The nasal cavity has a robust vascular supply, and bleeding is a primary obstacle to the minimally invasive skull base technique. Venous bleeding, including the cavernous sinus, can be managed with various techniques using hemostatic materials and pressure. A thorough understanding of the skull base vascular anatomy is vital for avoiding injury to major arteries and having confidence to control venous bleeding to optimize the endoscopic view and tumor resection.
Key points
- •
A comprehensive preoperative history and review of medications and supplements are important to identify and optimize patients with an increased risk of bleeding.
- •
Intraoperatively, total intravenous anesthesia, controlled hypotension, controlled heart rate, and a reverse Trendelenburg position can reduce blood loss and improve visibility.
- •
Hot saline irrigation improves the surgical view, particularly in cases longer than 2 hours.
- •
Embolization or intraoperative arterial control should be considered preoperatively in vascular tumors.
- •
Cavernous sinus bleeding can be reliably controlled using FloSeal and pressure applied with a cottonoid.
Introduction
Minimally invasive skull base surgery is a technique that provides a panoramic view to the surgeon through a 4-mm telescope. This technique has many advantages over open approaches, including the avoidance of an external scar, shortened hospital stays and recovery time, and improved visualization. However, visualization and operative times can be hindered if hemostasis is not optimized. The nasal cavity has a robust vascular supply, and a primary obstacle to the minimally invasive technique is the prevention of blood from obscuring the endoscope and narrowing the surgical field. The risk of serious complications increases when important landmarks cannot be clearly delineated.
Many of the techniques for improving hemostasis are derived from the endoscopic sinus surgery literature and include preoperative evaluation, anesthetic techniques, and intraoperative considerations. Although hemostasis is the primary method for improving visualization, there are other techniques and advances in technology that have allowed for improved visualization and efficiency.
Introduction
Minimally invasive skull base surgery is a technique that provides a panoramic view to the surgeon through a 4-mm telescope. This technique has many advantages over open approaches, including the avoidance of an external scar, shortened hospital stays and recovery time, and improved visualization. However, visualization and operative times can be hindered if hemostasis is not optimized. The nasal cavity has a robust vascular supply, and a primary obstacle to the minimally invasive technique is the prevention of blood from obscuring the endoscope and narrowing the surgical field. The risk of serious complications increases when important landmarks cannot be clearly delineated.
Many of the techniques for improving hemostasis are derived from the endoscopic sinus surgery literature and include preoperative evaluation, anesthetic techniques, and intraoperative considerations. Although hemostasis is the primary method for improving visualization, there are other techniques and advances in technology that have allowed for improved visualization and efficiency.
Hemostasis
Preoperative Evaluation
A thorough preoperative patient history is paramount in assessing an increased bleeding risk. Questions about epistaxis, gingival bleeding with brushing, excessive bruising, and severe bleeding with trauma or previous surgery help rule out hereditary disorders. Patients should be asked about medications, supplements, and alternative therapies that may affect coagulation. Medical conditions that inhibit platelet function or cause thrombocytopenia should also be elucidated in the history.
The routine use of coagulation studies is not recommended but should be considered in patients with histories of abnormal bleeding. A panel of laboratory tests should be ordered when the history is concerning for a bleeding abnormality and include an activated partial thromboplastin time, prothrombin time, platelet count, fibrinogen, and a von Willebrand panel or thromboelastogram If an abnormality is found, further testing and a hematology evaluation are warranted.
The American Society of Anesthesiologists recommends that patients stop all herbal medications 2 to 3 weeks before surgery. Antiplatelet and anticoagulant medications should be stopped before surgery according to the most recent Chest guidelines. Bridging with heparin or low-molecular-weight heparin is recommended for patients with a strong indication for anticoagulation (patients who have a mechanical heart valve, atrial fibrillation, or venothromboembolism and high risk for thromboembolism). It is recommended to stop warfarin 5 days, low-molecular-weight heparin 24 hours, and heparin 4 to 6 hours before surgery. Aspirin and nonsteroidal antiinflammatory medications should be stopped 7 to 10 days before but may need to be continued perioperatively in high-risk patients. Thienopyridines (clopidogrel) are stopped 10 days and glycoprotein IIb (GpIIb)/GpIIIa antagonists 24 to 72 hours before surgery. Surgery should be deferred for 6 weeks after bare-metal stent placement and 6 months after drug-eluting stent placement instead of undertaking elective surgery within these periods. Cardiologists should be consulted regarding management of anticoagulation in the perioperative period in high-risk patients; require perioperative antiplatelet therapy may be required in urgent situations.
Intraoperative considerations
Anesthetic Techniques
Total intravenous anesthesia (TIVA) with a combination of propofol and remifentanil has been shown to provide a more optimal surgical field compared with inhalation anesthesia. This finding is believed in large part to be related to hemodynamic advantages seen with TIVA compared with inhalation anesthesia. More specifically, TIVA has been associated with lower mean arterial pressures (MAPs), and lower MAP has been shown to affect both blood loss and visibility. MAP and controlled hypotension are discussed in greater detail later. In addition, TIVA has been associated with lower heart rates compared with inhalation anesthesia, and this has been shown to significantly affect surgical field clarity as well.
However, in a study by Wormald and colleagues comparing TIVA with inhalation anesthesia, when MAP and heart rate were both held constant, visibility still remained significantly better in the TIVA group, suggesting an additional variable at play. The investigators of this study hypothesized that this additional variable could potentially be vasodilation caused by the inhalational agents, which is not seen with TIVA. Any special requests regarding anesthesia should of course be discussed with the anesthesia team before the start of the case to ensure that the most appropriate and safest anesthesia is given to the patient based on their overall health status. Any other benefit of 1 form of anesthesia over another is a secondary consideration.
Patient positioning
The positioning of the patient can have an impact on visualization during surgery. Both Ko and colleagues and Hathorn and colleagues randomized patients into groups to compare the reverse Trendelenburg position (RTP) with a reclined or horizontal position. Ko and colleagues found that a 10° RTP and Hathorn and colleagues found that a 15° RTP significantly decreased total blood loss, blood loss per minute, and improved the surgical field but did not decrease the operative time. Gan and colleagues then compared 5°, 10°, and 20° RTP in a double-blind randomized controlled trial of 75 patients undergoing endoscopic sinus surgery. These investigators found a significant improvement in the Boezaart endoscopic field-of-view score and a decrease in blood loss (1.8, 135 mL) when the head position was at 20° compared with 5° (2.0, 231) and 10° (1.8, 230 mL). There was no significant difference in mean arterial blood pressure, blood loss per minute, or operative time among the 3 groups. Controlled hypotension is a technique often used to help reduce blood loss. A goal MAP between 60 and 70 mm Hg is typically recommended. Some studies have shown that an increased MAP significantly affects the surgical field by increasing blood loss. Other studies have failed to support this finding and suggest that MAP less than 70 mm Hg can increase intraoperative bleeding secondary to vasodilation. Neurologic injury secondary to inadequate cerebral blood flow is also a concern. In our experience, visualization is improved when the MAP is safely minimized. The goal MAP is dependent on the patient’s preoperative blood pressure control and medical comorbidities.
Topical and local vasoconstriction
Use of topical and injectable vasoconstrictive agents provides 2 major benefits: decongestion of the nasal mucosa and less bleeding. Decongestion of the mucosa alone improves the visual field. It further provides more space through which to pass instruments and can lead to less traumatization to the tissue and thus less bleeding. Anecdotally, it is believed that injection of vasoconstrictive agents leads to less bleeding and better visualization, but this remains to be proved objectively.
It is our practice to inject 1% lidocaine with 1:100,000 of epinephrine into the anterior and posterior septum, the lateral nasal wall, middle turbinates, and the sphenopalatine foramen (SPF). We specifically avoid injection at the anatomic location of the posterior septal artery in the interest of preserving the vascular pedicle to the nasoseptal flap.
Irrigation
Irrigating with copious amounts of saline washes any fresh or clotted blood from the surgical site and effectively clears the surgical field. Hot saline irrigation (49°C) has been shown to improve visualization in endoscopic sinus surgery for patients with chronic rhinosinusitis when the surgical time was longer than 2 hours. Gan and colleagues also showed a reduced blood loss per minute when irrigating with warm irrigation in longer cases. The mechanism of action is not well understood but is believed to include mucosal and intraluminal edema that narrows and compresses the vessels and thus decreases flow. Hot water irrigation (40–42°C) reduces mucosal bleeding and bleeding from minor intracranial vessels.
Control of arterial bleeding
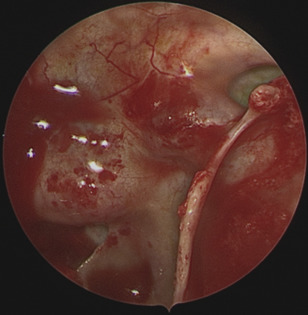
With many minimally invasive skull base approaches, the internal carotid arteries (ICA) and basilar artery are either in the field or millimeters away ( Figs. 1 and 2 ). Injury to the ICA can be devastating and the importance of preparedness for this situation cannot be overstated. The ICA surgical anatomy, mechanisms of injury, management of injury, and outcomes are discussed in greater detail in another section.
Embolization
It is our practice for vascular tumors such as juvenile nasopharyngeal angiofibromas (JNAs), and occasionally meningiomas, to perform preoperative embolization. Studies have shown that embolization performed 24 to 48 hours before surgery can be safely carried out with low risk of neurologic complications. Two techniques for preoperative embolization of vascular tumors are a transarterial approach (TA) versus direct tumor puncture (DTP). The TA method is effective but has several noted disadvantages. Elhammady and colleagues described these disadvantages as being more time consuming because multiple feeding vessels must be catheterized, less complete embolization given, there may be a need and sometimes failure to catheterize these feeding arteries for various reasons (vessel origin angle, diameter of the vessel, tortuosity), and there may be an increased risk of inadvertent embolization into the cerebral circulation. The benefits of DTP were found to be that it is less time consuming and provides better penetration of embolic material into the tumor parenchyma; overall, DTP led to a greater degree of angiographic tumor devascularization.
Various embolic materials exist and are classified into either particulates or liquid embolic material. Particulates tend to have several pitfalls, including coalescence and occlusion of the microcatheter, which then must be exchanged, leading to repeat catheterization of the pedicle and a prolonged operative time. Particulates must also be mixed with contrast dye to be seen on angiography. Particulates also carry a higher risk of inadvertent reflux into the intracranial circulation. Cyanoacrylate and ethylene vinyl alcohol (Onyx, Irvine, CA) are the 2 liquid embolic agents. Overall, the ease of use of Onyx and its properties that allow for more controlled injection with better penetration into the tumor and the ability to pause and restart an injection make it a more popular material than cyanoacrylate. In a study comparing transarterial particulate embolization (TAPE) with direct percutaneous embolization (DPE) with Onyx, the DPE group had significantly less intraoperative blood loss and need for transfusion over the TAPE group, suggesting better clinical outcomes of Onxy over particles.
Endoscopic resection of JNAs has been shown to be appropriate for certain lesions (Andrews stages 1, 2, and some 3a) and has been associated with reduced intraoperative blood loss, shorter hospital stays, and excellent control of disease, with no recurrences after endoscopic resection. Certainly, resection of these tumors can be a challenge given the high volume of blood loss and difficult anatomy of the pterygopalatine or infratemporal fossa. Instituting the techniques discussed within this article along with the 4-handed/2-surgeon technique that has allowed so much success in endoscopic skull base surgery along with careful preoperative planning can provide a more controlled setting and possibly better outcomes.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


