This article reviews the use of robotic technology for otolaryngologic surgery. The authors discuss the development of the technology and its current uses in the operating room. They address procedures such as oropharyngeal transoral robotic surgery (TORS), laryngeal TORS, and thyroidectomy, and also note the role of robotics in teaching.
Robotic technology has been widely used in many nonmedical industries for more than 50 years. However, medical applications in robotics became commonly available only recently. In 1985, the first robotic-assisted procedure was performed, used to accurately localize neurosurgical biopsies. The same device (Puma 560) was then used to perform transurethral biopsies of the prostate. However, despite these advances, the interest in robotics in medicine was still weak. In 1992, the U.S. Food and Drug Administration (FDA) approved the first medical use of a robot. At about the same time, the National Aeronautics and Space Administration and the Department of Defense, recognizing that having a surgeon available on the front lines attending to wounded soldiers during the “golden hour” of trauma would be difficult, began to explore the concept of telepresence battlefield surgery. In theory, a robotic setup could be deployed into frontline battlefield zones, and surgery could be performed remotely on an injured soldier, by a team operating from a safe zone. The Department of Defense, through the Defense Advanced Research Projects Agency, invested significant time and money into this application, which helped boost the general interest in robotics in medicine. This influx of funding and scientific interest finally created enough momentum that the technology began to reach into routine nonmilitary medical applications. This process accelerated the creation of the first commercially available robotic systems, the AESOP (Computer Motion of Santa Barbara, CA, USA) and the da Vinci (Intuitive Surgical, Sunnyvale, CA, USA) systems. Variations of these are still commercially in use today.
The basic concept of telepresence on the battlefield is the premise for the evolving concept of telesurgery, whereby the surgeon performing the operation is not in the same location (or operating room area) as the patient. In general, telesurgery infers a significant distance between the patient and the surgeon, whether this be across town or between states or countries. A major advance of telesurgery is that it brings the expert surgeon to the patient and obviates the need for the patient to travel to the surgeon. This concept of telesurgery, and telemedicine overall, has both national and world health advantages, wherein high-level care could theoretically be provided to underserved areas and populations. Although it seems natural to expand classic robotic surgery as performed today into routine telesurgery, many more complexities exist with respect to the requirements for advanced communications technology and extreme high-speed and dedicated data connections. The feasibility of intercontinental robotic telesurgery was established in 2001 by surgeons in New York performing a cholecystectomy on a patient in Paris. The present hurdles in information management and data transfer over the Internet or dedicated communication portals must be overcome to make telesurgery a reality.
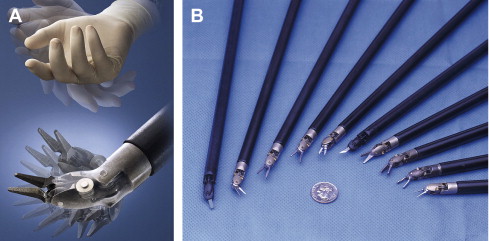
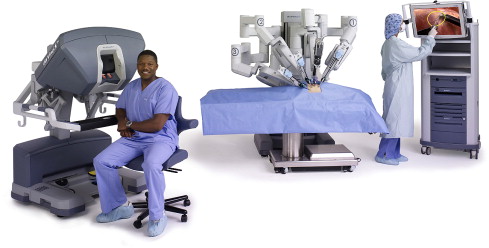
In otolaryngology-head and neck surgery, the primary robotic system in use is the da Vinci system. It consists of a two major components. The first component is the surgeon console, which is a master control where the primary surgeon sits to manipulate the robotic arms. The second component is the robotic cart, which is manipulated remotely by the operating surgeon. The current technology allows the surgeon to manipulate up to three arms with wristed, interchangeable instruments, and one stereoscopic (three-dimensional image) camera, also manipulated from the surgeon console. The robotic instruments, unlike most endoscopic and laparoscopic instruments, are designed to mimic and even exceed the natural range of movement of the surgeon wrists, giving 7° of freedom ( Fig. 1 A and B). With respect to the high-powered optics, the robotic telescope actually incorporates two separate cameras in the distal tip, offset by 15°, giving a true stereoscopic, three-dimensional, high-definition view of the field ( Fig. 2 ). The combination of the wristed movement, distal dexterity, and three-dimensional view are what make this tool well suited for surgery within a confined space ( Fig. 3 ).

In the field of otolaryngology–head and neck surgery, robotics has only a brief history. Initial reports in the literature from the early 2000s described the use of the da Vinci robotic system to help minimize incisions in the neck. The first reported case in a live patient was the excision of a benign vallecular cyst.
Shortly thereafter, Weinstein and colleagues described the first transoral robotic surgery (TORS). The concept was adapted from the evolving use of robotics in the field of urology and cardiac surgery. If the robotic instruments could be placed through small incisions to access the heart or prostate, it seemed reasonable to explore their use in the pharynx and larynx. Furthermore, the trend toward less-invasive and endoscopic procedures in otolaryngology-head and neck surgery led many physicians to explore alternative means of approaching well-established open surgical techniques. Much like endoscopic or laparoscopic surgery, robotic surgery allows surgeons to place instruments into small openings or orifices, allowing distal dexterity that would otherwise be difficult to achieve without large incisions.
Much of the early work in robotics came from the fields of cardiac and urologic surgery. In both of these fields, robotic surgery has now become somewhat routine. In fact, in 2009, more than 85% of men treated surgically for prostate cancer had the surgery performed with robotic assistance. On the heels of the success of robotics in these specialties, other fields of surgical medicine have adopted the use of robotics. Gynecology and bariatric surgery have created several applications for robotic surgery. Other subspecialties are also beginning to consider robotic applications.
The initial preclinical experiments establishing the premise of transoral robotic surgery were performed by O’Malley and Hockstein at the University of Pennsylvania. These early experiments were conducted on human airway mannequins. Building on these original studies, Hockstein and colleagues established a true preclinical research program with both cadaver and live canine experimental models for developing novel robotic surgical techniques and testing the feasibility of robotic surgery as it applies to the field of otolaryngology–head and neck surgery.
One of the first obstacles to overcome in adapting the robotic instruments to the mouth was the laryngoscope. Conventionally, most laryngoscopes have a narrow inlet, and the configuration and size of the robotic arms cannot work within this space. However, several instruments were available and useful to overcome this problem. The Dingman retractor, Crow Davis retractor, and the FK laryngoscope (Gyrus Ent LLC, Bartlett, TN, USA) were some of the early devices used to gain access to the laryngopharynx and allow adequate mobility of the robotic arms for surgery ( Fig. 4 ). Using these retractors, the robotic arms could gain access to the laryngopharynx via the oral cavity. With respect to the cadaver and canine experiments, the original procedures evaluated were vocal cord stripping, partial cordectomy, mucosal flap harvest and inset, tongue base resection, and arytenoidectomy. The authors concluded that this technology may increase the precision of many of these procedures.

After these technical feasibility and discovery studies were completed in cadavers, additional studies were designed and performed to evaluate the safety or to identify risks in using robotic instruments for transoral or head and neck procedures in general. Hemostasis, inadvertent facial and oral injury, and general safety precautions were evaluated. These studies concluded that the safety profile of the robotic-assisted surgical procedures is similar to that of conventional transoral surgery. The combination of technical feasibility and safety established in the preclinical work cleared the way for human trials.
Weinstein and O’Malley established a prospective Institutional Review Board (IRB)–approved human trial at the University of Pennsylvania and conducted the first human experiments for TORS. The original human trials included patients with tonsil, base of tongue, and supraglottic cancers, and a variety of benign tumors and lesions that could be accessed transorally. The trials investigated the safety of the surgery, the optimal instrumentation, and the rate of complications ( Fig. 5 ). Results showed that TORS could be performed in a safe and effective manner, with minimal complications. After the initial surgical trials, further data were collected to show the appropriateness, safety, and efficacy of this procedure. This compiled data were presented to the FDA and, in December 2009, TORS was approved in the United States to treat benign tumors or lesions and selected T1 and T2 malignant tumors in adults. The use of TORS for larger lesions (T3 and T4) is not currently approved by the FDA and merits more investigation.

The TORS operating room setup involves several steps to dock the robot and ensure adequate exposure of the surgical field:
- •
Once the patient is intubated with a reinforced tube, the table is turned away from the anesthesia cart to give the robotic patient cart more room to maneuver.
- •
The appropriate laryngoscope or retractor is placed and suspended.
- •
The endotracheal tube is sewn in place to retract it out of the surgical field and reduce the chance of inadvertent extubation.
- •
The robotic console is brought in from a 30° angle from the patient, and the robotic instruments are introduced into the oral cavity.
- •
The primary surgeon begins at the console, and the bedside surgeon assists by retracting and suctioning at the head of the patient.
Oropharyngeal TORS
Tonsil and base of tongue cancer resections are among the more commonly performed procedures with TORS. Before the advent of TORS, patients with oropharyngeal cancers who were treated surgically often required classic mandibulotomy, tracheostomy, and often free flap or other reconstructions to achieve successful negative-margin surgery. In selected cases, TORS allows these patients the option of completely transoral approach ( Fig. 6 ). In the analysis of the first 27 patients undergoing this approach, the results showed a low incidence of morbidity, with no perioperative mortality. In this series, one patient developed a bleed, and another required a tracheostomy.

To be a candidate for TORS for oropharynx cancer, certain patient and tumor characteristics must be met:
- •
The most obvious is that the tumor must be adequately visualized and exposed for resection.
- •
Characteristics such as trismus, anterior positioned larynx, large tongue, or morbid obesity often make placement of the pharyngeal retractors impossible.
- •
During staging laryngoscopy, the appropriate retractors may need to be inserted to determine if the tumor will be amenable to negative-margin resection with TORS techniques.
The following characteristics are also considered contraindications for TORS :
- •
Unresectability of involved neck nodes
- •
Mandibular invasion
- •
Tongue base involvement requiring resection of greater than 50% of the tongue base
- •
Pharyngeal wall involvement necessitating resection of more than 50% of the posterior pharyngeal wall
- •
Radiologic confirmation of carotid artery involvement
- •
Prevertebral fascia fixation of tumor.
After the resection, a decision is made regarding the need for continued intubation. Many patients with tongue base resections benefit from remaining intubated postoperatively, until the edema created by the surgery has a chance to regress. This process often requires approximately 48 hours. In patients who primarily undergo surgery in the region of the tonsil, this is often not necessary.
Neck dissections are almost always necessary in this population, and most studies have advocated delaying this portion of the surgery for 1 to 4 weeks. The rationale is to reduce the chance of orocutaneous fistula, and to reduce the laryngopharyngeal edema related to both the length of the surgery and the instrumentation in the pharynx and neck concomitantly.
Laryngeal TORS
Before the introduction of TORS, laser microsurgery for select glottic and supraglottic lesions had established itself as a safe and effective means to manage these tumors. TORS takes advantage of many of the characteristics of laser procedures, and adds several others, making it an excellent alternative to laser resections. In addition to oral access to the larynx, TORS affords the operating surgeon excellent distal control of instrumentation and removal of the line of site issues that can occur with the operating microscope, allowing great dexterity in the resection and management of these tumors ( Fig. 7 ).

Much like decision making in oropharynx lesions, choosing appropriate candidates for this surgery is critical. Not only is it important to confirm that the tumor can be adequately resected via this approach but also the operating surgeon must feel that surgery will produce the best functional outcome (relative to nonsurgical approaches).
Not surprisingly, these patients have a slightly higher rate of temporary tracheostomy in the combination of trials performed in the literature. Furthermore, the rate of dysphagia seems slightly higher in patients undergoing laryngeal TORS compared with oropharyngeal TORS.
The instrumentation to perform laryngeal microsurgery is still being designed. Despite the excellent visibility and dexterity of the robotic arms, the lack of fine instrumentation and the limitations imposed by the relatively large robotic arms and camera still pose a challenge for managing many of the tumors below the level of the supraglottis.
Robotic Thyroidectomy
Transaxillary robotic thyroidectomy is another application of robotics in the field of otolaryngology–head and neck surgery. Although this technique evolved from attempts to reduce or eliminate the cervical incisions that have generally been the hallmark of thyroid surgery for more than 100 years, it may ultimately allow surgeons to become facile with endoscopic neck surgery. Although TORS eliminates the incisions related to resection of the primary, many of these patients still require an open neck dissection. Researchers have postulated that mastery of these techniques, initially through thyroid surgery, will ultimately allow head and neck cancer to be managed entirely via an endoscopic approach.
Over the years, thyroidectomy incisions have become smaller in selected patients. The application of endoscopes has allowed for video-assisted thyroid surgery. Several authors described various approaches to the thyroid using incisions hidden from view, including inframammary, areolar, and even transoral approaches to the thyroid gland, typically using carbon dioxide (CO 2 ) insufflation to maintain a working space. An endoscopic transaxillary approach to this region had been developed both with and without CO 2 insufflation. After a significant experience with the endoscopic approach, robotic technology was applied ( Fig. 8 ).

One of the pioneers of the robotic transaxillary approach to the thyroid is Dr Chung at Yonsei hospital in Korea. He has performed and reported on more than 500 robotic thyroid cases, with excellent results. More recently, this surgery gained popularity in the United States, and several studies have been designed to evaluate its feasibility and safety.
Generally, the robotic transaxillary approach to the thyroid involves creating a surgical working space.
- •
The space is maintained with a retractor instead of insufflation.
- •
A plane is created from the axilla, over the pectoralis muscle, and the heads of the sternocleidomastoid muscle are separated.
- •
The strap muscles are retracted anteriorly–anteriorly, allowing access to the lateral aspect of the thyroid bed.
- •
The robotic instruments are then brought into the field and the thyroid is removed.
- •
The contralateral lobe is removed through dissecting over the trachea and taking a medial-to-lateral approach to the gland.
The obvious benefit of the robotic approach to the thyroid through the axilla is the lack of a neck incision. In addition, possible added benefits relate to magnified stereoscopic visualization and improved dexterity. These benefits must be shown through comparative trials. Additionally, potential complications that do not typically occur during traditional thyroid surgery must be considered because of the lateral approach, including injury to the carotid artery, jugular vein, and esophagus.
The Role of Robotics in Teaching
Robotics lends itself easily to serving as a teaching tool. Even as an observer of the procedure, the visualization is excellent. With the exception of the stereoscopic view, observers are seeing the same field as the surgeon. Additionally, some centers are equipped with three-dimensional observation screens to provide a more realistic view for observers.
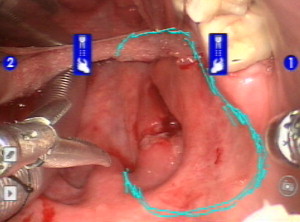
Another useful tool that serves as a teaching aid for robotic surgery with the da Vinci robot is the telestration capacity ( Fig. 9 ). Although the surgical student sits at the console, the teacher can use one of the real-time monitors to draw and illustrate in a manner that be seen by the physician at the console. This technique allows a hands-on approach by the teacher, even while the student is at the console.