΔF508, or deletion of the phenylalanine codon at position 508, of which 1 out of 25 to 30 Caucasians are carriers. This mutation results in restricted efflux of anions, such as chloride and bicarbonate, thus leading to thick, obstructive, inspissated sinobronchopulmonary secretions, further promoting mucosal inflammation and superinfections. The pancreas and reproductive systems are also affected, frequently leading to exocrine insufficiency and male infertility, respectively. More recent studies have classified CF patients as either high or low risk based on CFTR genotype, with an apparent impact on prognosis. Specifically, high-risk CF patients have an earlier age of diagnosis, worse pulmonary status (ie, lower forced expiratory volume at 1 second), increased colonization by Pseudomonas aeruginosa , increased sweat chloride, and worse overall survival.
Patients tend to present with clinical manifestations of CF at a young age. A history of recurrent sinonasal and bronchopulmonary infections in a child should prompt consideration of a workup for CF. Similarly, the finding of nasal polyposis in a child is suggestive of unrecognized CF, occurring in one-third to one-half of patients. On computed tomography (CT) imaging of the sinuses, CF patients tend to have hypoplasia of all sinuses ( Fig. 1 ). In a study by Ferril and colleagues, comparison of high- and low-risk CF patients additionally found that high risk-patients are even more likely to have sinus hypoplasia. CF patients also tend to develop mucoceles. Throughout their lives, CF patients require close care by pulmonologists, gastroenterologists, geneticists, otolaryngologists, respiratory therapists, and nutritionists to optimize their medical condition and preserve functional status.
Newborn screening for CF using serum immunoreactive trypsinogen and genetic testing for CFTR mutations is now nearly universal in the United States. A diagnosis of CF can be made by (1) clinical signs and symptoms indicative of the diagnosis and (2) one of the following: (a) abnormal sweat chloride test on 2 separate occasions, (b) having 2 disease-causing mutations in CFTR , or (c) an abnormal nasal potential difference (less commonly used). The most commonly used diagnostic tool is the sweat chloride test, which is deemed abnormal if 60 mmol/L or greater and borderline if between 40 (30 for age <6 months) and 59 mmol/L. Although the test is generally reliable, it may nevertheless miss CF diagnoses up to 3 years of age.
Management principles of CF-related CRS somewhat parallels that of non-CF CRS patients, although coordination with other disciplines is important. Medical therapy frequently involves nasal irrigations and dornase alfa (recombinant deoxyribonuclease) to clear thick secretions, topical and oral corticosteroids to ameliorate mucosal inflammation, and antibiotics for acute infections. Liang and colleagues in a systematic review found that, of these therapies, dornase alfa and topical corticosteroids were associated with significant clinical improvement for CF-related CRS.
Surgical therapy for CF patients is individualized, and may be indicated for patients who have persistent symptoms after medical therapy, have obstructive nasal polyps and mucoceles, develop chronic or recurrent bronchopulmonary infections from rhinogenic flora, and prophylactically before lung transplantation. As opposed to reestablishing mucociliary clearance in non-CF patients, the role of surgery is to promote gravitational drainage of secretions. Often, this plan includes extended procedures such as a mega-antrostomy in place of a standard maxillary antrostomy. Several studies have highlighted significant improvements in quality-of-life after endoscopic sinus surgery (ESS). This finding is corroborated by another systematic review by Liang and colleagues, which found that ESS seems to improve symptoms and endoscopy scores, although the impact on lower airway disease is unknown. In the senior author’s experience, ESS for CF patients seems to produce clinical improvement in pulmonary disease, and is thus recommended for medically suitable candidates. Most CF patients tolerate ESS in an outpatient setting. Soudry and colleagues found in a cohort of 33 CF patients that postoperative pain, but not preoperative medical condition (eg, pulmonary function), was associated with inpatient admission after ESS for CF-related CRS, underscoring the importance of careful postoperative monitoring.
Another consideration is the impact of prophylactic ESS in CF patients before lung transplantation. Some experts have found that ESS not only seems to decrease Pseudomonas colonization and subsequent bronchopulmonary infections, but also decreases the risk of bronchiolitis obliterans and improves posttransplant survival. In contrast, Leung and colleagues found in a retrospective review of 87 CF lung transplant patients who underwent pretransplant ESS that bacterial recolonization occurred in 87% of cases within the course of several weeks postoperatively, with no change in survival as compared with those who did not undergo ESS. Prospective studies are required to define the clinical impact of ESS in patients with CF who undergo lung transplantation.
Both within the discipline of rhinology and beyond, novel therapeutic strategies for CF remain an active area of investigation. One proposed strategy to ameliorate the inflammatory consequences of CF-related CRS is through restoration of mucociliary clearance by administering “secretagogues,” which promote transepithelial ionic transport. Recently, pharmacologic agents, especially those found naturally or within herbal medications, such as hesperidin, chlorogenic acid, Sinupret (Bionorica, Neumarkt, Germany), quercetin, and resveratrol, or CFTR modulators such as genistein, VRT-532, and UCCF-152, have been demonstrated to have such properties based on both in vitro (human) and in vivo (murine and/or porcine) models. Using the same experimental models, tobacco smoke and hypoxia have been found to suppress transepithelial ion transport, worsening mucociliary clearance. Resveratrol in particular has been extensively studied and has been shown to restore mucociliary transport in a model of acquired CFTR deficiency (simulating CF). Such therapies are extremely promising in expanding the arsenal of medical management for CF-related CRS.
Sarcoidosis
Sarcoidosis is a systemic granulomatous disease that primarily manifests in the respiratory tract, particularly the lungs in the form of bilateral, diffuse interstitial lung disease. Other organs that may be involved include the skin, eye, heart, endocrine system, and gastrointestinal tract. Although it may affect all races, sarcoidosis is 3 to 4 times more common among blacks, and tends to be more severe in this population. The pathophysiology is unclear, but involves genetic predisposition and modification by environmental factors, ultimately leading to immune dysfunction. Histopathologically, the hallmark of diagnosis is the presence of noncaseating granulomas. The standard workup should include chest radiography (bilateral hilar adenopathy) and laboratory testing (serum angiotensin converting enzyme), with biopsy considered for more accessible sites (eg, skin, nasal cavity), and the diagnosis is made through clinical, radiographic, and histopathologic data.
Sarcoidosis presenting in the sinonasal tract is rather rare, involving only approximately 1% of sarcoidosis cases. CRS likely results through granulomatous destruction of nasal mucosa and surrounding structures (eg, cilia, olfactory fibers, vasculature), creating a drying effect and local tissue destruction (ulceration and perforation). Because the sinonasal signs and symptoms are rather nonspecific (nasal obstruction, crusting, epistaxis), rhinologic manifestations of sarcoidosis, especially at initial presentation, may be easily missed. In 1999, deShazo et al proposed diagnostic criteria to aid in the diagnosis of sinonasal sarcoidosis: (1) radiologic evidence of sinusitis, (2) histopathologic confirmation of noncaseating granuloma in the sinus tissue supported by negative stains for fungus and acid-fast bacilli, (3) negative serologic test results for syphilis and antineutrophil cytoplasmic antibodies (ANCA), and (4) no clinical evidence of other disease processes associated with granulomatous nasal and sinus inflammation. The authors revisited this topic in 2010 and, in reviewing the most common rhinologic manifestations of 36 sarcoidosis patients, found that having 2 of the signs of nasal crusting, anosmia, and epistaxis in a patient with CRS was highly specific for sinonasal sarcoidosis. Other reports have commented on the presence of a nodular appearance of the nasal mucosa overlying the septum and turbinates, which can be readily seen on endoscopy.
The mainstay of treatment for sarcoidosis is medical, with symptomatic patients typically treated with systemic corticosteroids. Patients who have persistent disease refractory to corticosteroids may be tried on immunosuppressants (methotrexate, azathioprine, infliximab). In a case control study, Aubart and colleagues found that patients with sarcoidosis with sinonasal involvement tend to be more difficult to treat medically, requiring more frequent and longer durations of therapy. This observation was corroborated by Long and colleagues in another retrospective study involving 6 patients with sinonasal sarcoidosis. Although no specific studies have examined this phenomenon, local medical treatments for the nasal cavity and sinuses may include nasal irrigations, corticosteroids (topical, intralesional, systemic), and antibiotic therapy (topical and systemic), although these therapies are secondary to primary systemic treatment.
The role of surgery for sarcoidosis-related CRS is limited, and should be reserved for patients with severe symptoms attributable to anatomic factors (eg, septal deviation, polyposis, ostiomeatal complex obstruction, scarring, mucocele) or recurrent infections ( Fig. 2 ). The only study reviewing ESS for sarcoidosis patients included 6 patients, with symptomatic improvement and decreased steroid use in all cases. In rare cases, patients with unrecognized sarcoidosis (asymptomatic or minimal symptoms) may have primary sinonasal complaints, and the diagnosis may be made after ESS. In the senior author’s experience, sarcoidosis-related CRS patients tend to have a higher rate of synechiae formation, and thus the decision to consider surgery should be weighed against the potential need for vigilant postoperative care and the potential for an outcome that may be compromised by the patient’s underlying inflammatory response. These patients should be referred to a pulmonologist for further workup and consideration of treatment, if indicated.

Eosinophilic Granulomatosis with Polyangiitis (Churg-Strauss Syndrome)
Previously known as Churg-Strauss syndrome or allergic granulomatosis and angiitis, eosinophilic granulomatosis with polyangiitis (EGPA) is an autoimmune vasculitic condition involving small- and medium-sized arteries. Most commonly, EGPA affects the upper and lower respiratory tracts in the form of allergic rhinitis, CRS, and asthma, but can additionally involve the ear (otitis media, middle ear effusion), peripheral nervous system (neuropathy), heart (cardiomyopathy, pericarditis, arrhythmia), kidneys (acute renal insufficiency), and gastrointestinal tract (eosinophilic gastroenteritis). In fact, sinonasal involvement is common (≤70% of cases), and can manifest as nasal polyposis (60%–70%), crusting, rhinorrhea, anosmia, sneezing, mucopurulent discharge, epistaxis, and septal perforation. The disease progresses in a distinct clinical pattern, although occasionally stages may overlap or not occur at all :
- 1.
Prodromal phase (allergic rhinitis, asthma)
- 2.
Eosinophilic phase (serum eosinophilia, progressive pulmonary involvement)
- 3.
Vasculitic phase (granulomatosis, constitutional symptoms)
One of the hallmarks of EGPA is serum and tissue eosinophilia. Furthermore, approximately 50% of patients will test positive for ANCA (p-ANCA, or antimyeloperoxidase antibodies, in 70% of cases). Although lung biopsy is the gold standard for tissue diagnosis, skin or nerve biopsy is less invasive and thus preferred. Based on the American College of Rheumatology guidelines, a diagnosis of EGPA is highly suggested (85% sensitivity, 99.7% specificity) with 4 or more of the following criteria: (1) asthma (history of and/or active wheezing), (2) greater than 10% eosinophils on differential leukocyte count, (3) peripheral neuropathy, (4) migratory or transient pulmonary opacities on radiologic imaging, (5) rhinosinusitis, and (6) a biopsy containing blood vessel showing eosinophilic accumulation in extravascular areas. Consultation with a rheumatologist is recommended.
Similar to sarcoidosis, treatment is primarily medical, with systemic corticosteroids playing a key role. For patients with multiorgan involvement or severe disease, cyclophosphamide is added to corticosteroids. Once remission is achieved, patients can be switched to maintenance therapy with less toxic immunosuppressants, such as methotrexate or azathioprine. Patients tend to respond well to treatment, with survival greater than 90% at 5 years based 1 study of 118 patients. For sinonasal involvement, nasal irrigations, topical corticosteroids, and antibiotics may be indicated for symptomatic relief.
Because EGPA is a rare condition, no prospective or retrospective analyses of the impact of surgical therapy have been conducted. If the clinical history is suspicious and surgery is planned, surgically removed sinonasal contents should be sent for histopathologic analysis to seek a possible diagnosis. An appropriate strategy for the management of patients with patients is aggressive, timely primary management of systemic disease, with ESS reserved for anatomic obstruction or recurrent infections.
Granulomatosis with Polyangiitis (Wegener’s Granulomatosis)
Granulomatosis with polyangiitis (GPA), formerly known as Wegener’s granulomatosis, is a small- and medium-sized vessel vasculitis affecting primarily the upper and lower respiratory tract and the renal system. The American College of Rheumatology criteria for GPA includes (1) nasal or oral inflammation (oral ulcers, nasal discharge), (2) abnormal chest radiograph showing nodules, infiltrates, or cavitations, (3) abnormal urinary sediment (microscopic hematuria with or without red cell casts), and (4) granulomatous inflammation on biopsy of a blood vessel or perivascular area. Having 2 of these 4 criteria is 88% sensitive and 92% specific for a diagnosis of GPA.
Laboratory testing should include serum PR3-ANCA (c [cytoplasmic]-ANCA), which is positive in nearly all cases of active, severe disease, but less telling in cases of localized disease. A recent study by Janisiewicz and colleagues showed that higher c-ANCA titers are also associated with increased rheumatologic and otolaryngologic visits, suggesting more severe disease. Although the constellation of symptoms and laboratory results may point to the diagnosis, tissue biopsy, usually of the skin, kidney, or lungs, demonstrating granulomatous inflammation is preferable. Nasal mucosal biopsies are another potential option, though diagnostic yield is lower than biopsies from other sites.
Sinonasal involvement in GPA is virtually universal (>90%), and typically manifests as nasal crusting, nasal obstruction, epistaxis, and septal perforation. Progression of disease results in further granulomatous tissue inflammation, and cartilage destruction leading to saddle nose deformity (20%) is possible. CT imaging of the paranasal sinuses may demonstrate mucosal thickening, septal destruction, osteitis, mucocele formation, neo-osteogenesis, and bone destruction ( Fig. 3 ).

Patients with GPA are initially treated with a combination of corticosteroids and methotrexate (mild disease, limited renal involvement) or cyclophosphamide (moderate to severe disease). Prognosis is generally related to the extent of renal involvement, with survival improving over the last several decades, likely owing to more effective medical therapies. For sinonasal manifestations, local therapies such as nasal irrigations, topical corticosteroids, and antibiotics for infections are used. Once again, surgery may be considered for those patients with severe symptoms, especially those caused by anatomic or infectious factors.
Primary Ciliary Dyskinesia
PCD is a class of inherited disorders involving dysmotility (and sometimes, immotility) of cilia. Motile cilia are hairlike organelles protruding from the cell surface that play a role in transporting mucus and liquids over an epithelial surface through a “beating” motion. The most common mode of inheritance for PCD is autosomal recessive, although a multitude of genes may be affected. Of these, the most common genetic mutation found in PCD patients is that coding for the motor protein dynein. Kartagener syndrome is a subtype of PCD characterized by the triad of CRS, bronchiectasis, and situs inversus.
The direct rhinologic impact of poor ciliary motion is impaired mucociliary clearance, which predisposes patients to formation of thick, inspissated sinonasal secretions that are unable to be properly cleared from the sinuses. In addition, patients may also present with a history of recurrent bronchopulmonary and ear infections. In a retrospective review of 84 children diagnosed with PCD, the most common signs and symptoms were chronic suppurative cough (81%), CRS (71%), neonatal respiratory distress (57%), and recurrent otitis media (49%). Once a diagnosis of PCD is made, consultation with genetics and pulmonology specialists should be sought to initiate appropriate counseling and provide long-term follow-up for monitoring pulmonary function, respectively. Because many patients with PCD are diagnosed in childhood, close collaboration with general and specialist pediatricians is equally critical in the care of PCD patients.
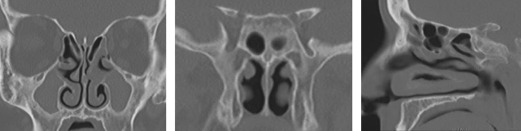
Traditionally, screening of PCD was conducted using the saccharin test, which assesses mucociliary clearance; however, the test is imprecise and thus no longer recommended as a diagnostic tool. More recently, there has been evidence that nasal nitric oxide levels are decreased in PCD patients, and measurement of nitric oxide levels through sampling nasal air has thus supplanted the saccharin test for PCD screening. To confirm the diagnosis, electron microscopy must be performed on nasal brush biopsies to evaluate ciliary structure. Ciliary beat frequency and pattern can further be examined to assess motility. CT imaging typically demonstrates pansinusitis, even after therapy ( Fig. 4 ).
Owing to the rarity of the disease, there is no consensus statement for the management of sinonasal disease in patients with PCD, although treatment strategies are similar to that for CF-related sinonasal disease (ie, promotion of gravitational drainage). A systematic review by Mener and colleagues found that management of sinonasal disease in children with PCD was highly variable and without adequate outcomes assessment. Medical therapies, including nasal irrigations, topical corticosteroid therapy, and systemic antibiotics for acute infections, are helpful in controlling mucosal inflammation and promoting mucociliary clearance. ESS is recommended for patients who fail to improve with medical therapy, or when patients develop recurrent pulmonary infections from a rhinologic source. Tympanostomy with pressure equalization tubes placement is indicated for recurrent middle ear infections.
Odontogenic sinusitis
The floor of the maxillary sinus is in close proximity to the tooth roots of the maxillary molars (teeth #1–3 and #14–16) and, at its most anterior extent, may even be intimately associated with the premolars (teeth #4, #5, #12, and #13). As such, periodontal disease or traumatic disruption of these tooth roots may erode the floor of the maxillary sinus, penetrate the periosteum and mucosa, and lead to maxillary sinusitis. The vast majority of cases (>75%) are unilateral, although a unilateral source leading to sinusitis beyond the maxillary sinus or the contralateral sinus is possible. The microbiology of such infections is quite distinct from that found in nonodontogenic sinusitis, and tends to be composed of a polymicrobial mix of anaerobes (eg, Peptostreptococcus , Fusobacterium ). In a metaanalysis of 770 odontogenic sinusitis cases, the molars are most commonly involved (91%), with overall rare involvement by the premolars (8%) and canines (1%). In the same study, the most common cause was iatrogenic (eg, root canal, dental implants, sinus lift; Fig. 5 ) accounting for 56% of cases, followed by periodontic infections (40%) and odontogenic cysts (7%; Fig. 6 ). Other dentoalveolar conditions such as osteonecrosis of the jaw (ie, bisphosphonate-related ) and malignancy, however rare, should also be considered in cases of isolated maxillary sinusitis ( Fig. 7 ).
Odontogenic sinusitis should be suspected in any patient with unilateral sinusitis with a recent history of dental procedures, especially those involving the upper teeth, or those patients with a longstanding history of dental problems. According to a retrospective review by Pokorny and Tataryn, the most common presenting symptoms of odontogenic sinusitis are facial pain (88%), postnasal discharge (64%), nasal congestion (45%), toothache (39%), and foul drainage (15%). CT imaging of the paranasal sinuses typically reveals unilateral maxillary sinusitis, and careful inspection of the maxillary sinus floor for bone loss (ie, oroantral fistula), dehiscence, or foreign bodies should be performed. Matsumoto and colleagues reviewed 190 CT scans of patients with unilateral sinus opacification and found that more than 70% were attributed to odontogenic infection. Another radiographic study by Bomeli and colleagues found that the extent of maxillary sinus opacification was directly correlated with a concurrent dental source, with 79% of maxillary sinuses that are more than two-thirds opacified caused by an odontogenic infection.
Because odontogenic sinusitis provides a direct entry point for oral flora, it generally cannot be treated adequately with medical or sinonasal surgery alone. Dental extraction, management of periodontal disease, or surgical repair of the oroantral fistula must be performed to resolve the infection. If foreign materials or cystic lesions are implicated in worsening the infection, maxillary antrostomy may be performed to gain access for retrieval and marsupialization, respectively. For revision cases or those requiring wide or anterior access, an endoscopic medial maxillectomy (mega-antrostomy) may be performed. Alternatively, a Caldwell-Luc approach may be undertaken, and has the advantage of direct access to the anterior wall of the maxillary sinus. Underdiagnosis and failure to recognize an odontogenic source of sinonasal infection are common, with many accounts in the literature of radiologists failing to mention odontogenic pathologies, and, as such, odontogenic sinusitis is associated with a higher rate of revision surgery.
Felisati and colleagues presented a prospective series of 257 patients with odontogenic sinusitis, with recommendations for therapy based on the exact cause of the odontogenic infection. They developed and followed an algorithm based on the cause, with an impressive 98.8% of patients deemed successfully treated. Their targeted treatment recommendations are as follows :
- •
The maxillary sinus should be surgically addressed with ESS or a Caldwell-Luc approach in all cases.
- •
Patients with infection after implant or foreign material placement should have the material removed.
- •
Patients with oroantral communication should undergo surgical repair, such as with local flaps.
With appropriate treatment, disease resolution rates are high, with a low risk of recurrence. There seems to be no difference in the timing of whether odontogenic or sinonasal treatments are undertaken, as long as both disease processes are addressed. Many studies demonstrating improvement with therapy have significant follow-up times (>2 years). Furthermore, because the microbiology is fundamentally different, odontogenic sinusitis requires a different antimicrobial treatment strategy. In the senior author’s practice, broad coverage of polymicrobial, anaerobe-predominant organism populations are desired, with penicillins containing a beta-lactamase inhibitor (eg, amoxicillin/clavulanate) or clindamycin, and metronidazole combination therapy fulfilling both of those criteria.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


