Purpose
To compare the risk of capsular rupture of the human lens during cataract surgery from contact by phacoemulsification needles using different vacuum pumps, ultrasound modalities, and contact angles.
Design
Experimental laboratory investigation.
Methods
The John A. Moran Eye Center, University of Utah, Salt Lake City, Utah, was the setting for this study. A Signature (Abbott Medical Optics, Inc) phacoemulsification machine was used in peristaltic and Venturi vacuum modes with transversal and micropulsed ultrasound. Contact was made with a capsular surrogate to achieve tip occlusion or tip contact only. Breakage rates were calculated by analyzing the capsular surrogate under a surgical microscope.
Results
Venturi and peristaltic pump modes had similar risk of capsular rupture, regardless of whether the data were analyzed with tip occlusion data included (44.2% peristaltic vs 40.2% Venturi, P = .047) or excluded from the analysis (66.3% peristaltic vs 60.3% Venturi, P = .013). Transversal ultrasound was significantly more likely to cause capsular rupture than micropulsed ultrasound (69.8% vs 56.8%, P < .0001). Tip contact was significantly more likely than tip occlusion to cause capsular rupture (63.3% vs 0%, P < .0001).
Conclusions
There is no significant difference in risk of capsular rupture using Venturi rather than peristaltic vacuum pumps, while transversal seemed to increase the risk when compared to micropulsed ultrasound. Tip occlusion is not a risk factor for capsular rupture, as all breaks in the capsular surrogate occurred with tip contact.
Many advances have been made in cataract surgery since its advent, especially since the addition of phacoemulsification by Dr Charles Kelman. However, with the addition of this powerful technology came additional opportunities for complications. Posterior capsular rupture is a relatively common complication of cataract extraction via phacoemulsification, with a reported incidence of between 1.7% and 5.2%. Capsular rupture can occur during many different steps of cataract surgery but most frequently occurs during nucleus removal, with approximately 40%–60% of capsular ruptures occurring during this stage. Most likely, this complication is owing to the combination of ultrasound energy and the sharp needle tip. While outcomes after capsular rupture are typically good, there is a definite increase in the incidence of temporarily raised intraocular pressure, persistent uveitis, endophthalmitis, cystoid macular edema, retinal detachment, and retained nuclear material, complications that in some cases necessitate additional surgery. Thus, many advances in phacoemulsification technique and technology have centered on reducing the risk of capsular rupture to increase the safety of the procedure.
Given the wide array of options available to the cataract surgeon regarding types of vacuum pumps, needle specifications, and ultrasound modalities, little data exist comparing the safety profiles of these different options. Recent studies have evaluated optimization of phacoemulsification variables for maximum efficiency of nuclear emulsification and decreased chatter ; however, all of those optimized configurations were found with the machines in peristaltic mode. A recent study by our group showed that Venturi vacuum significantly improved the efficiency of lens fragment removal when compared to peristaltic vacuum. Owing to the inherent differences in vacuum generation and fluid dynamics between peristaltic and Venturi pumps, their safety profiles cannot be assumed to be identical. This study assesses the risk of rupture if the phacoemulsification needle were to inadvertently contact the capsule during cataract surgery, and compares optimized phacoemulsification settings in peristaltic and Venturi mode.
Methods
Design
This study was designed as an experimental laboratory investigation. No human or animal studies were done as part of this investigation.
Previous Work
Our methods and experimental design are a continuation and expansion of work by Meyer and associates. This previous study used peristaltic modes on the Infiniti (Alcon, Inc, Fort Worth, Texas, USA) and Signature (Abbot Medical Optics [AMO], Inc, Santa Ana, California, USA) phacoemulsification machines with a bottle height of 75 cm, machine-indicated flow rate of 60 mL/min, and 550 mm Hg vacuum setting. Their micropulsed ultrasound trials used a WhiteStar handpiece (AMO, Inc) at 2 longitudinal power settings, 10% and 100%, both with a 6 ms on-duty cycle and 12 ms off-duty cycle. Their transversal ultrasound trials used an Ellips handpiece (AMO, Inc) at 100% power and torsional ultrasound trials used an OZil handpiece (Alcon, Inc) at 100% power. For each of these 4 ultrasound modalities, they tested 4 needles: (1) 19 gauge sharp, (2) 19 gauge Dewey Radius (MST, Redmond, Washington, USA), (3) 20 gauge sharp, and (4) 20 gauge Dewey Radius. For each condition, the tip was tapped against the capsule surrogate 200 times. Additionally, they tested 20 fresh human cadaver lenses with exactly the same phacoemulsification parameters. However, owing to the limited number of cadaver lenses, they were limited to the following conditions: (1) micropulsed ultrasound at 100% power with a 6 ms on-duty cycle and 12 ms off-duty cycle with a 20 gauge Dewey Radius needle, (2) transversal ultrasound at 100% power with a 20 gauge sharp needle, (3) transversal ultrasound at 100% power with a 20 gauge Dewey Radius needle, and (4) torsional ultrasound at 100% power with a 20 gauge Dewey Radius needle. The lenses were tapped gently in different places until capsule rupture occurred, rendering the lenses unusable for further trials. They found the rounded edge tip to be very protective of the capsule with all modalities tested.
Capsule Surrogate
Plastic wrap (Great Value Clear Plastic Wrap; Wal-Mart Stores, Inc, Bentonville, Arkansas, USA) was stretched tightly over one end of a closed 4-inch-diameter polyvinylchloride tube as a surrogate for the capsule in the manner previously described by Meyer and associates. The Meyer study used fresh whole human cadaver lenses to further validate this approach. All trials were performed on plastic wrap from the same roll, and pieces of plastic wrap were cut to be large enough to extend beyond the edge of the tube by at least 1 inch in all directions. Tension on the capsule surrogate was established by placing it over the pipe underwater to ensure no air bubbles were trapped underneath, then placing a rubber band around the diameter of the tube to secure it. Once secured in this fashion, to ensure a reasonably uniform tension in all directions, the capsule surrogate was examined for wrinkling, as this would indicate uneven tension. Any wrinkling was resolved by adjusting tension in the appropriate axis of the plastic wrap. This adjustment process was repeated until the entire surface of the capsule surrogate was smoothly uniform. This formed a chamber that was completely filled with water and then submerged in a water bath in order to have a fluid interface on both sides of the capsule surrogate.
Phacoemulsification Settings
The Signature (AMO, Inc) phacoemulsification machine was used with the Fusion cassette (AMO, Inc), with all trials using a 550 mm Hg vacuum setting in both peristaltic and Venturi modes, a bottle height of 50 cm, and balanced salt solution. All trials in peristaltic mode used a flow rate of 40 mL/min. While we do not know the exact fluid flow for Venturi vacuum at 550 mm Hg, in a previous study at 500 mm Hg fluid flow was 102.2 ± 2.3 mL/min for micropulsed longitudinal and 96.6 ± 0.7 mL/min for transversal ultrasound. Micropulsed ultrasound trials used a WhiteStar handpiece (AMO, Inc), while transversal ultrasound trials used an Ellips FX handpiece (AMO, Inc). Micropulsed ultrasound was set at 50% power with a 6 ms on-duty cycle and 6 ms off-cycle. Transversal ultrasound was set at continuous 50% power. Ultrasound and vacuum were both used at only their maximum setting, with all settings on panel control to ensure uniformity. While previous work has shown that micropulsed ultrasound is most efficient at 100% power and transversal at 50% power, we decided the fairest test would be to use the same power setting for both in order to minimize power settings as a confounding factor if there were differing breakage rates.
Phacoemulsification Tips
All trials used phacoemulsification tips with a 30 degree bevel and 0.9 mm (20 gauge) tip diameter. Transversal ultrasound trials were done with a 30 degree bent (Kelman) tip, while micropulsed trials used a straight tip. All tips were made by MicroSurgical Technology (Redmond, Washington, USA). A new tip was used at the beginning of each condition to control for the effect of repeated contact with the capsule surrogate on tip sharpness.
Contact With Capsule Surrogate
In order to distinguish possible differences in safety between peristaltic and Venturi pump modes, 2 techniques for contacting the capsule surrogate simulated different clinical situations. The first technique consisted of tapping the edge of the tip against the plastic wrap by approaching the membrane with the needle bevel up at an angle approximately 30 degrees above parallel to the testing membrane, with no tip occlusion, as indicated in the Figure , Left (tip contact). Ultrasound was engaged during the approach to the surrogate capsule, needle contact, and retraction away from the membrane.
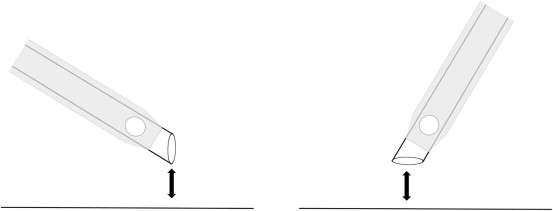
The second technique involved tapping the needle opening at an appropriate angle against the plastic wrap to achieve tip occlusion. To achieve proper and even occlusion, the handle was held such that the bevel of the needle was facing downward with the needle opening parallel to the capsule surrogate as indicated in the Figure , Right (tip occlusion). Ultrasound was engaged during approach to the surrogate and contact and establishment of occlusion; once tip occlusion was indicated by the increasing pitch of audio tones, which signaled increasing vacuum, the pedal was released fully and the tip was simultaneously retracted away from the plastic wrap. The total time of occlusion from initial contact of the needle to release and retraction away from the membrane was approximately 1 second.
In both techniques, contact between the needle and capsule surrogate was monitored under direct visualization, which was aided by placement of a light that would reflect off the membrane, allowing observation of the time and point of contact. Eight conditions were tested: (1) micropulsed ultrasound in peristaltic mode with tip contact; (2) micropulsed ultrasound in peristaltic mode with tip occlusion; (3) transversal ultrasound in peristaltic mode with tip contact; (4) transversal ultrasound in peristaltic mode with tip occlusion; (5) micropulsed ultrasound in Venturi mode with tip contact; (6) micropulsed ultrasound in Venturi mode with tip occlusion; (7) transversal ultrasound in Venturi mode with tip contact; and (8) transversal ultrasound in Venturi mode with tip occlusion. For each occlusion condition, contact was made with the plastic wrap in different places for a total of 200 taps. For each tip contact, contact was made with the plastic wrap in different places for a total of 400 taps. This differential in the number of taps was owing to the considerable difference in breakage rates between tip occlusion and tip contact conditions that we observed in preliminary experiments.
Analysis of Capsule Surrogate
After each run of 200 or 400 taps, the plastic wrap was examined under a microsurgical microscope (Leica Microsystems Inc, Buffalo Grove, Illinois, USA) using a Sinskey hook (Bausch & Lomb Inc, Rochester, New York, USA) to gently probe for breakage. Additionally, in tip occlusion trials we further verified that occlusion had been achieved by observing a full 360 degree outline of the needle in the plastic wrap for each trial.
Statistical Analysis
A χ 2 analysis was used to compare breakage rates between conditions, looking at differences between peristaltic and Venturi modes; between micropulsed and transversal ultrasound; and between tip edge contact and tip occlusion conditions. Results were considered statistically significant at P < .007 after a Bonferroni correction for multiple comparisons.
Results
Seven comparisons were performed on the data set: (1) peristaltic vs Venturi pump modes with occlusion data included, (2) peristaltic vs Venturi pump modes without occlusion data, (3) micropulsed vs transversal ultrasound with occlusion data included, (4) micropulsed vs transversal ultrasound without occlusion data, (5) tip contact vs tip occlusion techniques, (6) tip contact using micropulsed ultrasound in peristaltic vs Venturi pump modes, and (7) tip contact using transversal ultrasound in peristaltic vs Venturi pump modes.
We analyzed the peristaltic vs Venturi pump data and the micropulsed vs transversal ultrasound data twice, including the occlusion data in one comparison and excluding it in another. This is because with the occlusion techniques, in all 800 trials and regardless of ultrasound modality or vacuum pump type, not a single break occurred. Hence, in comparisons where the tip occlusion data were included, the large number of included trials that did not cause any breaks resulted in a smaller percentage difference in breakage rates. Thus, in an effort to unmask possible smaller differences between variables, we analyzed the data both ways.
We found that there was no significant difference in breakage rates between peristaltic and Venturi pump modes. When tip occlusion data were included in this comparison, breakage rates were 44.2% for peristaltic pump mode and 40.2% for Venturi pump mode ( P = .047). When tip occlusion data were excluded from this comparison, breakage rates were 66.3% for peristaltic pump mode and 60.3% for Venturi pump mode ( P = .013). Neither of these comparisons exceeded our corrected level of statistical significance.
We further found that transversal ultrasound was significantly more likely to cause a breakage than micropulsed ultrasound. When tip occlusion data were included in this comparison, breakage rates were 46.5% for transversal ultrasound and 37.8% for micropulsed ultrasound ( P < .0001). When tip occlusion data were excluded from this comparison, breakage rates were 69.8% for transversal ultrasound and 56.8% for micropulsed ultrasound ( P < .0001). Both these comparisons exceeded our corrected level of statistical significance.
As stated above, not a single break occurred in any of our tip occlusion trials, regardless of ultrasound modality or vacuum pump type. Thus, contacting the capsular surrogate with the tip was significantly more likely to cause a breakage than tip occlusion, with a breakage rate of 63.3% for tip contact and 0% for tip occlusion ( P < .0001) ( Table ).
| Conditions | Vacuum Pump Type | Ultrasound Modality | Tip Contact or Occlusion | No. of Trials Performed | No. (%) of Breaks |
|---|---|---|---|---|---|
| 1 | Peristaltic | Micropulsed | Contact | 400 | 246 (61.5%) |
| 2 | Peristaltic | Micropulsed | Occlusion | 200 | 0 |
| 3 | Peristaltic | Transversal | Contact | 400 | 284 (71%) |
| 4 | Peristaltic | Transversal | Occlusion | 200 | 0 |
| 5 | Venturi | Micropulsed | Contact | 400 | 208 (52%) |
| 6 | Venturi | Micropulsed | Occlusion | 200 | 0 |
| 7 | Venturi | Transversal | Contact | 400 | 274 (68.5%) |
| 8 | Venturi | Transversal | Occlusion | 200 | 0 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


