Purpose
To describe characteristics of patients with severe limbal stem cell deficiency associated with contact lens (CL) wear.
Design
Retrospective case series.
Methods
Database search of patients with severe limbal stem cell deficiency related to CL wear was conducted. The charts of 12 patients (18 eyes) were reviewed. Outcome measures included patient demographics, CL type, duration of wear, indications for wear, symptoms, location and laterality of limbal stem cell deficiency, coexisting ocular disease, and treatment.
Results
Mean patient age at presentation was 42 years (range, 19 to 58 years), and 8 patients (67%) were female. Mean duration of CL wear was 14.1 years (range, 1 to 20 years), 6 patients (50%) had bilateral disease, and all wore soft CLs for refractive error correction. Vision was decreased to a mean of 20/78 (range, 20/30 to 20/250) in all eyes. Fifteen eyes (83%) had photophobia, pain, or both. Findings leading to the diagnosis included whorl-like epitheliopathy, corneal conjunctivalization, and late fluorescein staining of the involved epithelium for at least 6 clock hours. On average, 10 clock hours (range, 6 to 12 clock hours) were involved, and 11 eyes (61%) had total ocular involvement. Conservative treatments failed in all eyes. Fourteen eyes (78%) underwent limbal stem cell transplantation with systemic immunosuppression.
Conclusions
Severe limbal stem cell deficiency related to CL wear is a clinical diagnosis that an ophthalmologist should recognize. Female patients, soft CLs, and extended duration of wear time are associated with this condition. Conservative measures may not reverse the disease, and limbal stem cell transplantation with systemic immunosuppression is a surgical option for these young and healthy patients.
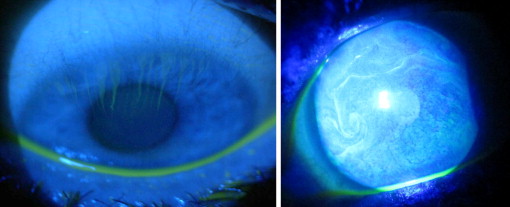
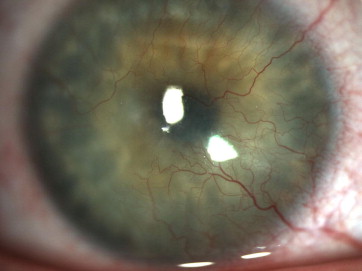
Normal limbal stem cells are required for a stable corneal epithelium to exist. They also serve as a barrier to prevent conjunctival epithelial cells from invading the corneal surface. A classic pattern of late fluorescein staining occurs in limbal stem cell deficiency ( Figure 1 ) because of the increased permeability of abnormal epithelial cells to the level of conjunctiva. Histologic analysis has shown the invasion of conjunctival goblet cells into the corneal epithelium in limbal stem cell deficiency. Sequelae of limbal stem cell deficiency include persistent epithelial defects, corneal conjunctivalization ( Figure 2 ), corneal scarring, and chronic inflammation, leading to potential vision loss, chronic pain, photophobia, and keratoplasty failure.
In the staging of ocular surface disease, it is important to determine how much of the limbal stem cells are deficient and the inflammatory status of the conjunctiva ( Table 1 ). Although chemical injuries, Stevens-Johnson syndrome, and ocular cicatricial pemphigoid are commonly recognized causes of severe limbal stem cell deficiency, the role of contact lens (CL) wear in severe cases of limbal stem cell deficiency is less well understood. Only a few studies have described limbal stem cell deficiency from CL wear. The purpose of this study was to describe the characteristics of severe limbal stem cell deficiency related to CL wear in a larger group of patients. Recognizing this condition is important to the ophthalmologist, who can ensure prompt referral to an ocular surface diseases specialist.
| Stage A: Normal Conjunctiva | Stage B: Previously Inflamed Conjunctiva | Stage C: Inflamed Conjunctiva | |
|---|---|---|---|
| Stage 1: < 50% limbal stem cell deficiency | Contact lens wear, iatrogenic, CIN | History of chemical or thermal injury | Mild SJS, OCP, recent chemical or thermal injury |
| Stage 2: > 50% limbal stem cell deficiency | Aniridia, iatrogenic, severe contact lens wear | History of severe chemical or thermal injury | Severe SJS, OCP, recent chemical or thermal injury |
Methods
This retrospective, observational case series was deemed exempt from the Research Ethics Board by the Institutional Review Board of St. Elizabeth’s Health Care, Edgewood, Kentucky (institutional review board no. 4/2011-009). This study was conducted in compliance with the tenets of the Declaration of Helsinki.
A Database search of patients seen over a 10-year period with a diagnosis of limbal stem cell deficiency was conducted at a cornea clinic at the Cincinnati Eye Institute, Cincinnati, Ohio. The charts of 18 eyes from 12 patients who were identified to have a diagnosis of severe limbal stem cell deficiency and a history of CL wear were reviewed retrospectively. Patients were excluded if they had a history of chemical injury, Stevens-Johnson syndrome, ocular cicatricial pemphigoid, multiple prior ocular surgeries, and long-term topical glaucoma drop use. Outcome measures that were analyzed included patient demographics, type of CL used, duration of CL wear, indications for CL wear, presenting symptoms, location and laterality of limbal stem cell deficiency, coexisting ocular disease, and treatment methods used.
Results
Individual patient and ocular details are shown in Table 2 . The average age at diagnosis in this cohort of patients was 42 years (standard deviation [SD], 12 years; range, 19 to 58 years old). Most patients (67%; 8/12) were female. The mean duration of CL wear was 14.1 years (SD, 7 years; range, 1 to 20 years), and 78% (14/18) eyes had between 10 and 20 years of CL use. All patients wore CLs for the correction of refractive error and reported daily usage of 10 or more hours. Bilateral severe limbal stem cell deficiency was present in 50% (6/12) of patients, all wore soft CLs only, and 58% (7/12) of patients had coexisting ocular disease or prior ocular insult (thimerosal exposure, severe meibomian gland dysfunction, rosacea blepharokeratoconjunctivitis, viral conjunctivitis, allergic conjunctivitis, and low serum vitamin A levels associated with having undergone gastric bypass).
| Case No. | Patient No. | Age (y) | Eye | Sex | BCVA | Duration of Soft CLW (y) | Daily Wear Time (h) | Past Ocular History | Symptoms | No. of Clock Hours of Conjunctivalization | Other Findings | Surgical Treatment | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Photophobia | Pain | Red Eye | Tearing | ||||||||||||
| 1 | 1 | 27 | R | M | 20/40 | 4 | 10 | — | + | + | 12 | Stromal haze | LR-CLAL | ||
| 2 | 2 | 19 | L | M | 20/250 | 6 | 12 | Severe viral keratoconjunctivitis | + | + | 12 | Filaments | KLAL OS | ||
| 3 | 3 | 43 | R | F | 20/200 | 20 | 14 | — | + | 12 | Stromal haze | LR-CLAL | |||
| 4 | 3 | 43 | L | F | 20/40 | 20 | 14 | — | + | 6 (superior) | Subepithelial fibrosis | LR-CLAL | |||
| 5 | 4 | 50 | L | F | 20/70 | 20 | 15 | Severe MGD | + | + | + | 12 | Epithelial defect, scar | KLAL and lateral tarsorrhaphy | |
| 6 | 4 | 50 | R | F | 20/80 | 20 | 15 | Severe MGD | + | + | + | 12 | Epithelial defect, scar | KLAL and lateral tarsorrhaphy | |
| 7 | 5 | 42 | R | M | 20/50 | 20 | 13 | — | + | + | 12 | Stromal scarring | KLAL | ||
| 8 | 6 | 58 | L | F | 20/70 | 20 | 10 | — | + | 9 (superior) | Stromal haze, epithelial defect | KLAL | |||
| 9 | 6 | 58 | R | F | 20/30 | 20 | 10 | — | + | 6 (superior) | Stromal haze | KLAL | |||
| 10 | 7 | 55 | R | F | 20/60 | 1 | 12 | Thimerosal exposure | + | 12 | Stromal haze | LR-CLAL | |||
| 11 | 8 | 27 | R | F | 20/80 | 3 | 10 | — | + | 12 | — | Observation | |||
| 12 | 9 | 28 | R | F | 20/80 | 10 | 14 | Rosacea MGD | + | + | 6 (superior) | — | Losing weight to qualify for systemic immunosuppression | ||
| 13 | 9 | 28 | L | F | 20/200 | 10 | 14 | Rosacea MGD | + | + | 6 (superior) | — | |||
| 14 | 10 | 29 | R | M | 20/60 | 10 | 12 | Severe allergic conjunctivitis | + | + | + | 12 | — | Observation | |
| 15 | 11 | 50 | L | F | 20/250 | 15 | 15 | Gastric bypass, low serum vitamin A levels | 12 | — | KLAL | ||||
| 16 | 11 | 50 | R | F | 20/100 | 15 | 15 | Gastric bypass, Low serum vitamin A levels | 12 | — | KLAL | ||||
| 17 | 12 | 47 | R | F | 20/60 | 20 | 14 | Rosacea MGD | + | + | 10 (superior) | Subepithelial fibrosis | KLAL | ||
| 18 | 12 | 47 | L | F | 20/40 | 20 | 14 | Rosacea MGD | + | + | 8 (superior) | — | KLAL | ||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


