Purpose
To report change in strabismus-specific health-related quality of life (HRQOL) following treatment with prism.
Design
Retrospective cross-sectional study.
Methods
Thirty-four patients with diplopia (median age 63, range 14-84 years) completed the Adult Strabismus-20 questionnaire (100-0, best to worst HRQOL) and a diplopia questionnaire in a clinical practice before prism and in prism correction. Before prism, diplopia was “sometimes” or worse for reading and/or straight-ahead distance. Prism treatment success was defined as diplopia rated “never” or “rarely” on the diplopia questionnaire for reading and straight-ahead distance. Failure was defined as worsening or no change in diplopia. For both successes and failures, mean Adult Strabismus-20 scores were compared before prism and in prism correction. Each of the 4 Adult Strabismus-20 domains (self-perception, interactions, reading function, and general function) was analyzed separately.
Results
Twenty-three of 34 (68%) were successes and 11 (32%) were failures. For successes, reading function improved from 57 ± 27 (SD) before prism to 69 ± 27 in-prism correction (difference 12 ± 20, 95% CI 3.2-20.8, P = .02) and general function improved from 66 ± 25 to 80 ± 18 (difference 14 ± 22, 95% CI 5.0-23.6, P = .003). Self-perception and interaction domains remained unchanged ( P > .2). For failures there was no significant change in Adult Strabismus-20 score on any domain ( P > .4).
Conclusions
Successful correction of diplopia with prism is associated with improvement in strabismus-specific HRQOL, specifically reading function and general function.
Strabismus associated with diplopia significantly impacts an individual’s health-related quality of life (HRQOL). Previous studies have shown that successful surgical correction of strabismus is often associated with significant improvement in both function and psychosocial HRQOL concerns, but there are few studies evaluating the effects of nonsurgical treatments for strabismus on the patient’s HRQOL. Prism correction is a commonly used nonsurgical treatment for binocular diplopia in the context of a variety of different strabismus types. Successful correction of diplopia using prism would be expected to result in significant improvements in visual function, which may then translate into improved HRQOL. The aim of this study was to assess whether successful treatment of diplopia with prism was associated with improved HRQOL.
Subjects and Methods
This study is a retrospective cross-sectional study of patients with diplopia treated with prism attending a clinical practice. Approval was obtained prior to the commencement of the study from the Institutional Review Board, Mayo Clinic, Rochester, Minnesota, and all procedures and data collection were conducted in a manner compliant with the Health Insurance Portability and Accountability Act (HIPAA). Verbal consent and written HIPAA authorization were obtained for each patient.
Subjects
Consecutive strabismus patients undergoing prism correction of diplopia (using either Fresnel or incorporated prism) in a clinical practice were retrospectively reviewed. Eligible patients were those prescribed prism who had also completed the Adult Strabismus-20 questionnaire and the diplopia questionnaire at both their preprism examination and their follow-up examination when wearing prism correction. Both the Adult Strabismus-20 and the diplopia questionnaire were administered routinely to all patients with diplopia, at each examination, from March 2010. Unwillingness or refusal to complete the questionnaires was extremely rare, minimizing patient selection bias. Patients prescribed prism for blur, asthenopia, or eye strain who did not also report symptoms of diplopia on the diplopia questionnaire were not eligible for inclusion; neither were patients who were already wearing a prism correction. Response to prism treatment was assessed at a follow-up examination at least 3 weeks after prism correction was prescribed.
Methods
Diplopia Questionnaire
The diplopia questionnaire (freely available at www.pedig.net , accessed February 3, 2014) was completed by each patient as part of his or her clinical examination, typically while the patient was in the waiting area and before any clinical testing commenced. The diplopia questionnaire allows the patient to rate the severity of his or her diplopia in each of 7 gaze positions (reading, straight-ahead distance, right gaze, left gaze, up gaze, down gaze, and any other gaze position) on a 5-point scale (never, rarely, sometimes, often, always).
For inclusion in the present study of responsiveness to prism correction, diplopia prior to prescribing prism was required to be at least moderately severe, defined as the patient rating diplopia frequency as either “sometimes” or worse for reading and/or for straight-ahead distance on the diplopia questionnaire. This requirement allowed room for improvement, defined as reduction in diplopia frequency to “rarely” or “never.”
Adult Strabismus-20 Questionnaire
The Adult Strabismus-20 is a patient-derived, strabismus-specific HRQOL questionnaire for adults with strabismus. Patients typically completed the Adult Strabismus-20 in the waiting area before the commencement of any clinical testing. In previous Rasch analysis of the Adult Strabismus-20, 4 distinct domains were identified: self-perception (5 items), interactions (5 items), reading function (4 items), and general function (4 items) (full questionnaire freely available at www.pedig.net , accessed February 3, 2014). Each of the 4 domains is scored independently using Rasch scoring methods and converted to a 0-100 score (worst to best HRQOL) for easier interpretation (scoring spreadsheet freely available at www.pedig.net , accessed February 3, 2014).
Analysis
Prism Success and Failure
Prism treatment success was defined as diplopia while wearing prism, rated as “never” or “rarely” for both reading and straight-ahead distance. Prism treatment failure was defined as worsening or no change in diplopia for reading and/or straight-ahead distance.
Adult Strabismus-20 Scores
Mean Adult Strabismus-20 scores (0-100, worst to best HRQOL) were calculated, both before prism correction and when wearing prism correction, for each of the 4 Adult Strabismus-20 domains (self-perception, interactions, reading function, and general function) in each patient. Before-prism data were taken from the visit at which prism was first prescribed. In-prism data were taken from the next examination, regardless of whether prism strength was subsequently changed or not.
Adult Strabismus-20 scores before prism correction and when wearing prism were compared overall, and in subgroups of successes and failures, using signed rank tests. In addition, Adult Strabismus-20 scores before prism correction and in prism were compared between Fresnel prism and ground-in prism for successes and failures using Wilcoxon tests.
To evaluate for potential baseline differences between patients who ended up as successes and those who ended up as failures, several factors were compared between groups. Mean Adult Strabismus-20 scores and mean diplopia questionnaire scores before prism were compared between successes and failures using Wilcoxon tests. Median prism strength prescribed was also compared between successes and failures using Wilcoxon tests. In addition, the proportion of patients with incomitant deviations was compared between groups using Fisher exact tests: incomitance was defined as a difference between primary position and up, down, right, or left gaze of 10 prism diopters (PD) or more for horizontal deviation or 5 PD or more for vertical deviation.
Results
Thirty-four patients (median age 63, range 14-84 years) were included. Twenty-four (71%) were female, and for 33 (97%) race was reported as white. Strabismus types were idiopathic (11/34, 32%), childhood onset (7/34, 21%), mechanical (7/34, 21%), and neurogenic (9/34, 26%). Twenty-four of 34 patients (71%) had undergone previous strabismus surgery, 9 (38%) having had surgery within the previous 3 months, but only 3 of these were prescribed prism owing to worse diplopia following surgery. No patient was prescribed prism for postoperative diplopia when there had been no diplopia preoperatively. Overall the mean magnitude of prism prescribed was 8 PD, ranging from 1 PD to 25 PD. Twenty-three of 34 patients (68%) were prescribed Fresnel prism and 11 (32%) were prescribed ground-in prism. Follow-up examinations in prism correction were a mean of 4.5 months (range 3 weeks to 18 months) following the preprism examination.
Indications for prism correction were either long-term management of diplopia associated with small-angle (defined as 10 PD or less) strabismus (n = 19, 56%), temporary correction of diplopia prior to strabismus surgery (n = 9, 26%), long-term management of diplopia in patients for whom strabismus surgery was presently inadvisable (eg, evolving Graves disease, resolving sixth cranial nerve palsy) (n = 5, 15%), and near-distance disparity, where different prisms were needed for near and distance fixation (n = 1, 3%).
Based on a priori definitions of success and failure using responses on the diplopia questionnaire, 23 of 34 patients (68%) were classified as prism successes and 11 (32%) were classified as prism failures.
Adult Strabismus-20 Scores Before Prism: All Patients
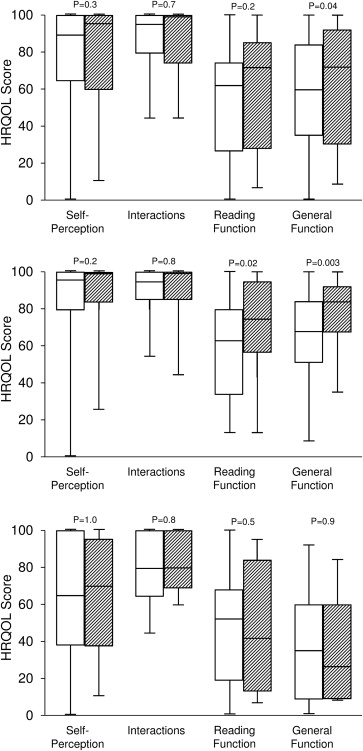
Overall mean Adult Strabismus-20 scores before prism were 57 ± 29 (SD) for the general function domain, 54 ± 28 for the reading function domain, 79 ± 26 for the self-perception domain, and 87 ± 16 for interactions ( Figure , Top).
Adult Strabismus-20 Scores in Prism: All Patients
Across all patients, mean Adult Strabismus-20 scores when wearing prism were significantly improved for the general function domain compared with scores before prism correction, improving from 57 ± 29 to 66 ± 29 (mean difference 9 ± 27, 95% CI −0.1 to 19.0; P = .04, Figure , Top). For the reading function, self-perception, and interaction domains, there were no significant changes in scores from before prism correction to wearing prism ( P > .1 for each, Figure , Top).
Adult Strabismus-20 Scores in Prism: Successes
For the 23 patients successfully treated with prism, mean Adult Strabismus-20 scores significantly improved when wearing prism for the general function and reading function domains. For general function, scores improved from 66 ± 25 before prism correction to 80 ± 18 in prism correction (mean difference 14 ± 22, 95% CI 5.0-23.6, P = .003, Figure , Middle). For the reading function domain, scores improved from 57 ± 27 before prism correction to 69 ± 27 in prism correction (mean difference 12 ± 20, 95% CI 3.2-20.8; P = .02, Figure , Middle). For self-perception and interaction domains, there was no difference between HRQOL scores before prism correction and when wearing prism correction ( P > .2 for each, Figure , Middle).
Adult Strabismus-20 Scores in Prism: Failures
For the 11 patients for whom prism treatment was unsuccessful, there were no significant differences between Adult Strabismus-20 scores before prism correction and Adult Strabismus-20 scores when wearing prism correction, for each of the 4 Adult Strabismus-20 domains ( P > .4 for each, Figure , Bottom).
Fresnel Versus Ground-in Prism
Of the 23 patients successfully treated with prism, 17 (74%) were treated with Fresnel prism and 6 (26%) with ground-in prism. Of the 11 patients who failed prism treatment, 6 (55%) were treated with Fresnel prism and 5 (45%) with ground-in prism. For successfully treated patients, Adult Strabismus-20 scores improved on the reading function domain both for patients wearing Fresnel prism (mean 58 ± 26 to 71 ± 25; mean difference 13 ± 23, 95% CI 0.8-24.9; P = .05) and for patients wearing ground-in prism (mean 55 ± 33 to 64 ± 36; difference 10 ± 7, 95% CI 1.9-17.2; P = .06). For the general function domain, scores improved for patients treated with Fresnel prism (mean 61 ± 26 to 80 ± 18; difference 19 ± 22, 95% CI 7.9-30.9; P = .002) but did not significantly improve for patients wearing ground-in prism (mean 80 ± 14 to 80 ± 20; difference −1 ± 10, 95% CI −10.7 to 10.7; P = .999). For the self-perception and interactions domains, there were no improvements in scores for patients treated with Fresnel prism ( P > .3 for each) or ground-in prism ( P > .6 for each). For failures, on the general function domain, scores numerically improved for patients wearing Fresnel (20 ± 19 to 44 ± 22; difference 24 ± 23, 95% CI −0.3 to 48.2, P = .1) and reduced for patients wearing ground-in prism (mean 59 ± 25 to 29 ± 32; difference −30 ± 23, 95% CI −58.6 to −2.2, P = .06); however, differences were not statistically significant. There were no differences in Adult Strabismus-20 scores for Fresnel prism or ground-in prism on any of the other 3 Adult Strabismus-20 domains ( P > .06 for all).
Baseline Differences Between Successes and Failures
Adult Strabismus-20 Scores Before Prism
For the general function domain of the Adult Strabismus-20, scores before prism correction were significantly higher (better) for the 23 successes than for the 11 failures (66 ± 25 vs 38 ± 29; P = .01). For the other 3 Adult Strabismus-20 domains, scores before prism correction were not significantly different between successes and failures ( P > .08 for each).
Diplopia Scores Before Prism
Comparing baseline diplopia questionnaire scores between successes and failures, there was no significant difference between scores for the 23 prism successes (mean diplopia score 58 ± 24) and scores for the 11 prism failures (mean diplopia score 58 ± 28, P = .999).
Magnitude of Prism Prescribed
The magnitude of prism prescribed was similar for successes (6 PD, range 1-25 PD) and failures (10 PD, range 2-20 PD; P = .3).
Incomitant Strabismus
Overall, 25 of 34 patients (74%) were classified as having comitant strabismus and 9 (26%) as incomitant strabismus. There was no significant difference in the proportion of patients with incomitant deviations in those successfully treated with prism compared with those for whom prism treatment failed: of the 23 successes, 6 (26%) had incomitant deviations and of the 11 failures, 3 (27%) had incomitant deviations ( P = .999).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


