This article introduces and evaluates the feasibility of robot-assisted neck dissection as well as robot-assisted neck surgery via a modified facelift or retroauricular approach. Robot-assisted neck surgery is feasible compared with conventional techniques and shows a clear cosmetic benefit.
Key points
- •
Neck dissection (ND) is performed for patients with head and neck squamous cell carcinoma and results in improved regional disease control as well as disease-specific survival.
- •
When performed through a conventional transcervical approach, ND leaves a visible scar on the neck, regardless of the size of the incision.
- •
In the past, a scar on the neck has been accepted as unavoidable.
- •
This article introduces our surgical technique to perform a standard ND while transposing the external scar by using the robotic system via a modified facelift or retroauricular approach.
Overview
Conventional head and neck surgery for neck dissection (ND) as well as for benign tumors is performed via transcervical incision. However, this conventional approach leaves a prominent scar on the neck, regardless of size. Considering the usual young age of patients with benign neck masses, easily visible scars might have a greater psychological impact on the patients than physicians assume, especially in young women. Therefore, in recent years, innovations in surgical technique have provided several new approaches to hide visible scars by modifying the surgical techniques and using remote access. Such efforts have resulted in endoscopic thyroidectomy techniques, and we previously reported our experience of a unilateral axillobreast approach. Clinical trials to make scars invisible have extended to other benign cervical lesions, and several investigators have reported the resection of the submandibular gland (SMG) or branchial cleft cyst using the retroauricular (RA) approach with or without an endoscope. The retroauricular, or facelift, approach showed good cosmetic effects because the scar was hidden behind the auricle and hair. We recently applied robotics to benign cervical lesions. We reported the feasibility of robot-assisted SMG resection and the Sistrunk operation via an RA approach.
Since the advent of surgical robotics a few years ago, transoral robotic surgery (TORS) has been actively applied worldwide in head and neck cancer surgery. Furthermore, various endoscope-assisted or robot-assisted minimally invasive approaches have been developed and applied to head and neck diseases. Since 2010, our institution has reported the feasibility of robot-assisted ND (RAND) for patients with cN+ necks as well as cN0 necks. At first, RAND was performed via the transaxillary and retroauricular (TARA) approach to remove cervical lymphatics from levels I to V. However, through accumulation of surgical experience of RAND, we realized that the operation can be conducted with no difficulty through the RA or modified facelift (MFL) approaches only. Hence, the RA or MFL approach is now considered sufficient when performing RAND in head and neck cancers. This article presents our novel surgical technique of RAND as well as benign neck mass excision via RA or MFL incisions.
Overview
Conventional head and neck surgery for neck dissection (ND) as well as for benign tumors is performed via transcervical incision. However, this conventional approach leaves a prominent scar on the neck, regardless of size. Considering the usual young age of patients with benign neck masses, easily visible scars might have a greater psychological impact on the patients than physicians assume, especially in young women. Therefore, in recent years, innovations in surgical technique have provided several new approaches to hide visible scars by modifying the surgical techniques and using remote access. Such efforts have resulted in endoscopic thyroidectomy techniques, and we previously reported our experience of a unilateral axillobreast approach. Clinical trials to make scars invisible have extended to other benign cervical lesions, and several investigators have reported the resection of the submandibular gland (SMG) or branchial cleft cyst using the retroauricular (RA) approach with or without an endoscope. The retroauricular, or facelift, approach showed good cosmetic effects because the scar was hidden behind the auricle and hair. We recently applied robotics to benign cervical lesions. We reported the feasibility of robot-assisted SMG resection and the Sistrunk operation via an RA approach.
Since the advent of surgical robotics a few years ago, transoral robotic surgery (TORS) has been actively applied worldwide in head and neck cancer surgery. Furthermore, various endoscope-assisted or robot-assisted minimally invasive approaches have been developed and applied to head and neck diseases. Since 2010, our institution has reported the feasibility of robot-assisted ND (RAND) for patients with cN+ necks as well as cN0 necks. At first, RAND was performed via the transaxillary and retroauricular (TARA) approach to remove cervical lymphatics from levels I to V. However, through accumulation of surgical experience of RAND, we realized that the operation can be conducted with no difficulty through the RA or modified facelift (MFL) approaches only. Hence, the RA or MFL approach is now considered sufficient when performing RAND in head and neck cancers. This article presents our novel surgical technique of RAND as well as benign neck mass excision via RA or MFL incisions.
Treatment goals
The authors’ hypothesis is that this procedure can produce better cosmetic satisfaction without significant surgical morbidity, but maintain the same quality and standards as in the conventional approach to ND. First and foremost, the procedure should guarantee complete removal of the lesion with acceptable feasibility compared with the conventional external approach. Next, such an approach might also provide patients with better cosmetic results after surgery. The RA approach can be a representative technique to study remote access to the neck, camouflaging the scar in the retroauricular hairline.
Although complications after conventional ND (CND) are uncommon, RAND may improve postoperative cervical wound problems such as fibrotic band formation and wound dehiscence, which are occasionally encountered in a cervical incision. If there is any skin dehiscence, the risk of great vessel exposure leading to fatal bleeding is low, as can be anticipated in conventional transcervical wounds. In addition, postoperative lymphedema can be avoided and the chance of developing wound healing problems after radiotherapy is less because the skin incision site is located far from the radiation field and normal lymphatic drainage are not disturbed. Most advantages of RAND rest on the incision being remotely placed. Considering the area of dissection, it is not more invasive than the traditional transcervical ND. The robotic system merely helps the surgeon to dissect the lymphatic tissue where access is troublesome. A considerable portion of RAND is performed under the gross vision (levels IIa, IIb, III, and Va). From the results of the present study, the numbers of lymph nodes retrieved for each type of RAND were comparable with its conventional counterpart. The combined treatment using TORS and RAND can be of maximal benefit to the patient in terms of cosmesis and postoperative function.
Preoperative planning and special equipment
Patient Selection
The body mass index (BMI [kg/m 2 ]) and length and circumference of the neck should be considered because they may affect the difficulty and duration of the procedure. There is no absolute contraindication regarding the body habitus or BMI. With more than 100 cases of RAND, we could successfully accomplish the planned procedures without conversion to the CND regardless of BMI. Obesity is not an absolute contraindication to the surgery, but the possible prolongation of operation time should be explained to the patient. Because RAND requires longer operation time than the conventional technique, patients in old age or with comorbidities should be carefully selected.
Every patient should be informed about the procedure, including both the advantages and the disadvantages of RAND and all other options, including CND, and chemoradiotherapy should be suggested. Informed consent should include this, elucidating the possibility of conversion to CND.
Precautions for Anesthesia
For flap elevation and upper ND under direct vision, the operator should be seated near the head of the patient looking cephalocaudally. The endotracheal tube should be directed to the contralateral side and connected to the ventilator, which is located near the patient’s feet, 180° from the typical setup. Risks of any other anesthesia-related complications or difficulties for intubation and anesthesia are not specifically increased with this procedure. The airway is not naturally compromised or disturbed in any way through this procedure.
Special Equipment
- 1.
Retractors for skin flap elevation
- •
Skin hook.
- •
Army-Navy retractor.
- •
Right-angle breast retractor.
- •
Self-retaining retractor (Sangdosa Inc, Seoul) ( Fig. 1 ).
Fig. 1
Self-retaining retractor and Yankauer suction. ( A ) The 2 retractors on the left are Chung retractors used for endoscopic or robotic thyroidectomy and the 4 on the right are self-developed retractors for ND via retroauricular approach or modified facelift incision. ( B ) New self-developed Yankauer suction with long or short length.
( Courtesy of Sangdosa Inc, Seoul, South Korea; with permission.)
- •
- 2.
Instruments for dissection under direct vision
- •
Monopolar cautery tips with variable length (spatula tip is preferred).
- •
Harmonic curved shears (Harmonic Ace 23E; Ethicon Endo-Surgery, Cincinnati, OH).
- •
DeBakey forceps or Russian forceps.
- •
Yankauer suction (see Fig. 1 ).
- •
- 3.
Robotic instrument (da Vinci Robotic System, Intuitive Surgical Inc, Sunnyvale, CA)
- •
Twelve-millimeter, 30° face-down endoscope (Intuitive Surgical Inc, Sunnyvale, CA).
- •
Five-millimeter, Maryland forceps (Intuitive Surgical Inc, Sunnyvale, CA).
- •
Five-millimeter, Harmonic curved shears (Intuitive Surgical Inc, Sunnyvale, CA).
- •
Eight-millimeter, ProGrasp forceps (Intuitive Surgical Inc, Sunnyvale, CA): installed at left or right arm depending on the side of ND. It could be substituted by an endoscopic alligator forceps manipulated by a patient-side assistant.
- •
- 4.
Vessel ligation system
- •
Hem-o-lok Ligation System (Teleflex Inc, Research Triangle Park, NC).
- •
Patient and robot positioning
Positioning of the Patient
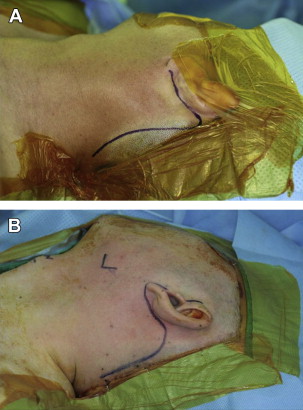
The patient is set in a supine position with the neck slightly extended by inserting a soft pillow under the shoulder and with the head rotated toward the contralateral side ( Fig. 2 ). The neck is sometimes relaxed in its natural position and not extended.
Positioning of the Robot
After sufficient working space is acquired and upper ND under direct vision is complete, the robotic system is introduced. After placing the foot end of the surgical bed 180° from the anesthesia team, the patient is placed in a supine position, and the manipulator cart and surgical bed are located 30° from the head on each side. A face-down 30° endoscope is used for visualization of the surgical field and 2 robotic instrument arms, equipped at either side of the endoscopic arm with 5-mm Maryland forceps and 5-mm Harmonic curved shears respectively, are used throughout the operation ( Fig. 3 ). A patient-side assistant can facilitate the robotic dissection by exposing the surgical field using an Army-Navy retractor or Yankauer suction.
Procedure
Robot-assisted Neurogenic Tumor Excision
The patient is placed in the supine position, the neck is extended, and the head is rotated to the contralateral side. A skin incision is made behind the auricle starting from the lower end of the retroauricular sulcus, moved upward to the midpoint of the sulcus, and then smoothly angulated downward 0.5 cm inside the hairline. Care should be taken to avoid damaging the hair follicles during the skin incision and subcutaneous dissection. The subplatysmal skin flap is elevated just above the sternocleidomastoid muscle and carried in an anterior and inferior direction using a monopolar coagulator under direct vision. Special attention is paid to preserve the great auricular nerve and other sensory nerves. When the mass is fully exposed, a self-retaining retractor is introduced, and the skin flap is raised using a lifting device to create a working space ( Fig. 4 ).

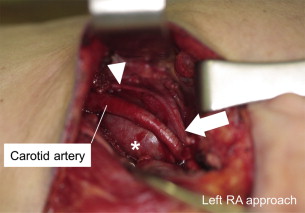
The da Vinci S Robotic System (Intuitive Surgical Inc, Sunnyvale, CA) is deployed, with a 30°-down dual endoscope in the center, a Maryland forceps in the nondominant hand, and a Metzenbaum scissors (PK Dissecting Forceps) in the dominant hand of the robotic arm. If needed, ProGrasp forceps (Intuitive Surgical) may be installed to enhance the dissection of tumor. Careful enucleation of schwannoma should be done by dissection of the carotid space between the carotid artery and the internal jugular vein (IJV) with dissecting forceps without neural damage under magnification. Attention should be paid to prevent the injury to the jugular vein, the carotid artery, and other nervous systems. Figs. 5 and 6 show this technique used for a neurogenic tumor, which should be identified and dissected to preserve the neural function.
Robot-assisted SMG Excision
The procedure for robotic dissection of SMG is similar to that for endoscopic SMG excision but the instrumentation of the robotic system makes the dissection more convenient. The 30° dual-channel endoscope provides a three-dimensional magnified view and the highly articulated wrist and 360° motion of the robotic arm controlled by the surgeons facilitates the dissection. Dissection begins at the lower border of the SMG. Dissection is conducted using a Harmonic curved shears or a monopolar cautery according to the surgeons preference. The Maryland dissector controlled by the surgeon and a Yankauer suction handled by a bedside assistant provides traction and countertraction, which facilitates the dissection between the SMG and surrounding tissues. Compared with the 2 arms of endoscopic dissection for traction and dissection, robotic dissection provides 4 hands at most (2 robotic arms and the 2 arms of the bedside assistant). The bedside assistant can use the Yankauer suction, endoscopic dissector, or an Army-Navy retractor to aid the surgical exposure and dissection. Traction and countertraction in robotic dissection not only facilitate the dissection of the SMG but also may prevent injury to the gland or the tumor, which may occur during dissection with excessive traction only. The proximal facial artery is ligated with the Harmonic curved shears or vascular clips, as is done with endoscopic dissection ( Fig. 7 A). The lingual nerve is separated from the submandibular ganglion with monopolar cautery or the Harmonic curved shears (see Fig. 7 B), and the Wharton duct is ligated with a vascular clip or a Harmonic curved shears (see Fig. 7 C). The lingual nerve and hypoglossal nerve are well preserved, and dissection should be performed closely attached to the surface of the gland to prevent thermal injury to these structures (see Fig. 7 D). The capsule of the intraglandular mass is carefully preserved to prevent tumor spillage.
Robot-assisted Excision of a Thyroglossal Duct Cyst (Sistrunk Operation)
After flap elevation through the retroauricular incision in the plane of the subplatysmal layer, the cystic lesion is identified beneath the superficial layer of the strap muscles. The fibrofatty tissue at the anterior neck is divided using a 5-mm Maryland forceps and 5-mm spatula monopolar cautery for midline identification. The cystic lesion is carefully dissected away from the surrounding fibroconnective tissue and muscle. After identifying the left great horn of the hyoid bone, the tumor is carefully dissected from the surrounding tissue and mobilized ( Fig. 8 A). Following the skeletonization of the ipsilateral hyoid bone, a bone cutter is introduced through the retroauricular port and the ipsilateral hyoid bone is resected by an assistant (see Fig. 8 B). After that, infrahyoid muscles together with fibroconnective tissue is dissected and freed from the mass (see Fig. 8 C). Further extension of the thyroglossal duct should be checked beyond the hyoid bone. Further dissection is then done to the contralateral side using monopolar cautery and the contralateral side of the hyoid bone is cut as well (see Fig. 8 D). In addition, careful dissection should be done to remove the main mass together with the resected hyoid bone.
Robot-assisted Selective ND (Level I–III)
Skin incision design
An MFL or RA incision is designed according to the surgical extent and types of surgery. The RA incision is made behind the auricle starting from the lower end of the retroauricular sulcus and moving upward to the midpoint of the sulcus, and then smoothly angulated downward 0.5 cm inside the hairline (see Fig. 2 A). An MFL incision is extended from the RA incision to the natural preauricular fold and continued behind the tragus (see Fig. 2 B). At first, the MFL approach was mostly chosen because it provided a wider and higher working space for the robotic instrument arms than the RA approach. However, as our experience with RAND increased, we realized that the RA approach could create a sufficient working space for robotic arms without preauricular incision. The RA approach is now mainly used for RAND.
Skin flap elevation
A subplatysmal skin flap is elevated just above the sternocleidomastoid (SCM) muscle using monopolar cautery under direct vision and is continued to the midline of the anterior neck, superiorly to the inferior margin of the mandible, and inferiorly to the level of omohyoid muscle. Two assistants pull the skin flap with the Army-Navy retractor or right-angle breast retractor. The greater auricular nerve and external jugular vein should be preserved superficial to the SCM muscle ( Fig. 9 ). Skin flap elevation below the mandible should be conducted with care not to give thermal injury to the marginal branch of the facial nerve. After identifying the contour of the SMG, the lateral border of the strap muscles should be identified medially and the superior belly of the omohyoid muscle should be identified inferiorly. When sufficient working space is acquired, a self-retaining retractor is applied.



