Head and neck cancer is a unique cause of dysphagia. Altered swallow function can be secondary to the mechanical effects of a tumor invading normal anatomy needed for deglutition, or as a direct sequela of cancer treatment (surgery and/or radiation ± chemotherapy). This article outlines the incidence of head and neck cancer, effects of anatomic changes associated with common surgical intervention, and the consequences of treatment-induced dysphagia. Assessment and rehabilitation techniques applicable for this population are discussed.
Key points
- •
Persistent human papillomavirus (HPV) infection of the oral cavity may lead to genetic damage and altered immune function, promoting progression to cancer; specifically squamous cell carcinoma of the tonsils and base of tongue.
- •
Radiation and chemotherapy can have adverse effects on overall function and quality of life.
- •
Surgery can have devastating effects on swallow functioning, but results are somewhat predictable and dependent on the location of resection and clinical T stage.
| BOT | Base of tongue |
| CRT | Chemotherapy |
| HNC | Head and neck cancer |
| HPV | Human papillomavirus |
| IMRT | Intensity-modulated radiotherapy |
| MDADI | MD Anderson dysphagia inventory |
| TL | Total laryngectomy |
| XRT | Radiation therapy |
Introduction
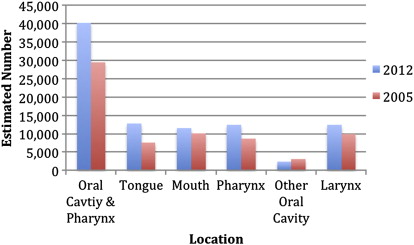
The incidence of head and neck cancer (HNC) has increased significantly over the past decade. According to the American Cancer Society, in 2012 an estimated 92,860 new cancer cases involved the oral cavity and pharynx, tongue, mouth, pharynx, other oral cavity, and larynx ( Fig. 1 ).
The steady increase in incidence rates of oropharyngeal cancer over the past several decades has been attributed to the growing number of human papillomavirus (HPV)–related cancers. More than 90% of HPV-positive oropharyngeal cancers are associated with 2 oncogenic high-risk HPV types: HPV 16 and HPV 18. Subtype HPV 16 has been associated with 85% to 90% of all HPV-positive oropharyngeal cancers. Persistent HPV infection of the oral cavity may lead to genetic damage and altered immune function, promoting progression to cancer; specifically squamous cell carcinoma of the tonsil and base of tongue.
HPV status has been strongly associated with therapeutic response and overall survival in patients with oropharyngeal cancer. In general, survival rates for HPV-related oropharyngeal cancer are higher than those for HPV-unrelated oropharyngeal cancers, with 2-year survival rates ranging from 80% to 95% versus 50% to 65%, respectively. However, treatment for HPV-related and HPV-unrelated oropharyngeal cancers are currently commensurate. To date, little research has been conducted to determine if functional outcomes, including swallowing physiology, are similar among these heterogeneous groups.
Surgery, chemoradiotherapy or a combination of treatment can alter both the anatomy and tissue characteristics of those structures and muscles involved in swallowing. Radiotherapy can affect muscles, nerves, and the vascular system. Injury to the neuromuscular junctures and radiation-induced neuropathy can result in impairment in nerve conduction, muscle fiber atrophy, necrosis, and impairment in muscle contraction with an increase in connective tissue. Vascular changes following irradiation have been found which result in tissue fibrosis as well as loss of muscle fibers, decreased fiber size and necrosis. The late effects of tissue fibrosis can have a negative impact on swallow functioning, with impairment in tongue and tongue base strength and range of motion, pharyngeal constrictor motion, reduced laryngeal motion for airway protection and upper esophageal sphincter opening and reduced bolus clearance through the pharynx. A reduction in both speed, strength and degree of structural movement within the oral cavity and pharynx can impact on bolus flow and clearance. Altered head and neck anatomy following surgery can result in swallowing deficits within the oral and pharyngeal phases of swallowing, depending on the specific structures resected. However, across treatment type, patients often exhibit impairment in bolus propulsion and clearance through the oral cavity and pharynx, as well as impairment in airway protection due to reduced glottic and supraglottic closure. Any of these deficits can result in bolus mis-direction and aspiration before, during or after the swallow.
Introduction
The incidence of head and neck cancer (HNC) has increased significantly over the past decade. According to the American Cancer Society, in 2012 an estimated 92,860 new cancer cases involved the oral cavity and pharynx, tongue, mouth, pharynx, other oral cavity, and larynx ( Fig. 1 ).
The steady increase in incidence rates of oropharyngeal cancer over the past several decades has been attributed to the growing number of human papillomavirus (HPV)–related cancers. More than 90% of HPV-positive oropharyngeal cancers are associated with 2 oncogenic high-risk HPV types: HPV 16 and HPV 18. Subtype HPV 16 has been associated with 85% to 90% of all HPV-positive oropharyngeal cancers. Persistent HPV infection of the oral cavity may lead to genetic damage and altered immune function, promoting progression to cancer; specifically squamous cell carcinoma of the tonsil and base of tongue.
HPV status has been strongly associated with therapeutic response and overall survival in patients with oropharyngeal cancer. In general, survival rates for HPV-related oropharyngeal cancer are higher than those for HPV-unrelated oropharyngeal cancers, with 2-year survival rates ranging from 80% to 95% versus 50% to 65%, respectively. However, treatment for HPV-related and HPV-unrelated oropharyngeal cancers are currently commensurate. To date, little research has been conducted to determine if functional outcomes, including swallowing physiology, are similar among these heterogeneous groups.
Surgery, chemoradiotherapy or a combination of treatment can alter both the anatomy and tissue characteristics of those structures and muscles involved in swallowing. Radiotherapy can affect muscles, nerves, and the vascular system. Injury to the neuromuscular junctures and radiation-induced neuropathy can result in impairment in nerve conduction, muscle fiber atrophy, necrosis, and impairment in muscle contraction with an increase in connective tissue. Vascular changes following irradiation have been found which result in tissue fibrosis as well as loss of muscle fibers, decreased fiber size and necrosis. The late effects of tissue fibrosis can have a negative impact on swallow functioning, with impairment in tongue and tongue base strength and range of motion, pharyngeal constrictor motion, reduced laryngeal motion for airway protection and upper esophageal sphincter opening and reduced bolus clearance through the pharynx. A reduction in both speed, strength and degree of structural movement within the oral cavity and pharynx can impact on bolus flow and clearance. Altered head and neck anatomy following surgery can result in swallowing deficits within the oral and pharyngeal phases of swallowing, depending on the specific structures resected. However, across treatment type, patients often exhibit impairment in bolus propulsion and clearance through the oral cavity and pharynx, as well as impairment in airway protection due to reduced glottic and supraglottic closure. Any of these deficits can result in bolus mis-direction and aspiration before, during or after the swallow.
Radiation therapy
Improvements in radiation therapy, including intensity-modulated radiotherapy (IMRT), and the addition of chemotherapy agents have dramatically shifted the care for HNC. The use of radiation therapy (XRT) ± chemotherapy, either as an adjunct to surgery or as a definitive treatment, has allowed for the development of organ-sparing treatments without a decrease in overall survival. However, these treatment modalities can have adverse effects on overall function and quality of life, causing side effects such as radiation dermatitis, pain, mucositis, soft tissue edema, weight loss, xerostomia, loss of taste, hoarseness, fibrosis, trismus, and dysphagia. Dysphagia is often the most problematic short-term and long-term effect seen in this population. Long-term dysphagia often results in critical consequences, including aspiration and dietary inadequacies, leading to malnutrition and its associated adverse effects.
The reported incidence rates of dysphagia after XRT and chemotherapy are highly variable. Nguyen and colleagues reported an average incidence of dysphagia of 50% after chemotherapy for advanced-stage HNC. Others have reported as many as two-thirds of all patients with HNC are left with permanent swallowing problems. These problems directly impact an individual’s nutritional status, hydration, and pulmonary health in addition to having a major impact on quality of life.
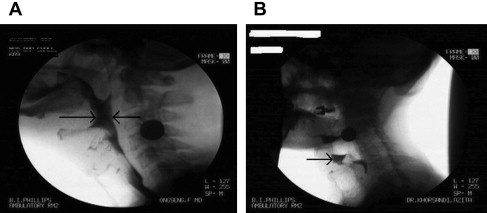
Characteristics of dysphagia secondary to XRT or chemotherapy depend primarily on tumor size and the presence or absence of metastatic neck disease. These features greatly impact the radiation field and dose required for definitive treatment. Common physiologic deficits and their impact on bolus transport are outlined in Table 1 . Impaired base of tongue retraction and reduced hyolaryngeal elevation have been identified as 2 of the most salient features of dysphagia after XRT ( Fig. 2 ). Lingual strength in patients with oral and oropharyngeal cancer treated with primary chemotherapy has been found to be lower than in that seen in healthy controls. Lingual strength has also been found to correlate with aspiration.
| Oral | Impairment |
|---|---|
| Trismus | Inability to open mouth to accept oral intake Impaired chewing |
| Dry mouth | Reduced range of motion of oral structures Impaired oral transit Difficulty breaking down food without saliva enzymes Increased risk of caries |
| Lingual weakness | Impaired bolus formation Impaired anteroposterior transport and bolus clearance leading to oral residue Lateral sulci residue |
| Pharyngeal | Impairment |
|---|---|
| Decreased base of tongue retraction | Impaired bolus propulsion Pharyngeal residue Increased number of swallows |
| Reduced laryngeal elevation/excursion | Impaired epiglottic inversion Impaired airway protection Penetration/aspiration Reduced opening of the cricopharyngeal segment resulting in pharyngeal residue |
| Impaired contraction of the pharyngeal constrictors | Impaired bolus transport and clearance through the pharynx Reduced opening of the cricopharyngeal segment resulting in pharyngeal residue |
| Stenosis of the cricopharyngeal segment | Reduced or absent bolus clearance resulting in pharyngeal residue |
Radiation treatment for HNC has shifted primarily to IMRT over the past decade. This shift has allowed for the delivery of nonuniform radiation intensities to various structures, thus protecting structures important for swallowing when possible. A recent study has compared physiologic measures of swallow functioning after IMRT versus conventional radiotherapy. Results indicate that individuals treated with IMRT maintain better swallow function with regard to timing, efficiency, and airway protection compared with individuals treated with conventional radiotherapy.
Undoubtedly, given the incidence of dysphagia in the population and the negative impact on swallow function and safety, the potential role of intervention during treatment is increasingly recognized as a means of maintaining oropharyngeal function. Although early treatment is recommended, it has not been operationally defined at this time. Few studies have looked at prophylactic swallowing intervention by way of muscle strengthening. However, only 2 of these studies were randomized controlled trials, with only 1 including a control group. All studies differed in outcome measures. These studies are outlined in Table 2 .
| Author | Outcome Measures | Therapy Exercises | Onset of Exercises | Results |
|---|---|---|---|---|
| Van der Molen et al, 2011 a |
|
| 2 wk before chemoradiation | Significant decrease in mouth opening, weight loss, and oral intake for both groups No significant difference between the pretreatment and posttreatment PAS scores |
| Carnaby-Mann et al, 2012 a |
|
| At the start of chemoradiation | Significant differences were seen in superior muscle maintenance and functional swallowing ability |
| Kulbersh et al, 2006 |
| Falsetto Masako Mendelsohn Shaker Lingual resistance (all participants) | 2 wk before radiation ± chemotherapy | Improved QOL measures: physical, emotional, global No improved QOL in the functional domain |
| Carroll et al, 2008 |
|
|
| Significant differences in epiglottic inversion and tongue position during swallow No difference in PEG removal |
| Kotz et al, 2012 |
|
| At the start of chemoradiation | FOIS and PSS-HN: no significant difference immediately after CRT or at 9 or 12 mo after CRT Significant differences at 3 and 6 mo after CRT |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


