Robotic Modified Radical Neck Dissection for Thyroid Cancer; Surgical Technique Using Gasless, Transaxillary Approach
Sang-Wook Kang
INTRODUCTION
The higher socioeconomic status enjoyed today has resulted in quality of life being viewed as a major issue. This trend has greatly influenced medical disciplines, and many medical and surgical therapies have been modified based on quality of life considerations. Accordingly, minimally invasive surgery in various surgical fields has rapidly developed and spread due to increased concerns about issues, such as incision scars, degree of pain, and time required to return to work after surgery.
In the head and neck area, well-differentiated thyroid carcinoma (WDTC) is the most common malignancy and, unlike other cancers of the head and neck, usually has a favorable prognosis. Furthermore, the incidence of early-stage cancer of the thyroid has markedly increased due to the institution of various health-screening programs, and the proportion of thyroid cancer in young women, who are particularly sensitive to cosmesis, is increasing. Accordingly, trials on endoscopic or minimally invasive techniques in thyroid surgery have been continuously conducted with a main aim of avoiding visible scars on the neck, and many early satisfactory results have already been reported for these techniques.
Papillary carcinoma of the thyroid (PTC)—the most common type of WDTC—usually has a mild biologic course, but nevertheless, it frequently metastasizes to the cervical lymph nodes (LNs). In cases of metastasis to the lateral neck nodes (LNM) from PTC, bilateral total thyroidectomy with modified radical neck dissection (MRND) for metastatic lateral cervical nodes is the treatment of choice. However, although conventional open MRND is the safest and most efficient type of surgical treatment, a desperately long incision scar on the neck is inevitable. In view of the favorable nature and high prevalence of PTC in women, the avoidance of unsightly scarring in the neck area necessitates minimally invasive and remote approaches to lateral neck dissection. Accordingly, I have applied endoscopic techniques to thyroidectomy and MRND procedures for PTC with LNM. Furthermore, the incorporation of dexterous robotic technology in surgery of the neck enables more precise and meticulous endoscopic movement during the complex procedure required for MRND. Recently, a robotic MRND technique for cancer of the thyroid with LNM was introduced and produces excellent cosmetic results. In addition, the technical feasibility and safety of robotic MRND have been reported, and the technique has been found to be capable of complete compartment-oriented dissection.
In the early 20th century, George Washington Crile first described a systematic surgical approach to en bloc neck dissection for cancers of the head and neck, and subsequently, Martin and his colleagues refined Crile’s original methods and substantially expanded the concept of radical neck dissection to its current format. Later many surgeons, including Suárez, Bocca, and Gavilán, attempted to modify, standardize, or establish the surgical extent of neck dissection. During the 1960s, surgeons at the MD Anderson Hospital (Jesse, Ballantyne, and Byers) began to selectively remove, based on location of the primary lesion, only the neck LN groups at highest risk of metastasis.
Recently, profound comprehension of the pathophysiology of cancers of the head and neck and intensive treatment experience resulted in alternative surgical options for cervical LN metastasis, such as selective or
superselective neck dissection in accordance with primary tumor biology to reduce surgical morbidity while preserving oncologic safety.
superselective neck dissection in accordance with primary tumor biology to reduce surgical morbidity while preserving oncologic safety.
In carcinoma of the thyroid, MRND type III (actually, selective neck dissection [levels II-VI]) is the current treatment of choice for the management of WDTC with LNM. In this chapter, I will describe in detail robotic MRND methods for the management of WDTC with LMN.
HISTORY
The patient should be questioned about a history of dysphagia, weight loss, or skin cancer removed in the past, or a persistent sore area in the upper aerodigestive tract. Also it is important to inquire about hoarseness, dysphagia, or weight loss. Question whether the patient has had other cancers, such as lung, breast, intra-abdominal, or prostate in addition to thyroid cancer. These cancers can spread via lymphatics and usually go to the left supraclavicular LNs.
PHYSICAL EXAMINATION
A complete examination of the head and neck should be performed. The location of the enlarged nodes can often guide you to the primary cancer. It is important to check the thyroid gland for nodules.
The size, number, and mobility of the LNs are important. It is also critical to note fixation to the skin, or underlying structures which may be a contraindication to this procedure.
INDICATIONS
The eligibility criteria for robotic MRND are as follows: (1) WDTC with clinical LNM (cases with a minimum of 1 or 2 metastatic LNs in the lateral neck), (2) a primary tumor size of ≤4 cm, and (3) minimal invasion of the anterior thyroid capsule and strap muscles by the primary cancer.
The role of the robotic procedure for the management of cancer of the thyroid with LMN remains controversial. For experienced surgeons, this approach may be well suited for cases with limited LNM from WDTC, but its role in cases of more locally advanced cancer is uncertain, and thus, robotic MRND is clearly contraindicated in such cases.
The exclusion criteria that should be applied are (1) definite tumor invasion to an adjacent organ (recurrent laryngeal nerve, esophagus, major vessels, or trachea), (2) multiple LN metastases in multiple levels of the lateral neck, or (3) perinodal infiltration at a metastatic LN.
CONTRAINDICATIONS
1. Life expectancy of <3 months
2. Uncontrollable cancer at the primary site
3. Fixed LNs unchanged by irradiation and/or chemotherapy
4. Surgeon who is inexperienced with robotic surgery and open MRND
PREOPERATIVE PLANNING
WDTC should be diagnosed in all patients by preoperative fine-needle aspiration biopsy (FNAB). High-resolution staging ultrasonography (US) and computed tomography of the neck can be performed for preoperative staging of the disease. All patients with clinically palpable lateral neck nodes or a lateral LN with a suspicious ultrasound appearance by preoperative staging US should undergo US-guided FNAB.
The presence of metastasis to a lateral neck node can be determined by US-guided FNAB histology or by measuring thyroglobulin (Tg) levels in FNAB washout fluid (FNA-Tg > 10 ng/mL, >mean + 2 SD of FNA-Tg measured in node-negative patients, or >serum-Tg) from lateral neck LNs.
Extent of Dissection for Modified Radical Neck Dissection
The optimal management of PTC remains the subject of considerable debate. Nevertheless, the most important initial consideration is the complete surgical resection of the cancer of the thyroid and metastatic LNs. Radioactive iodine treatment can be administered later for ablation of any remaining thyroid tissue, and TSH suppression
therapy can be added according to risk. The surgical extent of PTC can be classified using the two LN-bearing compartments to which PTC usually metastasizes, that is, the central and lateral compartments. Routine prophylactic lateral neck dissection in PTC patients is controversial, because lateral neck areas may be treatable by second surgery. However, therapeutic lateral neck dissection in PTC patients with clinically determined LMN is always necessary.
therapy can be added according to risk. The surgical extent of PTC can be classified using the two LN-bearing compartments to which PTC usually metastasizes, that is, the central and lateral compartments. Routine prophylactic lateral neck dissection in PTC patients is controversial, because lateral neck areas may be treatable by second surgery. However, therapeutic lateral neck dissection in PTC patients with clinically determined LMN is always necessary.
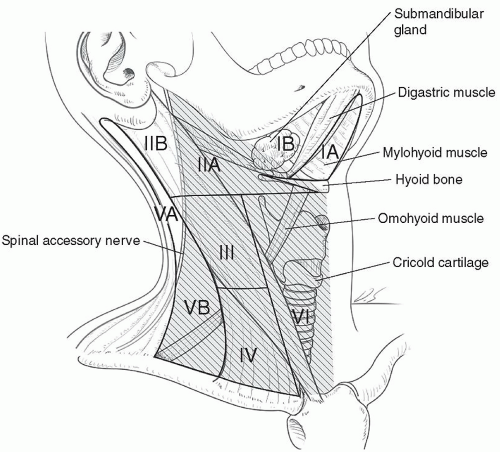 FIGURE 5.1 The anatomic landmarks used to divide the lateral and central LN compartments into levels I-VI; the area with a deviant crease line is where LN dissection is made during MRND. |
The surgical approaches used most commonly in cases with LNM from PTC are bilateral total thyroidectomy with central compartment neck dissection and concurrent MRND (type III, sparing sternocleidomastoid muscle [SCM], spinal accessory nerve, and the internal jugular vein [IJV]). The submental, submandibular, parotid, and retroauricular nodes are virtually never dissected, and level IIB and VA lymph nodes are not routinely dissected either in cancer of the thyroid with LNM, because its rarely metastasizes to levels I or IIB, or VA.
However, if an enlarged or suspicious cervical LN is encountered by palpation or by preoperative US in these areas, these compartments are also included in en bloc dissection. Thus, the usual extent of surgical dissection for MRND in WDTC with LNM are levels IIA, III, IV, VB, and VI, which applies to robotic and open MRND procedures (Fig. 5.1).
SURGICAL TECHNIQUE
Patient Preparation
With a patient in a supine position under general anesthesia, the neck is slightly extended by inserting a soft pillow under the shoulder and turning the face away from the lesion. The lesion-side arm is stretched out laterally and abducted about 80 degrees from the body (Optimally expose the axillary and lateral neck areas). The landmarks for dissection are the sternal notch and the midline of the anterior neck medially, the anterior border of trapezius muscle laterally, and the submandibular gland superiorly (Fig. 5.2).
Development of Working Space
A 7- to 8-cm vertical skin incision is placed in the axilla along the anterior axillary fold and the lateral border of the pectoralis major. A subcutaneous skin flap is made over the anterior surface of the pectoralis muscle from axilla to the clavicle and the sternal notch. After crossing the clavicle, a subplatysmal skin flap is made. The flap is dissected medially over the SCM muscle toward the midline of the anterior neck. Laterally, the trapezius muscle is identified and dissected upward along its anterior border. The spinal accessory nerve is identified and traced carefully along its course until it passes on the undersurface of the SCM muscle. The subplatysmal skin flap is elevated upward to Erbs point, and after exposure of this landmark, the dissection proceeds deep to the




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
