Submacular Hemorrhage
Rishi P. Singh
Hilel Lewis
INTRODUCTION
Submacular hemorrhage is a common consequence of choroidal neovascularization (CNV) in patients with age-related macular degeneration (AMD) (Figure 52-1A, 52-1B). It also can be seen secondary to retinal arterial macroaneurysm, trauma, retinopathy resulting from Valsalva’s maneuver and leukemia, and CNV from other causes including presumed ocular histoplasmosis syndrome and high myopia. Observational studies on the natural history of submacular hemorrhage show variable results depending on the underlying cause. Patients with submacular hemorrhage from AMD may develop severe loss of vision, especially if the center of the fovea is involved (1, 2, 3 and 4). However, submacular hemorrhage from trauma or macroaneurysm may resolve with much less damage to the photoreceptors and retinal pigment epithelium (RPE) (1).
Traditionally, these patients were observed, because precise localization of choroidal neovascular membranes for laser treatment or photodynamic therapy was not possible and other treatment modalities were not available. Recent advances in both submacular surgical techniques and intravitreal antivascular endothelial growth factor agents (anti-VEGF) have increased interest in surgical treatment of such patients. Clinical and histopathologic studies published to date do support recommendations regarding surgery and specific interventions for submacular hemorrhage. Although some patients with submacular hemorrhage may benefit from surgical evacuation, the ideal characteristics for good surgical outcomes have not been studied in a randomized large multicenter trial. General guidelines for management can be formulated through our current understandings of histopathological studies and small case series of eyes with submacular hemorrhage.
HISTOLOGY AND PATHOPHYSIOLOGY
How does submacular hemorrhage cause retinal damage? There are a variety of theories that have been formulated based on histological examination of submacular hemorrhage in animal models. It is likely a combination in factors which leads to retinal damage after submacular hemorrhage. First, toxicity may occur resulting from iron released from hemoglobin (5). Second, the blood may act as a barrier, impairing metabolic exchange between the photoreceptors and RPE. Finally, fibrin-mediated mechanical damage to the outer retina may occur because of clot contraction (6,7).
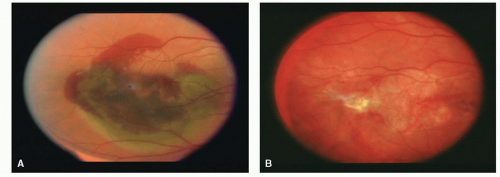 Figure 52-1. A: Preoperative photo demonstrating submacular hemorrhage due to age-related macular degeneration. Visual acuity count fingers at 3 feet. B: Postoperative photo with complete resolution of submacular hemorrhage, localized atrophy, and subretinal fibrosis. Visual acuity is 20/400. |
Glatt and Machemer (5) demonstrated irreversible damage to the photoreceptors within 24 hours after introduction of subretinal blood in a rabbit model and outer retinal degeneration within 3 to 7 days. Toth et al. (7) looked at the early events associated with subretinal hemorrhage in a cat model. The most striking finding in their study was the rapid formation of a fibrin clot interdigitating between the photoreceptor outer segments. This was seen within the first hour of introduction of subretinal hemorrhage. Mechanical shearing of the photoreceptors resulting from traction of fibrin strands followed. The most severe retinal degeneration occurred over the ensuing 3 to 14 days and was found over the areas of dense fibrin coagulum, as opposed to the areas of dense erythrocytes. The authors proposed that fibrin and perhaps other inflammatory products are responsible for the retinal damage rather than iron toxicity or the presence of erythrocytes as a barrier to diffusion. If tissue plasminogen activator (t-PA), a clotspecific fibrinolytic agent, was injected into the subretinal space along with the blood, mechanical shearing of the photoreceptors was not seen. This confirmed the initial observation by Lewis and coauthors that fibrinolytic therapy may be a useful adjunct to surgical removal of subretinal hemorrhage (6).
Lewis et al. (6) also studied the effect of recombinant t-PA on experimental subretinal hemorrhage in rabbits. Subretinal hemorrhage created by injection of blood alone was compared with simultaneous injection of blood and t-PA or blood and balanced salt solution (BSS). Clearance of subretinal hemorrhage was significantly faster in eyes given t-PA than in those given BSS or blood alone. Additionally, eyes receiving t-PA or BSS sustained less degenerative change in retinal appearance and retained larger numbers of well-organized retinal outer segments than those receiving blood alone. It is
postulated that this beneficial effect of both t-PA and BSS may be caused by dilution of toxic factors released by lysed blood cells, as well as a reduction in metabolic barrier from clot in the subretinal space.
postulated that this beneficial effect of both t-PA and BSS may be caused by dilution of toxic factors released by lysed blood cells, as well as a reduction in metabolic barrier from clot in the subretinal space.
Terasaki et al. (8) evaluated the changes in preoperative versus postoperative focal macular electroretinography in five patients undergoing surgical drainage of submacular hemorrhages. Preoperative electroretinographic response was reduced remarkably or was unrecordable in all eyes. Postoperative electroretinographic responses, recorded between 1 and 4 months after surgery, recovered to about one half of the amplitude of the normal fellow eye. These findings showed that the severe retinal dysfunction associated with submacular hemorrhage can be reversed at least partially with surgical intervention (8).
NATURAL HISTORY
Observational studies in humans have shown a wide variability in the natural course of subretinal hemorrhage (Table 52-1A, 52-1B). The largest series to date reviewed by Scupola et al. (4) examined sixty eyes with submacular hemorrhage due to AMD. In this retrospective series, vision deteriorated in 80% of patients with a mean initial acuity of 20/240 and a mean final acuity of 20/1250 at 24 months follow-up. Worse visual outcome was correlated with larger initial hemorrhage size and greater initial retinal thickness. The natural dissolution of hemorrhage varied from 2 to 18 months and recurrent bleeding occurred in 38% of eyes. At the end of the study, 25% had atrophic scars, 38% had subretinal fibrosis, and 22% had RPE tears (4).
Bennett et al. (1) highlighted the variable outcome of submacular hemorrhage from causes other than AMD. In this study, 29 patients with subretinal hemorrhages greater than one disc diameter involving the center of the fovea were included. The cause of hemorrhages in this study included (listed in descending order of frequency) choroidal neovascular membranes associated with AMD, ruptured retinal arterial macroaneurysms, traumatic choroidal rupture, choroidal neovascular membranes associated with presumed ocular histoplasmosis syndrome and pseudoxanthoma elasticum, and complications of scleral buckling surgery. Initial visual acuities varied widely, from 20/70 to light perception (average 20/860). Final visual acuities with a mean follow-up of 3 years also varied widely, from 20/30 to light perception (average 20/480). The most important predictor of poor visual outcome was the presence of AMD. The average final visual acuity in patients with AMD was 20/1700, and none of these patients had a final visual acuity better than 20/200. Patients with submacular hemorrhage associated with other causes of choroidal neovascular membranes also had poor outcomes, with the exception of one patient with presumed ocular histoplasmosis syndrome whose visual acuity improved from 20/200 to 20/30. The patients with the best outcomes in this series were those with subretinal hemorrhages from traumatic choroidal rupture. This may be explained partly by the fact that, on average, patients with hemorrhages from choroidal rupture had better initial visual acuity than patients with AMD, and all of the traumatic hemorrhages were classified as thin (1).
TABLE 52-1 COMPARISON OF NATURAL-HISTORY STUDIES AND SURGICAL STUDIES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||



