Secondary Epithelial Neoplasms
The secondary epithelial neoplasms encroach upon the orbit from contiguous sites such as the nasal cavity and paranasal sinuses; lacrimal sac; caruncle; parotid gland; external surface of the eye; and skin of the forehead, eyelids, and temple.
Features common to the secondary epithelial neoplasms are their variable presentation, radiologic evidence of bone destruction, and a slow relentless course. They are difficult to eradicate by the present treatment modalities, have a high rate of recurrence, and a discouraging death rate. Their presentation varies according to where they enter the orbit. If the tumor invades the anterior orbit either from an adjacent paranasal sinus or from the surface of the eyelids or face, there is usually a palpable mass or fullness of the cheek or medial canthal area, an upward or lateral displacement of the eye, epiphora, and a mass effect influencing ocular motility. If the tumor enters the posterior orbit, there may be pain or numbness over the superficial branches of the trigeminal and facial nerves, visual loss, papilledema, afferent pupillary disturbance, and ophthalmoplegia.
Neoplasms of this type from the Mayo Clinic Series, 1,795 consecutive cases (1948 to 1997), are listed according to their histopathologic type and order of frequency in Table 16.1.
As a group, these neoplasms are three times more frequent (252:80) in the orbit as the primary epithelial neoplasms discussed in Chapter 15. These secondary tumors comprise 14% of the total of 1,795 tumors studied by us over a 50-year period. In past years, the literature contained several reports wherein the incidence of secondary tumors was based on large patient cohorts. These reports were not comparable to our own because their analyses were not limited to epithelial neoplasms.
Squamous Cell Carcinoma
This is the most frequent carcinoma (133 cases) in the total of 1,795 consecutive, histopathologically proved orbital tumors. Secondary squamous cell carcinomas, alone, constitute 6.8% (122 of 1,795 tumors) of the total tumors. Table 16.2 illustrates the primary source of the secondary neoplasms at the time of orbital invasion, as also the sex ratio and mean age of the patients.
Patients with lesions on the eyelids, eyebrow, or surface of the eye and an obstruction along the nasolacrimal excretory duct were usually first seen by an ophthalmologist. Ulcerative and nodular lesions of the cheeks, nose, forehead, and temple were usually first diagnosed by the patients’ family physician.
Patients whose carcinoma, on subsequent examination, would prove to have an origin in the ethmoidal sinus would present with some combination of displacement of the eye, unilateral proptosis, pain, and a palpable mass suggesting an orbital tumor. However, only a small minority of the large number of carcinomas in the maxillary sinus and nasal passage presented as an orbital disorder.
The presenting signs and symptoms of paranasal sinus and nasal carcinomas were chiefly rhinologic in nature. In order of decreasing frequency, these included a mass or swelling of the cheek, pain or paresthesia of the face, a mass along the alveolar ridge of the maxilla, a sore gum, numbness of the face, nasal mass, history of polypectomies, epistaxis, nasal obstruction, and orbital apex syndrome. Some combination of two or more of these findings was present in all patients. The orbital manifestations of proptosis, displacement of the eye, and diplopia with or without a palpable orbital mass would follow at some variable interval after the onset (see Fig. 16.1).
The orbital manifestations of the few cases of nasopharyngeal carcinoma were those of the orbital apex syndrome (papilledema, trigeminal nerve paresthesias or anesthesia, optic disk pallor, ophthalmoplegia, afferent pupillary defect, and severe visual loss) indicating an extension of the tumor along the base of the skull.
Orbital extension from neoplasms of the adnexal tissues and lacrimal sac was more straightforward. These patients usually had a history of multiple surgical procedures on
a nodular or ulcerative mass, which finally invaded the contiguous orbit. A hard mass would be palpable along the affected orbital rim, and the motility of the eye would be increasingly impaired (see Fig. 16.2). These patients did not have the pain and discomfort associated with squamous cell carcinoma in other orbital sites unless the lesion was well advanced.
a nodular or ulcerative mass, which finally invaded the contiguous orbit. A hard mass would be palpable along the affected orbital rim, and the motility of the eye would be increasingly impaired (see Fig. 16.2). These patients did not have the pain and discomfort associated with squamous cell carcinoma in other orbital sites unless the lesion was well advanced.
Table 16.1 Secondary Epithelial Neoplasms Mayo Clinic Series, 1948 to 1997 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
In the Mayo Clinic Series, squamous cell carcinoma of the lower eyelid is nearly as frequent as the lesion in the upper eyelid.
Imaging Aspects
Both magnetic resonance imaging (MRI) and computed tomography (CT) scan are useful in the diagnosis and management of these neoplasms when orbital invasion occurs. MRI is considered the imaging modality of choice for soft tissue definition and CT scan is best for revealing the location and extent of bone destruction, which is invariably present. The lesions are usually homogeneous, highly attenuated in character, and enhance to some degree (see Fig. 16.3). Physicians working in this field for long have been hopeful these imaging modes would be helpful in determining the presence and degree of perineural spread.
Nemzek et al. (1998) reported a sensitivity of 95% for MRI detection of perineural spread but only a 63% sensitivity for mapping the entire extent of the process. Contrarily, despite a clinical suspicion of perineural spread, de Keizer et al. (1997) did not find either imaging method helpful in determining nerve extension. Preoperative detection of insidious but not clinically visible perineural spread is almost always a component of secondary orbital squamous cell carcinoma. The image display of perineural spread is an enlarged or expanded cord-like structure extending outward from the periphery of the mass lesion (Veness and Biankin, 2000), as it may be a solitary structure appearing on an image plane beyond the carcinomatous mass.
Nemzek et al. (1998) reported a sensitivity of 95% for MRI detection of perineural spread but only a 63% sensitivity for mapping the entire extent of the process. Contrarily, despite a clinical suspicion of perineural spread, de Keizer et al. (1997) did not find either imaging method helpful in determining nerve extension. Preoperative detection of insidious but not clinically visible perineural spread is almost always a component of secondary orbital squamous cell carcinoma. The image display of perineural spread is an enlarged or expanded cord-like structure extending outward from the periphery of the mass lesion (Veness and Biankin, 2000), as it may be a solitary structure appearing on an image plane beyond the carcinomatous mass.
Table 16.2 Secondary Orbital Squamous Cell Carcinomas Mayo Clinic Series, 1948 to 1997 | ||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
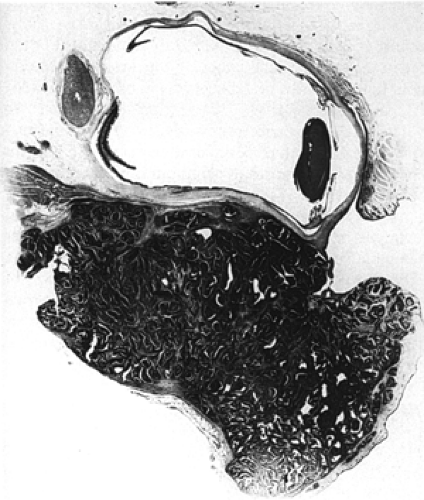 Figure 16.1 Gross specimen of a squamous cell carcinoma of the maxillary sinus showing massive, secondary invasion of inferior orbit from a 67-year-old man with 3 months’ swelling of left upper face and 1 month epiphora (× 2½. |
 Figure 16.2 A 23-year-old woman with nodular and ulcerating lesions at the medial portion of the right upper and lower eyelids from a squamous cell carcinoma with secondary extension into the orbit. Several months earlier, an “infection” at the medial canthus had been treated by a dacryocystotomy. Origin of the lesion was the lacrimal sac. Secondary orbital squamous cell carcinoma, an extension from a lower eyelid. |
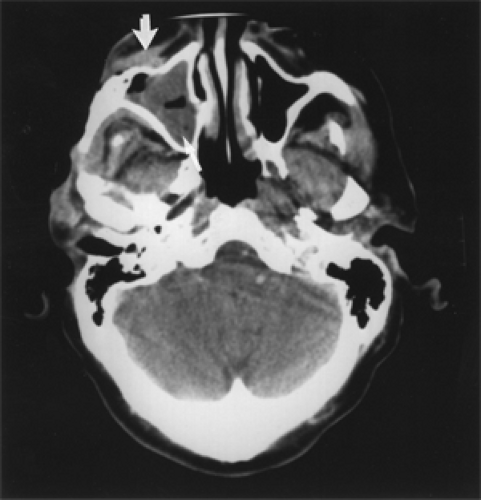 Figure 16.3 Squamous cell carcinoma: Axial computed tomography (CT) scan shows homogeneous mass occupying right maxillary sinus (lower arrow) with extension into right cheek (upper arrow) of a 59-year-old man. Subsequent maxillectomy also showed extension into right orbit, although this was not evident on preoperative scan. |
Pathology
In a small zone around the anterior nares, squamous epithelium is normally arranged in a pavement-like pattern similar to that of skin. Elsewhere in the upper respiratory passages, squamous epithelium has undergone functional modification into a pseudostratified, sometimes ciliated, epithelium. The histologic pattern of this epithelium is, however, alike everywhere, but it varies according to the functional purposes of the specific anatomic sites. In the mucous membranes of the sinuses and anterior nasal cavity, the epithelium is ciliated and less stratified than in skin but it still possesses some characteristics of keratinization of skin. In the more posterior recesses of the nasal cavity, the epithelium becomes more columnar with little or no keratinization. This histologic pattern is frequently referred to as a transitional type of epithelium. In the nasopharynx, the epithelium becomes but a loose and thin layer of squamous cells covering a predominantly lymphocytic-adenoid type of stroma. Such an arrangement is usually termed a lympho-epithelial type of respiratory epithelium. Lower down the respiratory passages, squamous cell surfaces show further changes that make possible their identification with a specific anatomic area when tissue specimens are examined microscopically. The carcinomas, in their growth, reflect these nuances in cellular morphology, but basically, all of them represent malignant squamous metaplasia.
Squamous cell carcinomas of the maxillary sinus and nasal passages vary significantly in the degree of cellular differentiation. In general, the poorly differentiated and anaplastic types are more common than the highly keratinizing types (see Fig. 16.4). As the neoplasm becomes more anaplastic, the prickle type cell may take on a spindle shape in some of the higher-grade malignancies. The latter cellular patterns resemble the histologic picture of some sarcomas. The cellular boundaries of these proliferating cells also become less distinct, and mitosis and hyperchromatism are observed, as with all malignancies. Foci of degeneration may appear in the highly undifferentiated tumors, giving them a pseudoglandular appearance.
It might be expected that the more malignant types of squamous cell carcinomas would be the ones that would finally reach the orbit. Among the cases in the Mayo Clinic Series, this was not always so with those tumors from the nasal cavity. Of the 52 carcinomas originating in the maxillary antrum, the malignancy was, in all the 52, either
grade 3 or 4. Of the squamous cell carcinomas arising in the nasal cavity, there was a nearly equal distribution among grade 2, grade 3, and grade 4 anaplastic types.
grade 3 or 4. Of the squamous cell carcinomas arising in the nasal cavity, there was a nearly equal distribution among grade 2, grade 3, and grade 4 anaplastic types.
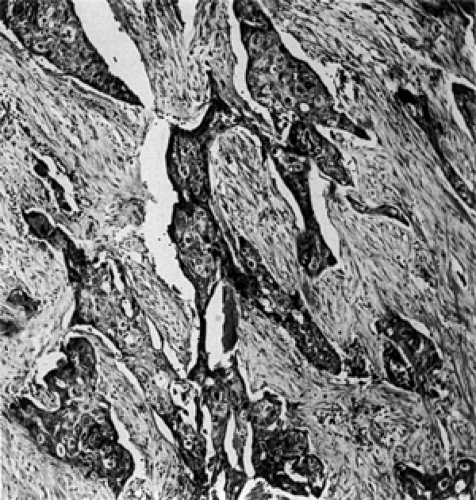 Figure 16.4 Squamous cell carcinoma orbital infiltration by highly anaplastic squamous cells with little evidence of keratin production in a 53-year-old man (× 100). |
The histopathologic features of the secondary neoplasms arising in the skin of the face, eyelids, temple, and eyebrow were similar to those of squamous cell carcinomas elsewhere in the integument (see Fig. 16.5). They were more differentiated tumors and their course was more prolonged than other carcinomas, and only one case had malignancy of grade 4 degree.
Management and Course
The behavior of squamous cell carcinomas with secondary orbital extension is notable for their perversive spread, their refractory response to irradiation, and their high recurrence rate, even with what is considered a major surgical ablation of both soft tissue tumor and the bone involved. In general, prognosis has been related to the degree of malignancy; the more undifferentiated the tumor, the worse the prognosis. These carcinomas possess potentialities for local invasive growth as well as distant metastatic spread. In many tumors of grade 4 showing a malignant degree of undifferentiation, the prognosis is almost hopeless. Prognosis is also influenced to a lesser extent by other factors. With secondary carcinomas arising from the maxillary antrum, for example, the eventual outcome may be influenced by their size and extent at the time of discovery. Some of these carcinomas are not discovered until they have invaded the orbit and by this time they will be almost beyond the boundaries of a radical dissection. For those carcinomas that invade the orbit from adjacent integumentary structures, prognosis may be altered by the completeness of the initial surgical treatment; once the tumor has recurred owing to incomplete excision, the opportunity to eradicate the tumor by subsequent treatment is proportionately limited.
 Figure 16.5 Squamous cell carcinoma. A papillary cell differentiated neoplasm resembling normal epidermis along the floor of the nasal cavity with extension into the area of the lacrimal sac and orbital floor of a 38-year-old man (× 85). |
In the several disorders we have dealt with of this vicious neoplasm, the goal of successful treatment—and possible cure—has been the total surgical eradication of the tumor. With recurrence of the neoplasm, it was evident that incomplete excision was the rule. The culprit in this fallacy probably has been the insidious, unsuspected, extension of the carcinoma by perineural spread (see Fig. 16.6). Even present refinements in imaging methods cannot always detect this spread.
In the 1940s and 1950s, we advised exenteration of the orbit in people showing early stage, orbital invasion. This, sometimes, was considered too harsh. However, later, recurrent tumor would be surgically discovered in the former epicenter of the lesion along the side away from the orbit. A somewhat similar situation evolved when Mohs surgery, several decades ago, became popular for lesions around the face and periorbital adnexae. When a lesion was removed and the margins were negative for carcinoma cells, it was assumed that a complete excision had been performed. Alas! This technique was not infallible. Recurrences were later related to skip foci of cells along the nerve.
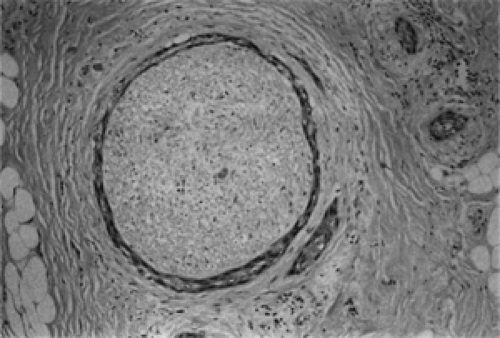 Figure 16.6 Histopathologic section of a branch of the facial nerve surrounded by a thin cuff of squamous cell carcinoma (× 150). (From McNab AA, Francis IC, Benger R, et al. Perineural spread of cutaneous squamous cell carcinoma via the orbit. Clinical features and outcome in 21 cases. Ophthalmology. 1997;104:1457–14620. ) (See Color image.) |
Conclusions
Orbital invasion should be considered an advanced stage of secondary carcinomatous disease.
Most patients die of their disease.
Of the several subgroups studied, those carcinomas arising on the surfaces of the eye, ocular appendages, and eyelids are associated with the smaller percentage of tumor-related deaths. This may be attributed to earlier discovery, easier access of the lesion to ablative surgery, and a lesser degree of histologic anaplasia.
The survival, in years, of patients with tumor-related deaths in the preceding subgroup is about twice that of patients whose carcinomas were primarily in the paranasal sinuses and nasal cavity. However, the percentage of tumor-related mortality in these two subgroups is comparable.
Most secondary orbital carcinomas will have some degree of bone involvement. The full extent of bone destruction may not be radiographically or grossly evident.
Occult bone involvement should be considered in the planning of the extent of surgical resection.
Orbital exenteration combined either with local removal of bone, orbitectomy, maxillectomy, or orbitocranial–facial resection is the present treatment of choice. These management options should be performed by a multidisciplinary surgical team.
No universal controlled study has been performed on a large series of patients regarding the effectiveness of Gamma Knife ablation, adjunctive radiotherapy, or chemotherapy.
In a hypothetical situation of two patients with secondary carcinomas in a similar location with similar extent and the same degree of tumor anaplasia, and equal access of the lesion to surgical removal, the presence or absence of perineural invasion of tumor beyond the margin of surgical removal may be the factor that determines the death of one patient and the survival of the other.
Basal Cell Carcinoma
The eyelids, side of the nose, upper face, and forehead are common sites for orbital, invasive, basal cell carcinomas. Certain features of the skin in these areas—its thin texture, glandular appendages, and exposure to direct sunlight—make it susceptible to these tumors.
A carcinoma in the area of the medial canthus, in particular, is apt to extend into the orbit because of discontinuity of the orbital septum in this area. Also, a surgeon’s reluctance to extirpate the lacrimal drainage system at initial tumor removal may contribute to increased incidence of a secondary orbital extension (Rootman, 1988).
The basal cell carcinomas primarily in the skin of the upper face and periorbital area have often been analyzed in the literature in terms of their frequency, age range, and sex distribution. The tumor is frequently lumped with squamous cell carcinoma in such analysis because the two tumors occur in the same anatomic sites. However, with reference to orbital invasion, a sizable series of basal cell carcinomas are seldom surveyed as a separate subject.
Incidence
In our 50-year tumor survey (see Table 3.3), there are 52 secondary basal cell carcinomas (2.9% of the total 1,795 orbital tumors and 7% of the total 735 secondary orbital tumors). The primary sites of these neoplasms are listed in Table 16.3. Eighty-six percent (45/52) of our patients had recurrent tumor at the time of initial presentation. Often, the duration of symptoms was so long or multiple surgical procedures so numerous that the patients forgot such data. The mean age at the time of presentation was 64 years
(range 28 to 88 years). The male-to-female ratio was 34:18. The right orbit was affected in 31 patients, the left orbit in 19 patients, and 2 patients had bilateral orbital disease.
(range 28 to 88 years). The male-to-female ratio was 34:18. The right orbit was affected in 31 patients, the left orbit in 19 patients, and 2 patients had bilateral orbital disease.
Table 16.3 Site of Origin of Secondary Orbital Basal Cell Carcinomas Mayo Clinic Series (1948 to 1997) (n = 52) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Clinical Features
This type of neoplasm is a master of disguise. In the early stages of growth, the tumor may be a round, elevated, smooth nodule with a shiny surface. In the upper eyelid and eyebrow, it may be warty. Or it may be a sinuous, elongated, superficial, or a lumpy ulceration along the margin of the lower eyelid. Sometimes the tumor is elevated and nodular but with a scaly center surrounded by a rolled border. Lastly, the tumor may be nothing more than an innocent-looking indurated plaque.
However, by the time orbital invasion occurs, these singular aspects tend to merge into an ugly, dirty-looking ulcer with an elevated irregular edge that is covered by a smelly crusted exudate. The surrounding tissues become progressively indurated as the lesion penetrates deeper into the soft tissue. Very advanced lesions may bleed easily, undergo partial necrosis, or show a fistula between the orbital cavity and nose.
The clue to orbital invasion is a fixation of the ulcerated lesion to the underlying rim or surface of the bony orbit. At this stage, the surrounding soft tissues usually show a mild inflammatory response characterized by redness and swelling of tissues or chemosis of adjacent conjunctiva. Pain is not a common accompaniment of early orbital invasion. Only 2 of our 40 cases noted pain at the time of presentation.
Gradually, the tumor becomes rooted to the orbicularis oculi muscle of both the upper and the lower eyelids, the canthal tendons, and the extraocular muscle nearest to the advancing border of the lesion. This results in fixation and immobility of the eyelids and a tethering effect on ocular motility (see Fig. 16.7). Later, the eye becomes immobile and “frozen,” corneal desiccation and perforation occurs, and the vision is lost. Seven of our patients had a visual acuity of hand movements or less in the affected eye at the time of presentation.
Once the neoplasm gains access to the periorbita and soft tissues of the orbital cavity, it tends to expand in a circular fashion in preference to a deeper penetration. Eradication may be possible at this stage provided there is no bone involvement.
Imaging Aspects
The most common areas of early orbital extension, by this neoplasm, are the medial and lateral canthi. A CT scan will show the posterior extent of the soft tissue mass along the inner face of the medial or lateral wall of the orbit, and there may be no bone destruction (see Figs. 16.8 and 16.9). Even so, upon palpation, the anterior orbital rim may have some irregularity indicating minimal bone involvement at this stage. Neuro-imaging is of critical importance in revealing the posterior extent of a recurrent neoplasm that has deeper involvement of orbital tissue. Bone destruction, if present, will also be evident by CT scan. T1 contrast–enhanced, fat-suppressed MRI will show the makeup of the mass and enhancement of the dura if early intracranial expansion is present (Selva et al., 2003).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


