Purpose
To assess the severity of keratoconus at diagnosis and its scalability over a period of 2 years in children compared to adults.
Design
A retrospective monocentric study was conducted in the National Reference Center for Keratoconus, Bordeaux (France), between October 1997 and November 2010.
Methods
In total, 216 patients were studied, comprising 49 patients (22.7%) aged ≤15 and 167 patients (77.3%) aged ≥27 years at diagnosis, who were seen within 2 years of diagnosis. Severity at diagnosis was assessed using Krumeich’s classification, and the scalability criteria of the US Food and Drug Administration (2010) were used. Student t tests and χ 2 tests were performed to compare the 2 groups.
Results
Keratoconus in children was significantly more severe at diagnosis, with 27.8% being stage 4 vs 7.8% of adults ( P < .0001). In addition, ophthalmoscopic signs were more frequent in children (42.9% vs 29.5%, P = .05), while mean values of maximum, average, and minimum keratometry as well as simulated keratometric astigmatism were higher ( P < .0001, P = .0002, P = .0005, and P = .001, respectively). After diagnosis, keratoconus did not evolve more frequently in children. However, in the case of progression, keratoconus evolved faster in children, with significant differences in the spherical equivalent and maximum and minimum keratometry ( P = .03, P = .02, P = .04, respectively).
Conclusion
At diagnosis, keratoconus is often more advanced in children than in adults, with faster disease progression. Early detection and close monitoring are therefore crucial in young patients.
Keratoconus is defined as a bilateral, asymmetric, noninflammatory corneal ectasia. The disease most often occurs at puberty and progresses until the age of about 30 to 40 years before stabilizing. According to published literature and the National Reference Center for Keratoconus (CRNK) in Bordeaux, the average age at diagnosis is 27 years. However, keratoconus may affect younger children, with some studies finding the average age at diagnosis to be less than 20 years. Worldwide, younger patients at diagnosis are frequently from Middle Eastern or Asian backgrounds, and they tend to present severe keratoconus. However, keratoconus patients can be of any background. Keratoconus is a rare cause of amblyopia and visual impairment in children, with figures varying between 0.08% and 12% according to the study and country of origin. As the development of visual function generally continues until the age of 8 to 11 years, amblyopia caused by keratoconus is rare in children.
However, keratoconus is one of the most common causes of corneal transplantation in children, after congenital corneal opacities, with figures in about 15% to 20% of all corneal transplants in children. Young age appears to be associated with more severe forms of keratoconus and faster disease progression, with an inverse correlation between age and severity. In addition, young age at diagnosis is linked to a greater risk of developing corneal opacity and requiring a corneal transplant. However, some studies found no statistically significant relationship between age and scalability of keratoconus.
Early diagnosis in children is interesting because of the development of new therapeutic possibilities. For many years, in the case of failure of contact lenses, penetrating keratoplasty was the only therapeutic option for affected patients. However, over the past decade, various techniques, such as intracorneal rings, corneal collagen cross-linking, lamellar keratoplasty, ring implants or techniques like Keraflex, and customized photorefractive keratectomy, have been developed.
The aim of our study was to assess the severity of keratoconus in children aged ≤15 years at diagnosis compared to adults aged ≥27 years, while examining severity at diagnosis as well as scalability during a 2-year follow-up.
Materials and Methods
Our retrospective monocentric study at the CRNK, Bordeaux, included keratoconus patients diagnosed between October 1, 1997 and November 30, 2010. Overall, 216 patients were studied, including 49 patients (22.7%) aged ≤15 years and 167 patients (77.3%) aged ≥27 years at diagnosis. The ages of 15 and 27 years were chosen because they represent, respectively, the legal age limit for pediatric medical care in France and the mean age of keratoconus diagnosis at CRNK. The criteria for eligibility for the study included diagnosis of keratoconus in children aged ≤15 years and in adults aged ≥27 years, as well as consultation visits within 2 years of diagnosis. In order to evaluate the scalability of keratoconus, the maximum duration of follow-up was 2 years. Exclusion criteria were patients aged between 16 and 26 years at diagnosis, those seen in consultation more than 2 years after the initial diagnosis, and those with a history of ophthalmic surgery, corneal scar, or high myopia (defined as an axial length greater than 26 mm).
At each consultation, clinical and paraclinical tests were performed on both eyes, including a clinical examination using slit-lamp biomicroscopy to detect any anomalies associated with keratoconus (eg, Vogt striae, Fleischer ring, superficial and deep corneal scar, superficial punctate keratitis, or corneal ulceration at the top of the cone), and examination of the dilated fundus. In addition, the following measurements were performed: uncorrected and best-corrected visual acuity (UCVA and BCVA) in logMAR; sphere, cylinder, and spherical equivalent (SE) using the Speedy-K autorefractometer (Nikon; Carl Zeiss Vision, Aalen, Germany); minimum (Kmin), average (AveK), and maximum keratometry (Kmax); corneal topographic astigmatism (SimK astig); anterior and posterior best-fit sphere (BFS) and central corneal thickness and thinnest point using Orbscan II (Bausch & Lomb, Rochester, New York, USA); and corneal hysteresis and corneal resistance factor using Ocular Response Analyzer (Reichert, Depew, New York, USA).
In order to assess the severity of keratoconus at diagnosis, Krumeich’s classification was used ( Table 1 ). Scalability criteria were used according to the 2010 US Food and Drug Administration (FDA) guidelines, which recommended treating progressive ectasia with collagen cross-linking. According to these criteria, keratoconus is considered scalable if 1 of the following 4 criteria was met for a period of less than 2 years: Kmax increase of ≥1 diopter (D), SimK astig increase of ≥1 D, increase in myopic SE of −0.50 D, or decrease in rigid contact lens radius of ≥0.1 mm without further explanation.
| Slit Lamp | Cylinder or Sphere (Diopters) | Maximum Keratometry (Central 3 mm) (Diopters) | Pachymetry (μm) | |
|---|---|---|---|---|
| Stage 1 | Vogt ± Fleischer | <5 | <48 | >500 |
| Stage 2 | Vogt ± Fleischer | 5–8 | 48–53 | 500–400 |
| Stage 3 | Vogt ± Fleischer | >8 | 54–55 | 400–200 |
| Stage 4 | Opacities | Unmeasurable | >55 | <200 |
In order to calculate the patient sample size, the main criterion was the difference in Kmax between the 2 age groups, estimated to be 2.55 D. For each child patient, 2 adult patients were recruited. Accepting an alpha risk of 5% and a statistical power of 80%, the number of subjects required to detect a difference of 2.55 D in Kmax was 141 patients, comprising 47 child and 94 adult patients. Different statistical tests were performed. Data were described using eye as the statistical unit. Qualitative data were described with frequencies and proportions. Distributions of qualitative data were compared between groups using the χ 2 test. Quantitative data were described with means and standard errors of the mean. Distributions of quantitative data in each group were compared using the Student t test. Statistical analyses were performed while taking into account a clustering sampling plan considering the subjects as clusters and eyes as statistical units. For the analysis of scalability, the difference between the initial and the final value of the parameters of interest was calculated for each progressive keratoconus. Student t test was used to compare the means of differences between the 2 age groups. Statistical analyses were performed using SAS software (version 9.2; SAS Institute Inc, Cary, North Carolina, USA). Statistical tests were considered significant when P < .05.
Results
Characteristics of Patients
Most patients were included during a keratoconus consultation, while 12 adult patients (7.2%) were diagnosed during a refractive surgery consultation. The mean age of child patients at diagnosis was 13.1 ± 2.1 years, ranging from 6 to 15 years, while for adult patients it was 37.2 ± 9.1 years, ranging from 27 to 74 years. A male predominance was observed in both age groups, with 75.5% (37/49) of children and 59.3% (99/167) of adults being male ( P = .0.04). The majority of our patients were white: 89.8% (44/49) of children and 85.6% (143/167) of adults.
Severity of Keratoconus at Diagnosis
In total, 432 eyes were studied at diagnosis: 98 eyes in children and 334 eyes in adults.
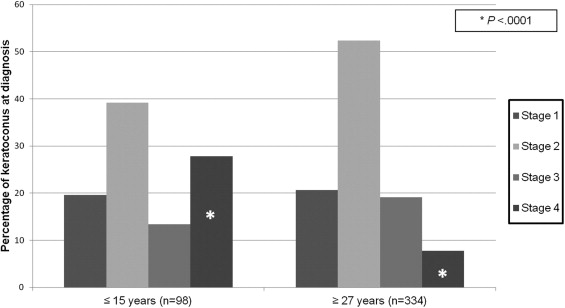
At diagnosis, keratoconus was significantly more severe in children than in adults when assessed using Krumeich’s classification, clinical ophthalmoscopic signs, Kmax, Kmin, AveK, SimK astig, and asymmetry of keratoconus. Children mostly presented keratoconus stages 2 and 4, while adults presented stages 1 and 2 ( Figure 1 ) . In child patients, 27.6% of eyes with keratoconus (27/98 eyes) were stage 4 vs 7.8% (26/334 eyes) in adult patients ( P < .0001), while 42.9% of child patients had ophthalmoscopic signs of keratoconus vs 29.5% of adult patients ( P = .05). The clinical signs most frequently found in both age groups were Fleischer ring and Vogt striae. Fleischer ring was seen in 23.5% of eyes and Vogt striae in 9.5%. Corneal scars (4.0%), superficial punctate keratitis (1.2%), and corneal ulcers (0%) were much less frequently observed at diagnosis. Means of Kmax, Kmin, and AveK were all significantly higher in children at diagnosis compared to adults (respectively 51.32 ± 0.66 D vs 47.98 ± 0.25 D, P < .0001; 46.23 ± 0.53 D vs 44.23 ± 0.20 D, P = .0005; and 47.91 ± 0.55 D vs 45.78 ± 0.18 D, P = .0002). In addition, SimK astig was significantly higher in child patients (4.95 ± 0.33 D vs 3.72 ± 0.18 D; P = .001). The asymmetry of keratoconus was significantly more important in children ( P < .0001), with the mean difference in Kmax being 7.32 ± 0.88 D in children vs 3.25 ± 0.24 D in adults. Other parameters at diagnosis, such as functional ocular signs, best-corrected visual acuity, spherical equivalent, anterior and posterior BFS, central pachymetry, and thinnest point, were also found to be more severe in children, but they did not statistically differ from adults ( Table 2 ). The assessment of corneal biomechanical parameters revealed that corneal hysteresis was significantly higher among children (9.16 ± 0.27 mm Hg vs 8.54 ± 0.14 mm Hg; P = .04). In contrast, there was no significant difference in corneal resistance factor (8.44 ± 0.33 mm Hg vs 8.26 ± 0.17 mm Hg; P = .64). It should be noted that the mean values of corneal hysteresis were higher than those of corneal resistance factor in both age groups. According to Krumeich’s classification, there was no significant difference in the severity of right and left eyes in children ( P = .22) or in adults ( P = .08) (test comparing the distribution of stages 1–2 vs stages 3–4).
| ≤15 Years (98 Eyes of 49 Patients) a | ≥27 Years (334 Eyes of 167 Patients) a | P Value | |
|---|---|---|---|
| Stage 4 | 27 (27.83) | 26 (7.78) | <.0001 |
| Functional signs | 44 (89.80) | 148 (88.62) | .82 |
| Rubbing eyes | 45 (91.84) | 117 (70.06) | .002 |
| Clinical signs | 21 (42.86) | 49 (29.52) | .05 |
| UCVA (logMAR) | 0.59 (0.07) | 0.69 (0.05) | .22 |
| BCVA (logMAR) | 0.31 (0.05) | 0.22 (0.02) | .09 |
| Spherical equivalent (D) | −5.03 (0.48) | −4.21 (0.32) | .16 |
| Kmax (D) | 51.32 (0.66) | 47.98 (0.25) | <.0001 |
| Kmin (D) | 46.23 (0.53) | 44.23 (0.20) | .0005 |
| AveK (D) | 47.91 (0.55) | 45.78 (0.18) | .0002 |
| SimK astig (D) | 4.95 (0.33) | 3.72 (0.18) | .001 |
| Kmax difference between 2 eyes (D) | 7.32 (0.88) | 3.25 (0.24) | <.0001 |
| Anterior BFS (D) | 43.69 (0.35) | 43.45 (0.14) | .53 |
| Posterior BFS (D) | 54.05 (0.38) | 53.37 (0.21) | .12 |
| Central pachymetry (μm) | 481.70 (7.03) | 486.57 (4.15) | .55 |
| Thinnest point (μm) | 454.94 (7.50) | 460.31 (4.56) | .54 |
| CH (mm Hg) | 9.16 (0.27) | 8.54 (0.14) | .04 |
| CRF (mm Hg) | 8.44 (0.33) | 8.26 (0.17) | .64 |
Scalability of Keratoconus in the 2 Years Following Diagnosis
The scalability of 368 keratoconus eyes was analyzed over a maximum period of 2 years, with 86 eyes in 43 child patients and 282 eyes in 141 adult patients. Thirty-two patients were lost to follow-up after the diagnosis.
The proportion of progressive keratoconus in both age groups was not statistically different ( P = .17), affecting 38.4% of keratoconus (33 of 86 eyes) in children vs 30.1% (85 of 282 eyes) in adults.
The FDA criteria used to detect progressive keratoconus were mostly fulfilled between 1 and 2 years after diagnosis, with 78.8% (26 eyes) of progressive cases in children and 86.6% (74 eyes) in adults being observed between 1 and 2 years into follow-up. Twenty-one percent of progressive keratoconus in children (7 eyes) in and 13% of progressive keratoconus in adults (11 eyes) fulfilled at least 1 of the FDA criteria between 1 and 6 months of follow-up. In line with the FDA criteria, in child patients, scalability was defined mainly using Kmax and SimK astig, whereas in adult patients, spherical equivalent was the main criterion. At diagnosis, stage 2 was the most common form of progressive keratoconus, representing 43% of cases in children and 49.4% in adults. Moreover, 24.2% of progressive keratoconus cases in children were stage 4 at diagnosis vs 7.2% in adult patients ( Figure 2 ) . There was no association found between age categories, stage of severity, and scalability ( P = .73). All keratoconus cases, regardless of disease stage and patient age, had the potential to evolve. Regarding progressive disease, no significant difference was found between the number of right eyes and left eyes affected in both children ( P = .27) and adults ( P = .46).
The scalability rate over a maximum period of 2 years was significantly higher in children in terms of spherical equivalent, Kmax, Kmin, and corneal resistance factor. The scalability of spherical equivalent was −0.28 ± 0.26 D in children vs +0.41 ± 0.15 D in adults ( P = .03). The mean of Kmax increased by 1.98 ± 0.59 D in children vs 0.47 ± 0.28 D in adults ( P = .02), while the mean of Kmin increased by +1.02 ± 0.35 D in children vs +0.26 ± 0.14 D in adults ( P = .04). Finally, corneal resistance factor progressed by −0.57 ± 0.18 mm Hg in children vs +0.14 ± 0.17 mm Hg in adults ( P = .007). Other parameters of interest tended to evolve to a greater extent in children than in adults, without the difference reaching significance: SimK astig, posterior BFS, central pachymetry and thinnest point, corneal hysteresis, and corneal radius of curvature of rigid contact lenses fitted in patients ( Table 3 ). In addition, when investigating the scalability of different parameters according to stage using Krumeich’s classification, stage 1 was associated with a significantly greater scalability in children than in adults in terms of Kmax, SimK astig, and spherical equivalent ( P = .008, P = .05, P = .006, respectively).
| ≤15 Years (33 Eyes of 20 Patients), Mean (SEM) | ≥27 Years (85 Eyes of 47 Patients), Mean (SEM) | ||||||
|---|---|---|---|---|---|---|---|
| Initial Value | Final Value | Scalability Average | Initial Value | Final Value | Scalability Average | P Value | |
| UCVA (logMAR) | 0.56 (0.09) | 0.61 (0.11) | −0.03 (0.07) | 0.62 (0.08) | 0.60 (0.08) | −0.04 (0.03) | .87 |
| BCVA (logMAR) | 0.25 (0.06) | 0.25 (0.06) | 0.03 (0.05) | 0.22 (0.04) | 0.16 (0.03) | −0.05 (0.03) | .17 |
| Spherical equivalent (D) | −5.09 (0.62) | −4.92 (0.87) | −0.28 (0.26) | −3.71 (0.62) | −3.51 (0.55) | 0.41 (0.15) | .03 |
| Kmax (D) | 49.85 (0.90) | 51.83 (1.13) | 1.98 (0.59) | 47.91 (0.42) | 48.37 (0.56) | 0.47 (0.28) | .02 |
| Kmin (D) | 45.11 (0.62) | 45.92 (0.68) | 1.02 (0.35) | 43.99 (0.32) | 44.28 (0.37) | 0.26 (0.14) | .04 |
| AveK (D) | 46.96 (0.73) | 47.92 (0.79) | 0.90 (0.33) | 45.67 (0.29) | 45.90 (0.35) | 0.25 (0.13) | .07 |
| SimK astig (D) | 4.19 (0.54) | 5.50 (0.78) | 0.73 (0.23) | 3.71 (0.35) | 3.98 (0.44) | 0.15 (0.22) | .07 |
| Anterior BFS (D) | 44 (0.68) | 43.53 (0.39) | −0.36 (0.65) | 43.54 (0.26) | 43.59 (0.27) | 0.15 (0.07) | .42 |
| Posterior BFS (D) | 53.54 (0.70) | 54.34 (0.53) | 0.23 (0.47) | 53.62 (0.35) | 53.60 (0.42) | 0.14 (0.16) | .86 |
| Central pachymetry (μm) | 490 (9.29) | 494.07 (11.07) | −2.87 (4.48) | 492.13 (7.69) | 498.20 (7.55) | 6.94 (3.23) | .08 |
| Thinnest point (μm) | 463.52 (10.93) | 464 (11.23) | −3.64 (4.21) | 470.53 (8.42) | 466.38 (9.38) | 0.81 (3.77) | .43 |
| CH (mm Hg) | 9.51 (0.34) | 9.26 (0.33) | −0.33 (0.18) | 8.47 (0.18) | 8.46 (0.22) | 0.20 (0.19) | .05 |
| CRF (mm Hg) | 8.94 (0.48) | 8.39 (0.48) | −0.57 (0.18) | 8.11 (0.27) | 7.89 (0.29) | 0.14 (0.17) | .007 |
| Corneal radius of curvature (mm) | 7.30 (0.27) | 7.18 (0.34) | −0.12 (0.13) | 7.52 (0.07) | 7.41 (0.11) | −0.11 (0.07) | .93 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


