Slit-Lamp Biomicroscopy and Photography
Mark P. Hatton
Lawrence M. Merin
Slit-lamp biomicroscopy of the anterior segment provides the ability to view an illuminated tissue under high magnification. It is not one technique. Rather, various methods of examination are used by adjusting the illumination intensity, beam width, viewing angle, and magnification of the slit-lamp biomicroscope. Alone, each method offers a unique perspective into the normal or abnormal tissue under investigation. Together, the dynamic process of slit-lamp biomicroscopy provides the examiner a complete picture of the nature of the healthy and diseased anterior segment.
EXAMINATION TECHNIQUES
Diffuse Broad-Beam Illumination
Opening the aperture of the slit to its widest setting creates a full, broad illuminating beam. The intensity of this beam can be dampened by the introduction of the neutral density filter to reduce the discomfort experienced by the patient. The wide beam provides diffuse illumination such as would be obtained from the illumination provided by a penlight or muscle light.
This technique is used to perform a general inspection of the anterior segment and adnexal structures under low magnification. It offers the observer the “big picture,” which might otherwise be missed if an area of interest is immediately isolated with high magnification. This technique is useful in assessing the overall degree of ocular erythema, identifying areas of corneal opacity or surface irregularity, localizing corneal and conjunctival foreign bodies, and determining patterns of normal and abnormal pigmentation (Fig. 6-1).
Examination with broad-beam illumination should also be performed while the light source is actively rotated from side to side. As the beam is applied tangentially at different angles, variations in elevation and depressions are emphasized and contrast is increased. This permits the observer to determine whether the lesion of interest is flat or if it has any degree of elevation (Fig. 6-2).
Focal Illumination
By narrowing the beam and shortening its height, the examiner can create a “spotlight” to permit viewing an object of interest in isolation without illuminating surrounding tissues. An essential derivative of this technique is the optical section. The slit-lamp biomicroscope provides the unique ability to view an optical cross section of the semitransparent (i.e., translucent) tissues of the eye (cornea, aqueous, lens) in vivo. Although the vast majority of light rays pass through the cornea unimpeded, slight irregularities in its substance result in reflection of light back to the examiner. This fact can be used to localize abnormalities to one or more layers of the cornea. Rotating the illumination arm allows the narrow slit beam to strike obliquely the lesion of regard. When angled at 45 degrees from the observation axis, maximal information about the internal structure of the cornea is revealed. At a lesser angle, the optical section collapses, whereas more than 45 degrees decreases brightness and gives a false impression of angular distance between the corneal layers.
The slit lamp is designed so that the slit beam and biomicroscope are focused at the same plane, thus allowing for movement of the illumination and viewing arms by the examiner to appreciate best the nature and depth of the lesion while remaining in focus. With this slit-beam technique, each layer of the cornea and tear film may be examined. Thus, the location of a lesion in the cornea may be determined by noting where it falls in the optical section. (Fig. 6-3).
The thin slit beam also permits the examiner to note the thickness and curvature of the cornea. Localized depressions result in the beam of light appearing to bend posteriorly. Similarly, elevated lesions within the cornea cause the light beam to appear to bend toward the observer (Fig. 6-4). This ability to detect changes in thickness may also be applied to the conjunctiva, where deviation in the appearance of the slit beam can detect elevations and depressions.
Focal illumination with a small, narrow slit beam also permits examination of the aqueous. The normal aqueous is transparent: Light rays pass through it unimpeded. White blood cells or increased protein content (flare) present during
inflammation result in reflection of light, or Tyndall’s phenomenon. A 0.2 × 0.2 light beam is applied at an oblique angle. On Haag-Streit and similar instruments, the light tower should be tilted forward. This technique is enhanced by observing the findings in the light beam against the black background provided by the pupil. The degree of inflammation is graded using a standard system (Tables 6-1 and 6-2).
inflammation result in reflection of light, or Tyndall’s phenomenon. A 0.2 × 0.2 light beam is applied at an oblique angle. On Haag-Streit and similar instruments, the light tower should be tilted forward. This technique is enhanced by observing the findings in the light beam against the black background provided by the pupil. The degree of inflammation is graded using a standard system (Tables 6-1 and 6-2).
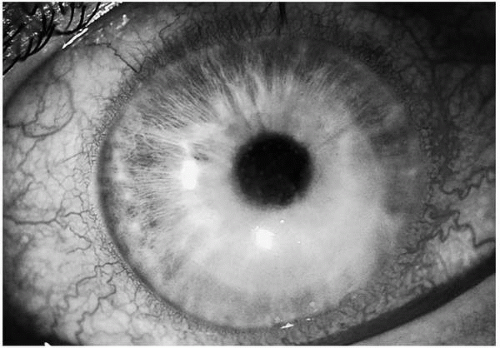 FIG. 6-1. Diffuse, broad-beam illumination of a patient with herpes simplex keratouveitis. The low magnification combined with diffuse illumination permits the examiner to comprehend the “big picture.” In this case, this technique documents ciliary flush, keratic precipitates, and corneal edema.(see color image) |
SPECULAR REFLECTION
Examination of the cornea with any light source results in the reflection of the light source back toward the examiner (e.g., corneal light reflex). This phenomenon obeys Snells’s law stating that the angle of incidence is equal to the angle of reflection. To observe objects in the cornea by specular reflection, the examiner must align the angle of observation to be equal with the angle of light directed toward the cornea.
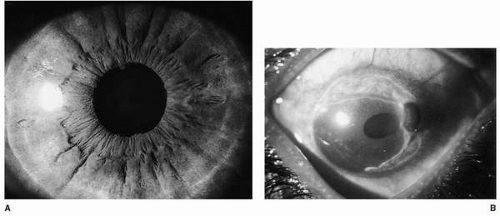 FIG. 6-2. A. Tangential illumination with a broad beam of a normal iris. The observed shadows result from elevations on the iris surface. This technique can permit the examiner to determine whether an observed lesion is flat or elevated. B. Tangential illumination of an eye with Mooren’s ulcer with perforation. The protruding iris casts a shadow, suggesting it is elevated above the plane of the cornea.(see color image) |
Specular reflection occurs both at the epithelium-tear interface as well as the endothelial-aqueous interface. The corneal light reflex, due to specular reflection from the epithelium-tear interface, is usually crisp and well defined. Any disruption in the surface of the cornea does not permit uniform reflection of light, which suggests areas of discontinuity or irregularity of the corneal surface.
Focusing the beam deeper into the cornea permits observation of specular reflection from the endothelial-aqueous interface. This method allows for visualization of the endothelial cells and can accentuate abnormalities, such as abnormal morphology characteristic of endothelial cell damage (Fig. 6-5).
The examination techniques discussed to this point rely on direct illumination of the object of interest by the light source. Additional information can be obtained by viewing the object of interest with light reflected from another location.
Sclerotic Scatter
Total internal reflection of light rays in the anterior segment requires the use of a gonioscopy lens to view the angle structures. Similarly, a portion of the light rays directed at the cornea undergoes total internal reflection between the anterior and posterior corneal surfaces. This can be maximized by directing the light beam at the corneoscleral junction. In the normal cornea, this technique results only in a faint glow at the limbus; the remainder of the cornea is not affected and remains clear. However, irregularities in the cornea, if present, cause the light being reflected in the stroma to be scattered and, in part, reflected toward the examiner (Fig. 6-6).
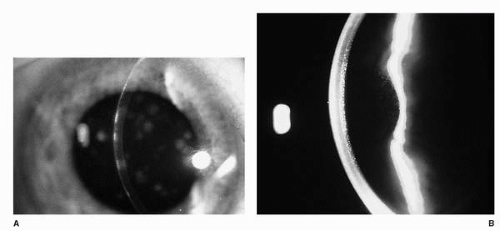 FIG. 6-3. A. In this photograph, the opacities that occurred during the course of adenoviral infection were located in the first part of the optical section, suggesting localization to the subepithelium or anterior stroma. B. Optical section of a cornea with Fuchs’ dystrophy. In this photograph, the abnormality (guttata) exists in the most posterior aspect of the slit beam, consistent with the endothelial location of the lesion. |
Sclerotic scatter is performed by directing the light beam tangentially toward the limbus until the entire limbal circumference appears to glow. Observation of the cornea is then performed. This technique is particularly useful for detecting subtle irregularities that might be missed with other examination techniques.
RETROILLUMINATION
Retroillumination is the technique of visualizing structures against an illuminated background. The beam of light, directed at a location more posterior than the object of interest, is reflected and viewed in its return pathway toward the examiner. Objects in this returning beam’s path block the transmission of light, thus permitting them to be visualized in silhouette. This is most frequently performed by directing light toward the pupil to create the familiar red reflex from the posterior segment (Fig. 6-7). However, retroillumination of the cornea can also be performed by directing the light beam at the iris (Fig. 6-8). Objects can appear different with each source of back-lighting (fundus or iris), and each can provide a different perspective to the examiner.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


