In the Pickwick Papers, Charles Dickens described a syndrome of obesity and hypersomnolence. Later, in 1906, William Osler noted that “an extraordinary phenomenon in excessively fat young persons is an uncontrollable tendency to sleep—like the fat boy in Pickwick.” Active research on sleep disorders began in the 1950s and 1960s when multiple reports associated obesity, hypersomnolence, alveolar hypoventilation, and cor pulmonale with the syndrome of obstructive sleep apnea (OSA).
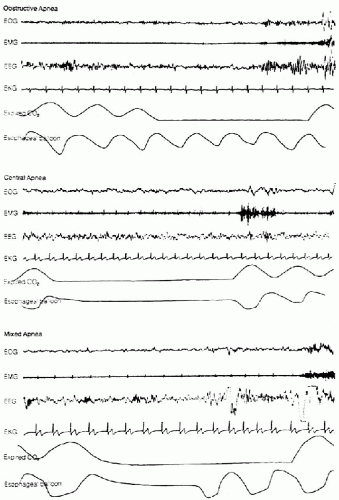
Obstructive sleep-disordered breathing is viewed as a continuum of severity ranging from primary snoring to upper airway resistance syndrome (UARS) to OSA. Patients with primary snoring have no sleep architecture disturbance or gas exchange abnormalities. Patients with UARS demonstrate abnormally increased upper airway resistance during sleep, resulting in increased respiratory effort and sleep fragmentation but with no apnea, hypopnea, or desaturations. Sleep apnea can be central (cessation of respiratory effort), obstructive (obstruction of airflow), or mixed (Fig. 20-1). An older definition of an apneic event is the absence of airflow at the level of the nares and mouth for longer than 10 seconds in a child or adult and 15 seconds in an infant (6 months or younger). Since children have faster respiratory rates than adults, the current definition of apnea in a child is the cessation of airflow for 1½ to 2½ breath intervals or about 6 seconds. Hypopnea is defined as the reduction in tidal ventilation with an associated decrease in arterial oxygen saturation. Polysomnography (PSG) is the gold standard for diagnosis with measurement of sleep stage, airflow, respiratory effort, chest wall movements, heart rate, and pulse oximetry. As quantified on the PSG, the respiratory disturbance index (RDI) is the number of apneas plus hypopneas per hour of sleep. In adults, OSA is defined as an RDI of 15 or higher. In children, an RDI at least 5 or an apnea index (number of apneas per hour) of at least 1 is considered abnormal. Desaturation below 92% is also considered abnormal in both adults and children.
The characteristic event in OSA is the collapse of the upper airway during inspiration during sleep. Upper airway collapse occurs when the negative pressure from inspiration exceeds the ability of the pharyngeal walls to resist collapse. The function of the pharyngeal abductor and dilator muscles is to maintain pharyngeal patency. Pharyngeal muscle activity decreases during some sleep states. During rapid eye movement sleep, there is an increase in heart and respiratory rate and concomitant hypotonia of skeletal muscles, except for the diaphragm. At these times, airway stability depends on pharyngeal size and tissue compliance. When upper airway muscle activity decreases, the airway may not be maintained. The most common and recognizable sign of sleep apnea is sonorous snoring, which is a sign of airway turbulence and partial obstruction. The sound results from vibrations of lax tissues when air passes over them. Approximately 30% of snorers have evidence of OSA.
FIG. 20-1. Types of apnea and their typical somnographic recordings. EOG, electro-oculogram; EMG, electromyogram; EEG, electroencephalogram; EKG, electrocardiogram. (From Hauri PJ.Current concepts: the sleep disorders. Kalamazoo, MI: Upjohn, 1982, with permission.)
Conditions that reduce airway dimensions, such as obstructing lesions or craniofacial morphologic features, may result in OSA. Any anatomic narrowing of the upper airway requires increased negative inspiratory pressure to maintain ventilation. This increase in negative pressure increases the probability of pharyngeal collapse. The site of obstruction in OSA lies between the nasopharynx and supraglottic larynx, particularly in the adenoid pad, pharyngeal tonsils, soft palate, tongue, and lingual tonsils. Among individual patients, the area of obstruction usually remains constant. Diagnosis of the site of lesion is imperative for direct management of the problem.
Central apnea, the cessation of airflow without inspiratory effort, is not as frequently seen as obstructive apnea. Increases in PCO2 detected by central and peripheral chemorecoptors stimulate increased ventilation. For many patients, central apnea is seen after the hyperventilation following obstructive events. These central apneic events apparently are caused by hyperoxia and hypocarbia, which leads to a decrease in ventilatory drive. A combination of obstructive and central apnea is called mixed apnea. In this disorder, periods of airway obstruction are associated with intervals of no respiratory effort. Obstructive events often are associated with a decrease in oxygen saturation and are typically terminated by brief arousals from sleep, which transiently increase pharyngeal muscle activity to maintain airway patency. Repeated obstructive events, either partial or complete, with corresponding decreases in oxygen saturation are believed to be the cause of long-term medical consequences.
NEWBORNS AND INFANTS
Sleep disorders caused by airway obstruction can be seen in newborns and infants (Table 20-1). Infants are more susceptible than adults to irregularities of respiration because of smaller airway dimensions, faster respiratory rates, obligate nasal breathing, and differences in sleep and wake patterns. Among preterm infants, brief apneic events may be common, and these events normally resolve as maturation of the central and peripheral nervous systems, the upper airway, and the bronchopulmonary tree occur. Although brief central apneic events may be common among infants, episodes lasting longer than 15 seconds are considered abnormal.
Congenital anomalies include laryngomalacia, laryngotracheal defects, vascular rings, pharyngeal encephaloceles, and compressive neck masses. In some craniofacial disorders, there are multiple sites of obstruction. Upper airway obstruction occurs in the Pierre-Robin sequence as a result of micrognathia, relative macroglossia, and pharyngeal hypotonia. A common cause of OSA is posterior nasal obstruction caused by bilateral choanal stenosis or atresia. Bilateral vocal cord paralysis from Arnold-Chiari malformation is one of several nervous system disorders that can lead to obstruction. Gastroesophageal reflux is a disorder with a significant association with apnea. The presence of acid and pepsin reflux may lead to obstruction via laryngospasm or central apnea through vagal reflux inhibition of respiration. Among older infants, the most common cause is hypertrophic tonsils and adenoids. OSA in infants may play a role in infants dying from sudden infant death syndrome (SIDS), although the etiology of SIDS remains unknown.
TABLE 20-1. Causes of symptomatic apnea of infants
Chronic hypoxemia from bronchopulmonary dysplasia or other intrinsic lung disease
Diagnosis
The history is of paramount importance in diagnosing and managing apnea among infants. It can help establish whether the infant had an apneic episode, a choking episode, or a seizure. The physical examination provides information about congenital abnormalities of the upper airway and craniofacial skeleton. PSG is the standard for the diagnosis of sleep apnea. Additional studies include electroencephalography, radiographic films, and both flexible and rigid endoscopy.
Treatment
Treatment of infants with apnea has two main goals. Elimination or control of the underlying disorder is the primary concern. Second, management is aimed at preventing complications. Complications include pulmonary hypertension, cor pulmonale, metabolic alkalosis, chronic hypoxemia, and failure to thrive. Central apnea syndromes are best managed with medical therapy. Methylxanthines are respiratory stimulants commonly used to manage infantile central apnea. In obstructive apnea, nasal continuous positive airway pressure (CPAP) can be used to increase oxygenation and prevent airway collapse. CPAP may be used as a sole treatment or in combination with surgical therapy. Procedures such as adenotonsillectomy, supraglottoplasty, choanal atresia repair, and tracheotomy correct specific obstructive conditions.
Only gold members can continue reading. Log In or Register to continue