Surgical Management of Suprachoroidal Hemorrhage
Chirag C. Patel
Naresh Mandava
Hugo Quiroz-Mercado
INTRODUCTION
Suprachoroidal hemorrhage (SCH) is the accumulation of blood in the suprachoroidal space (Fig. 59-1). This can occur in the perioperative period as a complication of ophthalmic surgery or occur as a result of trauma. A distinction should be made between choroidal detachment and SCH. A choroidal detachment refers to an accumulation of serous fluid within the suprachoroidal space. This is often the result of inflammation or hypotony. In a SCH, the fluid in the suprachoroidal space is by definition blood. In addition to etiology, the extent of SCH can vary. A small collection of blood in the suprachoroidal space is usually benign and may resolve on its own. In contrast, a large SCH may grow to a sufficient size to cause the inner retinal surfaces to touch; these have been described as appositional or “kissing” choroidals (Fig. 59-2). Larger SCHs are much less likely to resolve on their own and have a worse prognosis. Additionally, if associated with an open wound during surgery or trauma, a large SCH may force intraocular contents out of the eye. This is called an expulsive SCH and has a poor prognosis. Since there can be a wide range of presentations of SCH, many factors must be taken into consideration to determine the appropriate management for such patients.
ANATOMY AND PATHOPHYSIOLOGY
The choroid is a highly vascular structure that lies between the retina and the sclera. It has maximal thickness posteriorly where it is 0.22 mm thick. It progressively thins anteriorly to 0.1 mm at the ora seratta (1). The short posterior ciliary arteries supply blood to the choroid. It is composed of three layers, the outermost Haller’s layer, the middle Sattler’s layer, and innermost choriocapillaris. These blood vessels have the highest rate of blood flow on the basis of volume per weight in the body and hold approximately 70% of the blood volume in the eye at any one time (2). The Haller’s layer is composed of relatively large caliber vessels. This layer merges with the intermediate caliber Sattler’s layer. These two layers are composed of nonfenestrated vessels that help to distribute blood entering through the short posterior ciliary arteries over the extent of the choroid. The innermost choriocapillaris lies adjacent to Bruch’s membrane. This layer is made up of fenestrated capillaries that allow passage of erythrocytes and nutrients to the retina and retinal pigment epithelium. After travelling through the choriocapillaris, blood collects in the venules that drain into the vortex veins. Each eye has four to five vortex veins that leave the eye near the equator.
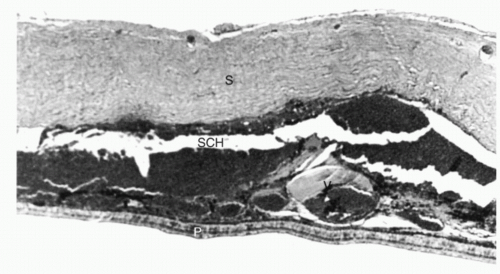 Figure 59-1. Suprachoroidal hemorrhage (SCH) between the retina (R) and sclera (S). |
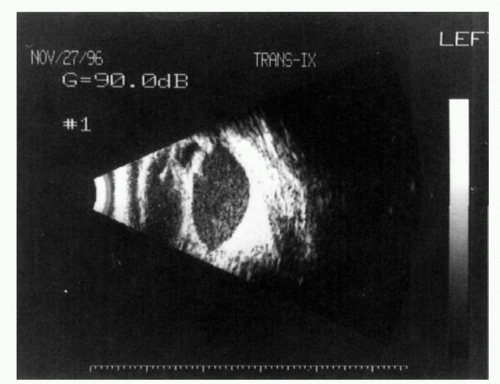 Figure 59-2. Appositional or “kissing” choroidal hemorrhage. A large amount of blood in the suprachoroidal space has caused retinal surfaces to touch. |
Posteriorly, the choroid is firmly attached to the optic nerve head; the vortex veins anchor the choroid to the sclera at the equator, and anteriorly the choroid is continuous with the ciliary body. The choroid weakly adheres to the sclera elsewhere. Consequently, choroidal detachments have a lobular appearance between these attachment points. The suprachoroidal space normally holds 10 cc of fluid (3); however, a SCH can cause this space to expand far beyond this volume to accumulate a large amount of blood. During a SCH, the space anterior to the equator usually expands first, followed by more posterior areas; this is a consequence of the choroid being more adherent to the sclera posteriorly (4).
Choroidal pressure is equivalent to intraocular pressure (IOP). IOP is an important factor in the development of SCH because adequate pressure is required to keep the choroid opposed to the sclera and the suprachoroidal space closed. In nontraumatized eyes, hypotony appears to be the major precipitating factor causing a SCH to develop (5). It is thought that hypotony can cause rupture of a ciliary artery resulting in hemorrhage. This rupture may be the result of ciliary artery necrosis (6). Additionally, an initial choroidal effusion may stretch a ciliary artery resulting in rupture (7). With trauma, a SCH can develop from direct injury to ciliary arteries, vortex veins, large choroidal vessels, or ciliary body. Hypotony inflicted from a penetrating or perforating injury can also cause a SCH in a similar fashion to that described above.
CLINICAL CONSIDERATIONS
SCH is a relatively rare event in the absence of trauma. It can occur during or after any type of ocular surgery. In a review of the literature, incidence of SCH is lowest after cataract phacoemulsification with intraocular lens implantation. A study reviewing 23,213 such surgeries found an incidence of SCH of 0.03% (8). Glaucoma surgery has the highest incidence of SCH, with rates as high as 6.1% having been reported (9). Rates during vitreoretinal surgery have been reported between 0.17% (10) to 1.9% (11). Unlike corneal or glaucoma surgery, prolonged intraocular hypotony usually does not occur during vitreoretinal surgery. However, development of SCH may be related to damage caused to the choroid during subretinal drainage procedures or during the creation of pars plana sclerotomies, or owing to compression of vortex veins during placement of scleral buckling elements (12).
Other risk factors for development of SCH include phakic or aphakic status, history of chronic glaucoma, severe myopia, and presence of SCH in the other eye. Sudden decompression of the globe during surgery can also predispose to SCH; it is therefore important to aggressively manage high IOP prior to ocular surgery (13). Systemic risk factors include intraoperative hypertension and tachycardia. Both can predispose the patient to intraoperative bleeding. General anesthesia is also thought to be a risk factor for SCH. SCH can occur if the patient coughs or “bucks” on the endotracheal tube during the procedure (14). Valsalva maneuvers postoperatively that can occur from vomiting or constipation can also cause SCH. Consequently, antiemetics and laxatives should be used in high-risk patients.



