Mortality of head and neck cancer has declined in the United States over the past 20 years. This improvement has been linked to use of multimodality treatment of advanced disease. Despite this improvement, disease-specific survival remains low. Patients who survive head and neck cancer are exposed to morbidity and mortality secondary to the same factors as the general population. Factors related to cancer and cancer treatment predispose them to increased risk of mortality. Improvements in head and neck cancer treatment have led to a scenario where an increasing proportion of patients die from causes other than the primary cancer, called competing mortalities.
Key points
- •
The mortality from head and neck squamous cell cancer has declined over the past 30 years.
- •
There are many competing risk factors that contribute to death in cancer patients.
- •
Competing risk factors include the effects of age, gender, race, comorbidities, diet, quality of life (QOL), human papillomavirus (HPV) infection, and second primaries.
- •
The presence of these competing risk factors affect the survival outcome of patients with head and neck cancer.
- •
Traditional survival analysis using Kaplan-Meier statistics may not be appropriate in patients with multiple competing risk factors and may overestimate disease-specific survival (DSS) figures.
- •
Statistical models, which include competing risk factors in the survival analysis model, need to be developed.
- •
These statistical models should be incorporated into the design and analysis of future randomized controlled trials (RCTs) in head and neck cancer management.
Mortality of head and neck cancer has declined in the United States over the past 20 years. This improvement has been linked to the use of multimodality treatment of advanced disease. Despite this improvement, DSS remains low.
Patients who survive head and neck cancer are exposed to morbidity and mortality secondary to the same factors as the general population. It is also clear, however, that factors related to their cancer and cancer treatment predispose them to increased risk of mortality.
Improvements in head and neck cancer treatment, even among patients with advanced disease, have led to a scenario where an increasing proportion of patients die from causes other than the primary cancer. These other causes of death are called competing mortalities. The quantification of overall mortality (OM) may not be an adequate representation of the benefits of treatment. Instead, it may merely be a reflection of the baseline host factors (age, gender, comorbidity status, and so forth) of the patients receiving active treatment and/or the result of the emergence of treatment-related factors and new malignancies.
During the past 20 years, there have been important advances not only in head and neck cancer treatment but also in the way that survival and the factors that affect it are understood, especially the competing causes of death. Examples of such competing risks for mortality are listed in Box 1 . The most important competing risks are death due to patient comorbidities, treatment-related complications, and death secondary to second malignancies. These conditions have been analyzed before in other types of cancers and are receiving greater attention in head and neck cancer.
Age
Gender
Race
Marital (partner) status
Comorbidities
Behavior lifestyles
BMI
QOL
Second primaries
HPV infection
The existence of competing mortalities may preclude the observation of the event of interest, generating negative results instead of improvements in survival. Competing mortalities are especially important in the context where survival is prolonged due to the use of better treatments; if they are present, getting positive will be more unlikely, generating bias toward the null hypothesis. This review analyzes these factors, how they affect survival, and how they can be integrated into survival analysis.
Traditional competing mortalities in head and neck cancer
Effect of Age
Long life expectancy has resulted in more elderly patients with cancer. It has been reported that by 2030, 70% of all cancers will be diagnosed in older adults. This will result in a major public health problem in the future. Elderly patients are likely to have serious comorbidities that can affect treatment decisions. Not all elderly patients will have serious coexistent disease, however, and some elders are healthy people. Unfortunately, older patients are often undertreated because of their age and not because of the presence of chronic diseases. This has been reported before and seems especially true in head and neck cancer patients.
In head and neck cancer patients, increasing age has been associated with poor survival. When severe comorbidities are not present, however, age is not necessarily an independent predictor of poor survival. In a matched-pair analysis, Pytynia and colleagues have shown there was no difference in OS, DSS, or recurrence-free survival (RFS) rates between patients younger than 40 years and older than 40 years when adjusted by comorbidity status.
Age does not necessarily mean poor outcome. There is no evidence that advanced age alone is a contraindication for radical surgery. There are reports that surgery can be safely performed in older head and neck cancer patients. This is also true for advanced reconstructive surgery; there is no evidence that there is a significant increased incidence of flap lost or mortality in the elderly. Multiple reports have shown that radiotherapy alone is effective and well tolerated among older patients in good health condition. In patients treated with chemoradiotherapy, however, age has been associated with reduced chemotherapy compliance. Unfortunately, an increased incidence of noncancer death has been reported in older patients submitted to chemoradiation regimes, probably secondary to acute and late toxicities. Adequate evaluation, effective management of toxicities, and tailored treatment regimes should help reduce this problem.
In a population-based analysis of RCTs undertaken by Mell and colleagues, competing mortality risk was significantly associated with increasing age and increasing comorbidity in a multivariable model. Older patients with comorbidities were more likely to die of noncancer causes. The investigators suggested that these patients should receive a tailored treatment based on their high risk and that they should be excluded from high-risk therapies evaluated in RCT.
Older patients are at risk of receiving substandard treatment based on a doctor’s bias related to age. In addition, families or patients themselves may refuse standard treatment just because of age. This decision is usually based on QOL concerns. There is prospective evidence, however, that QOL in patients treated for head and neck cancer does not differ significantly 1 year after treatment between patients older than 70 and patients younger than 60.
The effect of age on overall survival (OS) is probably clouded because of the presence of comorbidities. Although it has been reported that older patients have a lower OS, this could be a consequence of comorbidities or substandard treatment. Bhattacharyya, in a analysis of 2508 patients with larynx, tongue, and tonsil cancer extracted from the Surveillance Epidemiology and End Results (SEER) database, have shown that when survival was adjusted by cancer-related factors and standard treatment, no significant difference was found between patients older and younger than 70. Substandard treatment is a significant poor prognostic factor in older patients. Therefore, head and neck cancer treatment in elderly patients should be based on comprehensive assessment of preexistent medical conditions and patient choice, not just on chronologic age. How elderly patients can be appropriately included in RCT to test new therapies, avoiding the bias related to age, is a question to be resolved.
Effect of Gender, Partner Status, and Sociocultural Factors
Female gender has been identified as a competing risk of mortality in a recent analysis of predictors of OS. Information about the effect of gender on survival and prognosis is contradictory. Previous reports by the RTOG in head and neck cancer suggested a worse survival in men, especially if they were single. Some population-based studies have also suggested a poorer survival time in men. A more recent analysis by the RTOG on the impact of partner status reported that the presence of a partner improves outcomes: partnered women and men have a better OS than unpartnered women and men. The same analysis showed the protective effect of female gender, partnered and unpartnered, on survival and locoregional control.
Differences in prognosis between genders have also been linked to the presence of HPV. HPV infection seems to be more frequent among men than women (10.1% vs 3.6%). Saba and colleagues, in a SEER database analysis from 1977 to 2006, reported a higher incidence of oropharyngeal cancer among men, likely related to the higher incidence of HPV infection among them. They failed to find a difference in survival between men and women in the whole period. In a similar SEER analysis, however, Brown and colleagues compared survival differences between gender and race between 1977–1991 and 1992–2006. In this analysis, they found better survival rates among white women compared with white and black men in the first period but an improved survival among white men over the other groups in the second period.
In other head and neck cancer sites outside of the oropharynx, the effect of gender on survival is more difficult to assess. A recent matched-pair analysis of patients, with tumors from different localizations in the head and neck, treated in a single institution with the same multidisciplinary approach failed to show any difference in OS, RFS, and DSS after stratification by gender and adjusted by other variables.
The poor prognosis in single men in some of the previous reports cited could have different explanations. This could be due to a lack of partner and family support, emotional problems, or lack of medical insurance, which are more common among single men. Also, gender and marital status have been related to other protective factors, such as high educational level and high socioeconomic status (SES). Lower educational level and lower SES have been shown to be important detrimental prognostic factors in head and neck oncology. Chen and colleagues have reported less mortality for patients with oral cavity and pharyngeal cancer among patients with at least 12 years of education. Similar results have been found in groups of patients treated in RTOG protocols, with significantly better OS and locoregional control in patients with college or technical education. Poor overall health and lack of support systems probably explains most of the differences in survival among these groups.
Gender differences on survival could be related to social-cultural rather than biologic factors. Theses aspects and the emergent influence of gender differences in HPV infection need further investigation and could be important objectives of public health policies.
Effect of Race
The incidence of head and neck cancer in the African American population is greater than that in the white population in the United States. In addition, outcomes are also poorer in African American patients with head and neck cancer. These differences are independent of comorbidities, clinical characteristics, and treatment modality. It has been suggested that outcome differences between patients of different races are related to social factors rather than biologic differences. These social factors include SES, educational level, lower income, lack of health insurance, and late diagnosis.
It has also been suggested that there are differences in the distribution of sites affected and the stage at diagnosis between different races. For example, in oral cavity cancer, it has been reported that black patients are more likely to present with advanced disease, even when socioeconomic and insurance status are adjusted for. Larynx cancer is more frequent among black patients than white, although it is not necessarily diagnosed at a more-advanced stage. Advanced oropharyngeal cancer also occurs more frequently in black patients than white patients. These differences have been linked to preference in tobacco use among black people, with more use of mentholated cigarettes. In addition, African Americans are less likely to stop smoking than whites.
Although the incidence and stage are higher in black patients, this does not necessarily mean that black patients have poorer outcome. Arbes and colleagues and Ragin and colleagues analyzed 2 series of oral cancer patients and failed to show a decrease in OS among African American patients compared with white patients when other demographic characteristics were adjusted for. Chen and colleagues, in a matched-pair analysis, showed no significant differences between cases and controls in RFS, DSS, or OS among black patients and white patients. Bach and colleagues, in a multisite meta-analysis, were not able to find a difference in survival among races in head and neck cancer. In contrast, however, some investigators have noticed differences in DSS, with poor DSS in black patients. In general, it is thought that the differences in survival among races are due to demographic factors rather than biologic factors.
An exception to this concept may be in HPV-related head and neck cancer. Settle and colleagues, in a retrospective and prospective analysis of head and neck cancer patients treated in a single institution, showed that the decrease in OS among African American patients was explained mainly by a worse OS of oropharynx cancer patients. HPV-positive white patients were 9-fold more frequent than HPV-positive black patients in that analysis. Other recent analyses have shown poorer survival rates for African American patients compared with white patients in tonsil and base of tongue cancers. HPV would have a major role in this survival difference. These findings raise the question about the importance of some racial factors in HPV infection and how this could affect prognosis, especially in oropharynx carcinoma. Further analyses of biologic factors that could explain these differences are needed.
Effect of Comorbidities and Lifestyle Behavior
Comorbidities become more common with increasing age and reduce life expectancy. The prevalence of comorbidities among head and neck cancer patients is high ( Table 1 ). The most frequent are cardiovascular (30%–40%) and respiratory (10%–13%) and are almost 2-fold more frequent than in the general population. The proportion of head and neck cancer patients with moderate to severe comorbidities has been reported to be approximately 21% and is just exceeded by the incidence among lung cancer and colorectal cancer patients, 40% and 25%, respectively.
| Author | Country | Patients (N) | Site | Index Used | Comorbidity Prevalence (%) | Prevalence of Moderate/Severe Comorbidity (%) |
|---|---|---|---|---|---|---|
| Singh et al, 1998 | US | 70 | Head and neck (<45 yo) | ACE 27 | — | 30 |
| de Cassia Braga Ribeiro et al, 2003 | Brazil | 110 | Oral cavity | CI | 53.6 | 8.2 |
| Paleri et al, 2003 | UK | 182 | Larynx | ACE 27 | 64.5 | 55.1 |
| Ribeiro et al, 2000 | US | 530 | Oral cavity, oropharynx | CI | 39.1 | — |
| Piccirillo et al, 2004 | US | 1086 | ACE 27 | ACE 27 | 53.9 | 24.1 |
| Borggreven et al, 2005 | Netherlands | 100 | Head and neck | ACE 27 | 83 | 57 |
| Alho et al, 2007 | Finland | 221 | Head and neck | CI | 48.4 | 48.4 |
| Castro et al, 2007 | Brazil | 90 | Larynx | ACE 27 | 88.9 | 16.7 |
| CI | 65.6 | 18.9 | ||||
| Sanabria et al, 2007 | Brazil | 310 | Head and neck (>70 yo) | ACE 27 | 75 | 29.4 |
| Datema et al, 2010 | Netherlands | 1282 | Head and neck | ACE 27 | 36.4 | 19 |
Comorbidities affect treatment decision making and prognosis. For patients with head and neck cancer, the prognostic effect of comorbidities have been widely studied and demonstrated.
Comorbidity assessment
There are different instruments to assess the comorbidity status of cancer patients. Most of these instruments are adapted from other chronic conditions and some of them have been specifically designed for head and neck cancer patients ( Table 2 ). The most commonly used are the Kaplan-Feinstein, adult comorbidity evaluation (ACE) 27, Charlson index, and Washington University Head and Neck Comorbidity Index (WUHNCI). These instruments capture comorbidity information in a retrospective or prospective way. This information can be used for survival prediction, QOL evaluation, or functional outcome.
| Index Name | Year | Developed For | Number of System Evaluated | Number of Comorbidity Ailment | Severity Scale of | Also Includes |
|---|---|---|---|---|---|---|
| Kaplan-Feinstein index | 1974 | General medical (diabetes mellitus) | 6 | 12 | Grade 0 to 3 | Malignancies Alcoholism Psychocomotor impairment |
| Charlson index | 1986 | Breast cancer | 9 | 19 | Severity weighted by 1–6 score. Grade from 0 to 3 according to the sum of weights. | Malignancies AIDS |
| ACE 27 | 2000 | Head and neck cancer | 8 | 27 | Grades 1 to 3. Score is defined according to the highest ranked single ailment | Alcohol abuse Illicit drugs Body weight |
| Washington University Head and Neck Comorbidity Index | 2003 | Head and neck cancer | 4 | 7 | Severity weighted by 1–4 scale. Score from 0 to 15 according to the sum of weights | Malignancies |
Effect of comorbidities on the prognosis of head and neck cancer patients
Patients with severe comorbidities and older age are less likely to undergo aggressive treatments (discussed previously). Patients with comorbidities are more likely to receive palliative therapy rather than curative treatment. It has been recommended that older patients without comorbidities be treated the same as younger patients but with close geriatric observation and more-supportive treatment.
The effect of comorbidities on the prognosis of head and neck cancer patients has been widely reported as an independent predictor on outcome ( Table 3 ). This risk of death, estimated by Piccirillo and colleagues for patients with moderate to severe comorbidities, was 2 to 3 times more compared with patients without comorbidities, adjusting for other patient and tumor characteristics. Reid and colleagues, in a large series of patients from the SEER and Medicare databases, reported an increased relative hazard for patients with Charlson index scores 1 and 2 or more, of 1.3 and 1.8, respectively. This seems extremely important in short-term mortality (less than 6 month). In a review by Datema and colleagues of the Netherlands cancer registries, 5.8% of patients treated died in the first 6 months, and this mortality rate was mainly explained by chronic comorbidities. In 2 analyses of patients with larynx cancer, it has been reported that the 5-year OS for patients with comorbidities was 15% compared with the 5-year OS of 54% to 74% for patients without comorbidities. In oral cavity cancer, similar reports have shown a 10% 5-year survival among patients with severe comorbidities versus 49% in patients without comorbidities. In oropharynx cancer, the same phenomena has been observed, with prognosis reported as 18% versus 40% for patients with and without comorbidities, respectively.
| Authors | Patients Number | Index Used | HR (95% CI) for Overall Survival |
|---|---|---|---|
| Reid et al, 2001 | 9386 | CI | Score 1: 1.33 (1.21–1.47) Score ≥2: 1.83 (1.64–2.05) |
| Piccirillo et al, 2004 | 1086 | ACE 27 | Moderate: 1.92 (1.50–2.48) Severe: 2.48 (1.77–3.47) |
| Datema et al, 2010 | 1282 | ACE 27 | Moderate 1.38 Severe 2.23 |
Alcohol and tobacco use effect on head and neck cancer
The burden of disease in head and neck cancer patients is highly determined by lifestyles; approximately 25% of head and neck cancer patients could be classified as alcoholic (using the Michigan Alcoholism Screening Test protocol) and more than 80% of patients as ever-smokers. The effect of tobacco and alcohol use on OS in these patients has been previously reported. Hall and colleagues estimated 18% of deaths were not related to cancer but were related to other diseases associated with tobacco use after a matched-pair analysis with healthy controls. Duffy has shown that smoking status was the strongest predictor of poor OS, with a hazard ratio of 2 for former smokers and 2.4 for current smokers. Among alcohol users, after controlling for smoking, there is an increased risk of death that has been estimated as 2-fold for patients with alcoholism and 2.76-fold for patients with systemic alcohol-related disease compared with nonalcohol users. Patients with severe alcoholism are at high risk of dying from cardiovascular disease, pulmonary disease, and other alcohol-related conditions.
The effect of alcohol and smoking is also associated with local and regional control of head and neck cancer. In an analysis by Fortin and colleagues, the local control rate among a series of head and neck cancer patients treated with radiotherapy was significantly better for never-smokers than for active smokers (5-year local control 75% vs 67%) and for never-drinkers than active drinkers. There was no significant effect for tobacco and alcohol with regional and distant failure. Regardless of the effect on locoregional control, the information available about the effect of tobacco or alcohol use on DSS is less clear and contradictory and is mainly based on small studies.
Complications with comorbidities
Patients with severe comorbidities also have a higher incidence of complications and mortality secondary to cancer treatment. The most frequent complications are cardiovascular (12%) and respiratory (11%). Complications tend to be more severe in patients with high-risk diseases, even among younger patients.
After treatment of head and neck cancer, the incidence of new comorbidities remains high for the first 6 to 12 months. After this time, the incidence of cardiovascular disease and diabetes returns to overall population rates but not for chronic respiratory disease, anemia, or depression. This is probably a multifactorial phenomenon influenced by the short-term and long-term effects of treatment and the burden of alcohol and tobacco use in most of these patients. On a separate issue, the risk of other malignant diseases remains elevated among these patients after 12 months of treatment, especially in the groups of patients treated with chemotherapy (discussed later).
Effect of Body Mass Index and Diet
A low body mass index (BMI) has been associated with increased risk of head and neck cancer, especially among drinkers and smokers. Rather than being an independent risk factor, however, low BMI is more likely a marker of poor chronic nutritional status secondary to tobacco and alcohol use. Malnutrition and weight loss have been associated with poor prognosis in head and neck cancer, but this seems a consequence of tobacco/alcohol use or an effect of cancer and cancer-treatment rather than an independent predictor. A better BMI could potentially improve treatment results from oncologic as well as QOL perspectives. For example, patients with BMI greater than 25 who undergo chemoradiation therapy are shown to have better swallowing function.
Two large population studies have found different results. Mell and colleagues reported that lower BMI is an independent risk factor of treatment-related mortality in a competing risk analysis. A similar finding appeared when recurrence and second malignancies were analyzed, showing a high incidence of lower BMI among patients with cancer-related events. Gaudet and colleagues, in a large prospective analysis, reported that smoking patients with BMI greater than 24.9 have a 28% higher risk of dying of head and neck cancer than smoking patients with BMI greater than 25. This result was not observed, however, among nonsmokers.
Despite these observations, when OS has been measured, low BMI has not been independently associated with poor survival in the few cases studies that have addressed this question.
Other pretreatment healthy behaviors have been reported to influence survival. High intakes of poultry, vegetables, and vitamin C were observed to improve survival in head and neck cancer patients. These protective effects were not observed among patients with high intake of animal proteins or high fat intake. A prospective analysis carried out by Sandoval and colleagues suggested that high intake of vegetables before and after diagnosis of oral cancer may reduce the risk of recurrence, overall mortality, and cancer mortality in oral cancer patients. The number of patients is small, however, and failed to show significance in a multivariate analysis. In a recent analysis by Duffy and colleagues, fruit and vegetable intake failed to predict survival in head and neck cancer patients after adjustment for tobacco and alcohol use or tumor characteristics.
The effect of dietary factors has also been analyzed with respect to the incidence of new primaries of the upper aerodigestive tract. It has been suggested that some dietary factors (like low citrus fruit intake) could contribute with alcohol and smoking to increase the risk of second primary cancers among patients with head and neck cancers.
Effect of Quality of Life
Health-related QOL has been increasingly measured in head and neck cancer patients in the context of prospective trials. The scales used to measure QOL give important information about the impact of disease and treatment on patients. It also allows analyzing any association between QOL and survival outcomes. In a recent review of the literature, published between 1982 and 2008, Montazeri reported that 4 of the 8 studies analyzing the association between QOL and survival of head and neck cancer patients failed to demonstrate any survival effect. It has been proposed that there is not a strong relationship between QOL and survival. Some specific factors, however, could be influencing long-term survival, such as poor satisfaction, eating/speech problems, and presence of pain 1 year after treatment. These factors could potentially help detect patients at high risk of poor survival.
Effect of Second Primary Malignancies
Head and neck cancer patients have a high risk of morbidity and mortality because of second primary malignancies. This is a problem for patients with early stage head and neck cancer because these patients often survive for a long time. Second primaries are also important for survivors of aggressive multimodality therapy for advanced disease. Second primary tumors of the upper aerodigestive tract are common among head and neck patients due to the chronic DNA damage within the squamous epithelium from carcinogenic exposure. The carcinogenic effect of tobacco and alcohol is multistep and synergistic. It also predisposes patients to multiple precancerous and cancerous lesions in the aerodigestive tract, upper esophagus, and lungs. Consequently, some types of secondary tumors are more frequent than in the general population and are a source of mortality that competes with the primary index tumor. Second primary tumors are the most important cause of death among head and neck cancer survivors.
The actuarial rate of second primary tumors of the aerodigestive tract has been reported to be between 9% and 14%. Leon and colleagues established that the annual incidence of second cancers among head and neck cancer patients is 3.8%. This increases to 5.1% in patients with a third tumor and to 7.8% in patients with a fourth tumor. The head and neck is the most common site of second malignancies (30%–50%), followed by the lung (34%). Most of these cancers are squamous cell carcinomas (86%). Haughey and colleagues, in a meta-analysis of second cancers, described a prevalence of 14.2% in 40,287 patients with head and neck cancer. Most of the second cancers are metachronous, as was described by Liao et al. The site with highest prevalence of second cancers is the oral cavity, and approximately 50% of aerodigestive tract second primaries were detected by 2 years from index tumor presentation. They are not uncommon, however, even after 5 years. For this reason, lifetime follow-up is recommended, with close endoscopic surveillance recommended during the first 2 years after the index tumor.
Previous reports have shown that second malignancies are generally detected earlier or at least in a less-advanced stage than the index cancer, probably due to more-intense surveillance. Despite this, patients with second malignancies have a lesser survival than patients with primary malignancies.
Survival with second primaries or successive tumors
Second primaries or successive tumors have been reported to adversely affect the survival of head and neck cancer patients. Leon and colleagues described a 10% decrease in 5-year OS with each new second malignancy, regardless if they were treated or not. The effect on survival of the second primary is influenced by the location of the new tumor. Second primary cancers arising in the esophagus and lungs are significantly associated with a poorer prognosis than second primary tumors arising in the head and neck region. It has been hypothesized that this poor prognosis could be secondary to the effect of previous treatment (eg, radiotherapy) or more-aggressive biologic behavior.
Jones described some factors that were more common among patients with second primary tumors:
- •
Younger age (second primary tumors more likely in men younger than 60 years)
- •
Laryngeal and oral cavity index tumor sites
- •
Small primary tumors
- •
Absence of neck metastases at the time of index tumor diagnosis
Lin and colleagues reported that tobacco and alcohol use was associated with a 5-fold and 2-fold increased risk of second primary tumors, respectively. Radiotherapy to the index tumor was not associated with an increased risk of developing a second tumor. Patients with a second primary can be treated successfully with surgery or nonsurgical treatment. Patients treated aggressively have a better survival than patients without treatment. The proportion of patients who are considered candidates for radical surgery decreases, however, with successive primaries.
The effect of previous radiotherapy on survival after a new primary is unclear. Dolan and colleagues, in a series of 358 patients with second primaries, reported that metachronous cancers are significantly associated with poor survival when the cancer arises within previously irradiated tissue. Other investigators have reported, however, no significant differences for previously irradiated patients.
Site of second primary tumors
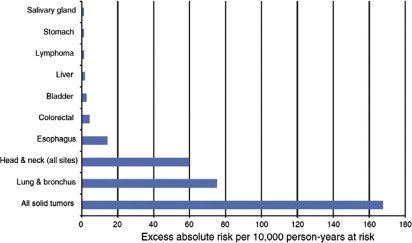
The increasing risk of second primaries is not restricted to the aerodigestive tract. Morris and colleagues, in a recent analysis of the SEER database, described an incidence of 22.6% of second primary malignancies if all other sites are included (colorectal, bladder, kidney, skin, and cervix). They estimated the incidence of observed to expect ratio of second primary cancer is 2.2 compared with the general population. Most of the excess is explained by second primaries arising in the upper aerodigestive tract, followed by colorectal cancer and bladder, both of which are linked to tobacco use ( Fig. 1 ). The risk of other common cancers, such as breast and prostate cancer, was not elevated over the general population.
Morris and colleagues have demonstrated the risk of second primary malignancies differs significantly by the subsite of index head and neck cancer. The higher observed-to-expected second-cancer ratio was for hypopharynx (3.5×), followed by oropharynx (3.0×), oral cavity (2.8×) and larynx (1.9×). Hypopharynx and larynx are most commonly associated with second primaries in the lung. Oropharynx and oral cavity are most commonly associated with second primaries in the head and neck. Morris and colleagues described a significant decrease in the incidence of second primaries among patients with oropharyngeal cancer in the past 10 years. This phenomenon could be linked to the etiologic shift in oropharyngeal carcinoma from a tobacco and alcohol–related cancer to an HPV-related carcinoma. Further analyses are needed, but there are some reports suggesting a decreased risk of second primaries among HPV-positive oropharyngeal carcinoma. An increasing incidence of anogenital cancer after an oral cavity/pharyngeal cancer, and vice versa, has been reported linking sexual behavior in the development of this disease.
Mortality risk factors with second primaries
In an analysis of how second primaries act as competing risk factors for mortality, Rose and colleagues identified increasing age, African American race, unmarried status, higher SES, advantage stage, nonsurgical treatment, and hypopharyngeal/oral cavity sites as independent risk factors of death among patients with second primaries.
The lack of effective preventative measures of second primary malignancies in survivors of head and neck cancer emphasizes the importance of tobacco and alcohol cessation among these patients and also the increasing importance of safe sexual behavior practice.
Traditional competing mortalities in head and neck cancer
Effect of Age
Long life expectancy has resulted in more elderly patients with cancer. It has been reported that by 2030, 70% of all cancers will be diagnosed in older adults. This will result in a major public health problem in the future. Elderly patients are likely to have serious comorbidities that can affect treatment decisions. Not all elderly patients will have serious coexistent disease, however, and some elders are healthy people. Unfortunately, older patients are often undertreated because of their age and not because of the presence of chronic diseases. This has been reported before and seems especially true in head and neck cancer patients.
In head and neck cancer patients, increasing age has been associated with poor survival. When severe comorbidities are not present, however, age is not necessarily an independent predictor of poor survival. In a matched-pair analysis, Pytynia and colleagues have shown there was no difference in OS, DSS, or recurrence-free survival (RFS) rates between patients younger than 40 years and older than 40 years when adjusted by comorbidity status.
Age does not necessarily mean poor outcome. There is no evidence that advanced age alone is a contraindication for radical surgery. There are reports that surgery can be safely performed in older head and neck cancer patients. This is also true for advanced reconstructive surgery; there is no evidence that there is a significant increased incidence of flap lost or mortality in the elderly. Multiple reports have shown that radiotherapy alone is effective and well tolerated among older patients in good health condition. In patients treated with chemoradiotherapy, however, age has been associated with reduced chemotherapy compliance. Unfortunately, an increased incidence of noncancer death has been reported in older patients submitted to chemoradiation regimes, probably secondary to acute and late toxicities. Adequate evaluation, effective management of toxicities, and tailored treatment regimes should help reduce this problem.
In a population-based analysis of RCTs undertaken by Mell and colleagues, competing mortality risk was significantly associated with increasing age and increasing comorbidity in a multivariable model. Older patients with comorbidities were more likely to die of noncancer causes. The investigators suggested that these patients should receive a tailored treatment based on their high risk and that they should be excluded from high-risk therapies evaluated in RCT.
Older patients are at risk of receiving substandard treatment based on a doctor’s bias related to age. In addition, families or patients themselves may refuse standard treatment just because of age. This decision is usually based on QOL concerns. There is prospective evidence, however, that QOL in patients treated for head and neck cancer does not differ significantly 1 year after treatment between patients older than 70 and patients younger than 60.
The effect of age on overall survival (OS) is probably clouded because of the presence of comorbidities. Although it has been reported that older patients have a lower OS, this could be a consequence of comorbidities or substandard treatment. Bhattacharyya, in a analysis of 2508 patients with larynx, tongue, and tonsil cancer extracted from the Surveillance Epidemiology and End Results (SEER) database, have shown that when survival was adjusted by cancer-related factors and standard treatment, no significant difference was found between patients older and younger than 70. Substandard treatment is a significant poor prognostic factor in older patients. Therefore, head and neck cancer treatment in elderly patients should be based on comprehensive assessment of preexistent medical conditions and patient choice, not just on chronologic age. How elderly patients can be appropriately included in RCT to test new therapies, avoiding the bias related to age, is a question to be resolved.
Effect of Gender, Partner Status, and Sociocultural Factors
Female gender has been identified as a competing risk of mortality in a recent analysis of predictors of OS. Information about the effect of gender on survival and prognosis is contradictory. Previous reports by the RTOG in head and neck cancer suggested a worse survival in men, especially if they were single. Some population-based studies have also suggested a poorer survival time in men. A more recent analysis by the RTOG on the impact of partner status reported that the presence of a partner improves outcomes: partnered women and men have a better OS than unpartnered women and men. The same analysis showed the protective effect of female gender, partnered and unpartnered, on survival and locoregional control.
Differences in prognosis between genders have also been linked to the presence of HPV. HPV infection seems to be more frequent among men than women (10.1% vs 3.6%). Saba and colleagues, in a SEER database analysis from 1977 to 2006, reported a higher incidence of oropharyngeal cancer among men, likely related to the higher incidence of HPV infection among them. They failed to find a difference in survival between men and women in the whole period. In a similar SEER analysis, however, Brown and colleagues compared survival differences between gender and race between 1977–1991 and 1992–2006. In this analysis, they found better survival rates among white women compared with white and black men in the first period but an improved survival among white men over the other groups in the second period.
In other head and neck cancer sites outside of the oropharynx, the effect of gender on survival is more difficult to assess. A recent matched-pair analysis of patients, with tumors from different localizations in the head and neck, treated in a single institution with the same multidisciplinary approach failed to show any difference in OS, RFS, and DSS after stratification by gender and adjusted by other variables.
The poor prognosis in single men in some of the previous reports cited could have different explanations. This could be due to a lack of partner and family support, emotional problems, or lack of medical insurance, which are more common among single men. Also, gender and marital status have been related to other protective factors, such as high educational level and high socioeconomic status (SES). Lower educational level and lower SES have been shown to be important detrimental prognostic factors in head and neck oncology. Chen and colleagues have reported less mortality for patients with oral cavity and pharyngeal cancer among patients with at least 12 years of education. Similar results have been found in groups of patients treated in RTOG protocols, with significantly better OS and locoregional control in patients with college or technical education. Poor overall health and lack of support systems probably explains most of the differences in survival among these groups.
Gender differences on survival could be related to social-cultural rather than biologic factors. Theses aspects and the emergent influence of gender differences in HPV infection need further investigation and could be important objectives of public health policies.
Effect of Race
The incidence of head and neck cancer in the African American population is greater than that in the white population in the United States. In addition, outcomes are also poorer in African American patients with head and neck cancer. These differences are independent of comorbidities, clinical characteristics, and treatment modality. It has been suggested that outcome differences between patients of different races are related to social factors rather than biologic differences. These social factors include SES, educational level, lower income, lack of health insurance, and late diagnosis.
It has also been suggested that there are differences in the distribution of sites affected and the stage at diagnosis between different races. For example, in oral cavity cancer, it has been reported that black patients are more likely to present with advanced disease, even when socioeconomic and insurance status are adjusted for. Larynx cancer is more frequent among black patients than white, although it is not necessarily diagnosed at a more-advanced stage. Advanced oropharyngeal cancer also occurs more frequently in black patients than white patients. These differences have been linked to preference in tobacco use among black people, with more use of mentholated cigarettes. In addition, African Americans are less likely to stop smoking than whites.
Although the incidence and stage are higher in black patients, this does not necessarily mean that black patients have poorer outcome. Arbes and colleagues and Ragin and colleagues analyzed 2 series of oral cancer patients and failed to show a decrease in OS among African American patients compared with white patients when other demographic characteristics were adjusted for. Chen and colleagues, in a matched-pair analysis, showed no significant differences between cases and controls in RFS, DSS, or OS among black patients and white patients. Bach and colleagues, in a multisite meta-analysis, were not able to find a difference in survival among races in head and neck cancer. In contrast, however, some investigators have noticed differences in DSS, with poor DSS in black patients. In general, it is thought that the differences in survival among races are due to demographic factors rather than biologic factors.
An exception to this concept may be in HPV-related head and neck cancer. Settle and colleagues, in a retrospective and prospective analysis of head and neck cancer patients treated in a single institution, showed that the decrease in OS among African American patients was explained mainly by a worse OS of oropharynx cancer patients. HPV-positive white patients were 9-fold more frequent than HPV-positive black patients in that analysis. Other recent analyses have shown poorer survival rates for African American patients compared with white patients in tonsil and base of tongue cancers. HPV would have a major role in this survival difference. These findings raise the question about the importance of some racial factors in HPV infection and how this could affect prognosis, especially in oropharynx carcinoma. Further analyses of biologic factors that could explain these differences are needed.
Effect of Comorbidities and Lifestyle Behavior
Comorbidities become more common with increasing age and reduce life expectancy. The prevalence of comorbidities among head and neck cancer patients is high ( Table 1 ). The most frequent are cardiovascular (30%–40%) and respiratory (10%–13%) and are almost 2-fold more frequent than in the general population. The proportion of head and neck cancer patients with moderate to severe comorbidities has been reported to be approximately 21% and is just exceeded by the incidence among lung cancer and colorectal cancer patients, 40% and 25%, respectively.
| Author | Country | Patients (N) | Site | Index Used | Comorbidity Prevalence (%) | Prevalence of Moderate/Severe Comorbidity (%) |
|---|---|---|---|---|---|---|
| Singh et al, 1998 | US | 70 | Head and neck (<45 yo) | ACE 27 | — | 30 |
| de Cassia Braga Ribeiro et al, 2003 | Brazil | 110 | Oral cavity | CI | 53.6 | 8.2 |
| Paleri et al, 2003 | UK | 182 | Larynx | ACE 27 | 64.5 | 55.1 |
| Ribeiro et al, 2000 | US | 530 | Oral cavity, oropharynx | CI | 39.1 | — |
| Piccirillo et al, 2004 | US | 1086 | ACE 27 | ACE 27 | 53.9 | 24.1 |
| Borggreven et al, 2005 | Netherlands | 100 | Head and neck | ACE 27 | 83 | 57 |
| Alho et al, 2007 | Finland | 221 | Head and neck | CI | 48.4 | 48.4 |
| Castro et al, 2007 | Brazil | 90 | Larynx | ACE 27 | 88.9 | 16.7 |
| CI | 65.6 | 18.9 | ||||
| Sanabria et al, 2007 | Brazil | 310 | Head and neck (>70 yo) | ACE 27 | 75 | 29.4 |
| Datema et al, 2010 | Netherlands | 1282 | Head and neck | ACE 27 | 36.4 | 19 |
Comorbidities affect treatment decision making and prognosis. For patients with head and neck cancer, the prognostic effect of comorbidities have been widely studied and demonstrated.
Comorbidity assessment
There are different instruments to assess the comorbidity status of cancer patients. Most of these instruments are adapted from other chronic conditions and some of them have been specifically designed for head and neck cancer patients ( Table 2 ). The most commonly used are the Kaplan-Feinstein, adult comorbidity evaluation (ACE) 27, Charlson index, and Washington University Head and Neck Comorbidity Index (WUHNCI). These instruments capture comorbidity information in a retrospective or prospective way. This information can be used for survival prediction, QOL evaluation, or functional outcome.
| Index Name | Year | Developed For | Number of System Evaluated | Number of Comorbidity Ailment | Severity Scale of | Also Includes |
|---|---|---|---|---|---|---|
| Kaplan-Feinstein index | 1974 | General medical (diabetes mellitus) | 6 | 12 | Grade 0 to 3 | Malignancies Alcoholism Psychocomotor impairment |
| Charlson index | 1986 | Breast cancer | 9 | 19 | Severity weighted by 1–6 score. Grade from 0 to 3 according to the sum of weights. | Malignancies AIDS |
| ACE 27 | 2000 | Head and neck cancer | 8 | 27 | Grades 1 to 3. Score is defined according to the highest ranked single ailment | Alcohol abuse Illicit drugs Body weight |
| Washington University Head and Neck Comorbidity Index | 2003 | Head and neck cancer | 4 | 7 | Severity weighted by 1–4 scale. Score from 0 to 15 according to the sum of weights | Malignancies |
Effect of comorbidities on the prognosis of head and neck cancer patients
Patients with severe comorbidities and older age are less likely to undergo aggressive treatments (discussed previously). Patients with comorbidities are more likely to receive palliative therapy rather than curative treatment. It has been recommended that older patients without comorbidities be treated the same as younger patients but with close geriatric observation and more-supportive treatment.
The effect of comorbidities on the prognosis of head and neck cancer patients has been widely reported as an independent predictor on outcome ( Table 3 ). This risk of death, estimated by Piccirillo and colleagues for patients with moderate to severe comorbidities, was 2 to 3 times more compared with patients without comorbidities, adjusting for other patient and tumor characteristics. Reid and colleagues, in a large series of patients from the SEER and Medicare databases, reported an increased relative hazard for patients with Charlson index scores 1 and 2 or more, of 1.3 and 1.8, respectively. This seems extremely important in short-term mortality (less than 6 month). In a review by Datema and colleagues of the Netherlands cancer registries, 5.8% of patients treated died in the first 6 months, and this mortality rate was mainly explained by chronic comorbidities. In 2 analyses of patients with larynx cancer, it has been reported that the 5-year OS for patients with comorbidities was 15% compared with the 5-year OS of 54% to 74% for patients without comorbidities. In oral cavity cancer, similar reports have shown a 10% 5-year survival among patients with severe comorbidities versus 49% in patients without comorbidities. In oropharynx cancer, the same phenomena has been observed, with prognosis reported as 18% versus 40% for patients with and without comorbidities, respectively.



