Purpose
To evaluate the change of epithelial and flap thickness after femtosecond laser–assisted in situ keratomileusis (LASIK) using spectral-domain optical coherence tomography (SD OCT) in correlation with the spherical equivalent refraction treated and clinical outcomes.
Design
Prospective, randomized, contralateral-eye study.
Methods
Forty myopic eyes underwent LASIK using an excimer laser with refraction ranging from −1.00 to −7.25 diopters (mean −3.25 ± 1.9). Flap creation was randomized between eyes, using the IntraLASE FS60 laser (IL) in 1 eye and WaveLight FS200 laser (FS) in the contralateral eye. SD OCT was used to evaluate the epithelial and flap thickness profiles and corneal power preoperatively and at 1 week and 1, 3, and 9 months postoperatively. Manifest and wavefront refractions were performed at each postoperative visit.
Results
Statistically significant epithelial thickening was observed in both IL and FS groups as early as 1 month postoperatively ( P = .033 and P = .042), but this stabilized between 3 ( P = .042 and P = .035) and 9 months ( P = .043 and P = .041). Femtosecond-LASIK flaps were thicker in the IL group in comparison to the FS group at 3 and 9 months postoperatively ( P = .003 and P = .005, respectively). There was a statistically significant correlation between the magnitude of preoperative myopic refraction and the central epithelial thickness at 1, 3, and 9 months (Pearson correlation coefficients 0.485, 0.587 and 0.576) ( P = .0021, P = .0010, and P = .0011), respectively. SD OCT corneal power maps showed steepening at 3 and 9 months along with mild myopic shift.
Conclusion
Progressive epithelial and flap thickening with increased corneal power were observed after femtosecond laser-assisted in situ keratomileusis for myopia with consequent stabilization between 3 to 9 months postoperatively. The magnitude of epithelial and flap thickness remodeling correlated to the preoperative myopic refractive error.
The corneal epithelium has been reported to be highly reactive to underlying stromal asymmetries to reduce surface irregularities and to preserve the optical system. Compensatory changes of the corneal epithelium to produce a smooth corneal surface have been described in keratoconus, stromal scars, and corneal dystrophies, and post refractive surgery.
Anterior segment spectral-domain optical coherence tomography (SD OCT) has been found to be more accurate and reproducible than time-domain OCT. In 2 previous studies of SD OCT, high-resolution cross-sectional scanning (with an axial resolution of 5 μm), localized corneal epithelial thickness changes, and greater patterns of thickness deviation were found in eyes with keratoconus and postoperative corneal ectasia in comparison to normal eyes.
Although up until recently, this detailed SD OCT analysis of epithelial thickness has not been previously performed in normal myopic post–laser-assisted in situ keratomileusis (LASIK) eyes, very high-frequency (50 MHz VHF) digital ultrasound mapping (with a resolution of 21 μm) has been previously studied, revealing progressive epithelial thickening in the central 4-mm zone with a surrounding annulus of epithelial thinning.
In this study, we seek to evaluate the epithelial thickness profile changes and flap architecture after myopic LASIK with 2 different femtosecond lasers, using high-resolution SD OCT to correlate the anatomic findings to the preoperative spherical equivalent manifest refraction and refractive outcomes. To the best of our knowledge, this is 1 of only 2 reported studies on epithelial thickness mapping and remodeling after femtosecond LASIK using an anterior segment SD OCT, and the first of flap thickness mapping using this same technology.
Patients and Methods
Forty eyes of 20 patients undergoing femtosecond LASIK for myopia from December 6, 2011 to January 15, 2013 were enrolled in a prospective, randomized, contralateral-eye study approved by the Cleveland Clinic Foundation’s Institutional Review Board. Prepresbyopic, myopic candidates for LASIK refractive surgery were voluntarily included in the study if they were able to complete the required follow-up and had no ocular diseases or previous ocular surgery. Informed consent was obtained from the patients to participate in the research study. All surgeries consistently adhered to the tenets of the Declaration of Helsinki.
Uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), manifest and cycloplegic refraction, corneal topography (Atlas 9000; Carl Zeiss Meditec Inc, Dublin, California, USA), corneal power changes by SD OCT (6 mm Pachymetry + Corneal power software [Cpwr] scans; RTVue-100; Optovue, Fremont, California, USA), and wavefront analysis (LADARWave aberrometer; Alcon Laboratories, Inc, Fort Worth, Texas, USA) were performed preoperatively and 1 week, 1 month, 3 months, and 9 months postoperatively.
Surgical Technique
The femtosecond laser flaps were created with the Wavelight FS200 laser (FS) (Alcon Laboratories) in 1 eye and the IntraLASE FS60 laser (IL) (Abbott Medical Optics, Irvine, California, USA) in the contralateral eye. Randomization of femtosecond laser use was determined by alternating right and left eyes by the day of the week in which the surgery was scheduled (Tuesday: FS OD, IL OS, Thursday: IL OD, FS OS). All flaps were created with a superior hinge, an intended flap thickness of 110 μm, diameter of 8.7 mm, side cut angle of 55 degrees, bed energy of 0.8 μJ, and spot and line separation of 7.0 μm. Both eyes were treated with the Allegretto Wave Eye-Q Excimer Laser System (Alcon Laboratories). All eyes were treated with the wavefront-optimized ablation profile, optical zone of 6.5 mm, and transition zone of 1.5 mm centered on the patient’s pupil. All surgeries were performed by a single surgeon (R.R.K.). Postoperatively, patients received prednisolone acetate 1% and moxifloxacin 0.5% 4 times daily for 1 week, along with artificial tears as needed.
Corneal Epithelial Thickness and Flap Thickness Mapping by Spectral-Domain Optical Coherence Tomography
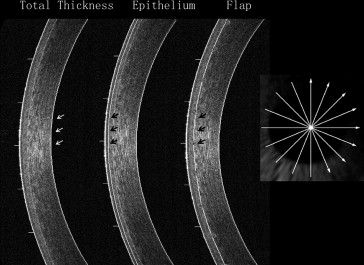
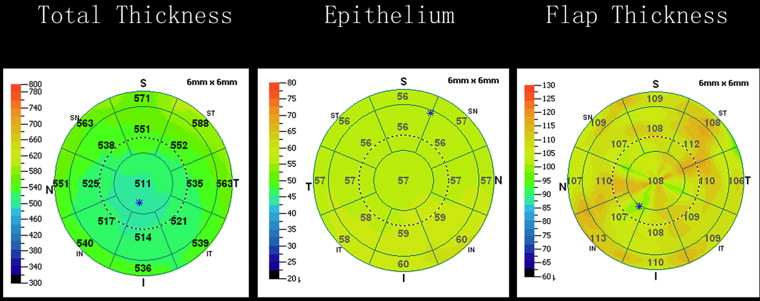
A spectral-domain OCT device (Optovue RTVue-100) with a scan rate of 26 000 axial scans per second, 830 nm wavelength, axial resolution of 5 μm, transverse resolution of 15 μm, and a corneal long adaptor (CAM-L mode: 6.0–2.0 mm) was used to assess the total pachymetry map and epithelial thickness map preoperatively and 1 week, 1 month, 3 months, and 9 months post femtosecond LASIK for myopia. Flap thickness maps were generated at 1 week, 1 month, 3 months, and 9 months postoperatively. The Pachymetry + Cpwr with 1024 axial scans and 6 × 6 mm diameter was used to scan the cornea in 8 meridians centered at the corneal vertex. The high-resolution, cross-sectional scans are repeated 5 times and averaged to generate the pachymetry maps. The air–tear interface and the epithelial–Bowman layer landmark were identified automatically by a computer algorithm to generate the epithelial thickness maps, as described by Li and associates.
The distance between the anterior surface of the cornea and the flap–stroma interface was used as OCT anatomic landmarks. These flap boundaries were manually detected and inspected and 9 points were manually measured in 8 meridians to generate the flap thickness profile maps. The automated algorithm built into the RTVue software was used to interpolate the high-resolution scans. The color scale ranged from 20 to 80 μm for the epithelial thickness maps and from 70 to 140 μm for the flap thickness profile maps. The average thicknesses of the central (2 mm) and superior and inferior zones (2–5 mm) were assessed for epithelial and flap thickness profile maps ( Figures 1 and 2 ).
Data Analysis
Statistical analysis was performed using the JMP 10.0 software (SAS Institute Inc, Cary, North Carolina, USA). Student t test was used to evaluate differences between groups, and 1-way analysis of variance (ANOVA) was used to compare central (2 mm) and peripheral (2–5 mm superiorly and inferiorly) measurements across the cornea. Pearson correlation coefficients were calculated between preoperative manifest refraction spherical equivalent and central epithelial thickness postoperatively. P values <.05 were considered statistically significant.
Results
Forty myopic eyes were enrolled in this study. Table 1 summarizes the preoperative clinical features and postoperative clinical outcomes comprising postoperative changes in manifest refraction (MRSE) and wavefront refraction (WRSE) spherical equivalent, wavefront analysis (spherical aberration and coma – 5.5 mm pupil diameter), and total corneal power measured by SD OCT (6 mm Pachymetry + Cpwr scans) in the IL and FS laser groups. One hundred percent of patients achieved UDVA of 20/20 or better in both groups at 9 months postoperatively. Meanwhile, the MRSE, WRSE, and Cpwr at 1 week and 1 month were the most hyperopic or flat, with a mild myopic shift or steepening at the 3 month time point, which then stabilized by 9 months.
| Groups (n = 40 eyes) | Wavelight FS 200 | IntraLASE FS 60 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| MRSE (D) | WRSE (D) | Cpwr (D) | Spherical Aberration (μm) a | Coma (μm) a | MRSE (D) | WRSE (D) | Cpwr (D) | Spherical Aberration (μm) a | Coma (μm) a | |
| Preoperative | −3.25 ± 1.93 (range −1.125 to −7.25 D) | −3.25 ± 1.97 (range −0.915 to −7.75 D) | 43.19 ± 1.52 (range 40.2 to 46.3 D) | 0.19 ± 0.12 (range 0 to 0.49 μm) | 0.20±0.10 (range 0.01 to 0.43 μm) | −3.24 ± 1.95 (range −1 to −7.125 D) | −3.2 ± 1.99 (range −0.955 to −7.11 D) | 43.32 ± 1.38 (range 40.5 to 45.8 D) | 0.18 ± 0.12 (range 0 to 0.47 μm) | 0.21 ± 0.09 (range 0 to 0.47 μm) |
| 1 week postoperative | 0.14 ± 0.28 (range 1 to 0 D) | −0.08 ± 0.53 (range 0.89 to −0.45 D) | 39.92 ± 2.91 (range 33.3 to 43.7 D) | 0.14 ± 0.12 (range 0.05 to 0.40 μm) | 0.19 ± 0.13 (range 0.02 to 0.54 μm) | −0.03 ± 0.17 (range 0 to −0.5 D) | −0.28 ± 0.42 (range 1.03 to −1.04 D) | 40.11 ± 2.28 (range 35.1 to 43.2 D) | 0.11 ± 0.10 (range 0.01 to 0.39 μm) | 0.19 ± 0.14 (range 0.02 to 0.52 μm) |
| 1 month postoperative | 0.08 ± 0.19 (range 0 to −0.37 D) | −0.03 ± 0.43 (range 0.47 to −0.645 D) | 39.84 ± 2.95 (range 33.1 to 43.3 D) | 0.18 ± 0.21 (range 0.01 to 0.53 μm) | 0.19 ± 0.10 (range 0.02 to 0.46 μm) | 0.05 ± 0.25 (range 0.375 to −0.375 D) | −0.24 ± 0.52 (range 0.63 to −1.45 D) | 40.07 ± 2.32D (range 33.9 to 43.1 D) | 0.12 ± 0.12 (range 0 to 0.42 μm) | 0.18 ± 0.12 (range 0.01 to 0.52 μm) |
| 3 months postoperative | 0.06 ± 0.16 (range 0 to −0.25 D) | −0.25 ± 0.49 (range 0.52 to −0.9 D) | 40.15 ± 2.9 (range 33.8 to 43.4 D) | 0.11 ± 0.11 (range 0 to 0.34 μm) | 0.20 ± 0.11 (range 0 to 0.46 μm) | −0.05 ± 0.16 (range 0 to −0.25 D) | −0.38 ± 0.51 (range 0.42 to −1.23 D) | 40.37 ± 2.36 (range 34.1 to 43.7 D) | 0.11 ± 0.10 (range 0 to 0.33 μm) | 0.18 ± 0.12 (range 0 to 0.48 μm) |
| 9 months postoperative | 0.02 ± 0.08 (range 0 to −0.25 D) | −0.26 ± 0.5 (range 0.46 to −0.9 D) | 40.21 ± 2.03D (range 33.9 to 43.9 D) | 0.15 ± 0.09 (range 0.01 to 0.34 μm) | 0.21 ± 0.13 (range 0.08 to 0.53 μm) | −0.04 ± 0.16 (range 0 to −0.5 D) | −0.36 ± 0.38D (range 0.21 to −1.025 D) | 40.39 ± 1.7 (range 38.24 to 43.7 D) | 0.13 ± 0.09 (range 0.01 to 0.32 μm) | 0.21 ± 0.09 (range 0.01 to 0.48 μm) |
a Spherical aberration and coma (μm) – 5.5 mm pupil diameter wavefront analysis (LADARWave, Alcon).
Mean epithelial thickness profiles evaluated by SD OCT preoperatively and at 1 week, 1 month, 3 months, and 9 months post femtosecond LASIK for myopia are shown in Table 2 .
| Epithelial Thickness Profile | Preoperative (μm) | 1 Week (μm) | 1 Month (μm) | 3 Months (μm) | 9 Months (μm) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Superior | Central | Inferior | Superior | Central | Inferior | Superior | Central | Inferior | Superior | Central | Inferior | Superior | Central | Inferior | |
| FS 200 (SD) | 52.75 ± 3.8 | 53.14 ± 2.2 | 54.63 ± 3.7 | 52.67 ± 4.7 P = .27 | 52.43 ± 3.1 P = .078 | 54.89 ± 4.2 P = .18 | 53.82 ± 2.9 P = .06 | 55.30 ± 3.7 P = .042 | 56.02 ± 3.9 P = .013 | 56.33 ± 6.3 P = .042 | 56.42 ± 5.6 P = .035 | 60.22 ± 7.4 P = .023 | 55.87 ± 6.1 P = .045 | 56.45 ± 4.3 P = .041 | 60.07 ± 6.3 P = .031 |
| IL 60 (SD) | 52.63 ± 3.5 | 53.21 ± 3.2 | 53.25 ± 2.2 | 52.0 ± 4.4 P = .19 | 51.93 ± 3.3 P = .057 | 53.44 ± 4.1 P = .2 | 53.79 ± 3.3 P = .071 | 56.33 ± 4.1 P = .033 | 56.45 ± 3.7 P = .007 | 56.56 ± 6.5 P = .04 | 57.07 ± 5.9 P = .042 | 59.44 ± 7.7 P = .031 | 56.01 ± 6.3 P = .044 | 56.89 ± 4.7 P = .043 | 59.09 ± 7.2 P = .035 |
At 1 week postoperatively, there appeared to be a trend for the epithelium to be thinner centrally in the IL and FS laser groups, but the difference was not statistically significant ( P = .057 and P = .078, respectively). Statistically significant epithelial thickening was observed in both IL and FS laser groups centrally ( P = .033 and P = .042) and inferiorly ( P = .007 and P = .013) at 1 month postoperatively in comparison with preoperative measurements. Superiorly, the epithelium was thicker at 1 month postoperatively but the difference was not statistically significant ( P = .071 and P = .06). At 3 and 9 months postoperatively the epithelium was thicker centrally ( P = .042 and P = .043 in the IL group; P = .035 and P = .041 in the FS group), inferiorly ( P = .031 and P = .035 in the IL group; P = .023 and P = .031 in the FS group), and superiorly ( P = .04 and P = .044 in the IL group; P = .042 and P = .045 in the FS group) in comparison with preoperative measurements ( Table 2 , Figures 3 and 4 ).



