Over the past 10 years, there has been increasing recognition of the interaction between the upper and lower airways in patients with a variety of infectious and inflammatory illnesses, including allergic rhinitis, rhinosinusitis, and asthma. Epidemiologic and mechanistic links have been proposed to demonstrate these relationships and to offer possible etiologic explanations to account for these observations. Among patients with upper respiratory illnesses, cough can be seen as a common symptom, both from the direct influences of upper airway inflammation, which incite reflex changes and bronchospasm, and from the exacerbation of associated pulmonary processes, such as asthma. Despite this increasing awareness of interaction between the upper and lower airways, the influence of both upstream and downstream respiratory inflammatory processes on laryngeal pathophysiology has not been extensively studied. Research suggests, however, that both direct stimulatory effects on the larynx and secondary effects of mucus production and mucus trafficking can create a range of laryngeal symptoms, including cough. This review discusses the interaction of the upper and lower airway in respiratory disease, and focuses on the effect of these respiratory processes on laryngeal inflammation, function, and symptoms.
Extensive epidemiologic and physiologic data gathered in the past decade suggest that the respiratory tract, from the eustachian tube and the paranasal sinuses through to the distal bronchioles, functions as a unified, organized, and interrelated unit. Both local inflammatory processes and the systemic propagation of inflammation through trafficking of inflammatory mediators promote a system-wide response in the respiratory mucosa through which pathology in one portion of this system can stimulate and influence pathophysiological changes at a site distal to the initial site of inflammation. The model developed to study and explain these observations has been termed the unified airway model and has been recently described:
The presence and severity of disease processes within the upper and lower airways are linked closely, and exacerbations of disease in one component of the airway are likely to encourage worsening of airway disease diffusely.
Several proposed mechanisms have been offered to provide a physiologic framework for understanding the unified airway response. In the early and mid–twentieth century, one primary hypothesis involved a putative nasobronchial reflex, in which neurogenic communication occurred reflexively between the nose and the bronchial apparatus. While early studies appeared to offer some support for this hypothesis, attempts to replicate these findings failed and interest in a nasobronchial reflex waned. A second hypothesis involved the proposed protective mechanism that the nose offered in supporting normal pulmonary function. An observation that occluding the nose in patients with exercise-induced bronchospasm could worsen pulmonary function was offered in support of this mechanism. Again, similar studies have not replicated these effects, and this mechanism has also fallen into disfavor.
More recently, a model of shared inflammation has become of primary interest as a mechanism to account for many observations seen in unified airway disease. Histologically and functionally, the respiratory mucosa throughout the upper and lower respiratory tracts consists of a uniform pseudostratified columnar epithelium that demonstrates similar responses to stimulation with various agents. Many chronic inflammatory conditions of the respiratory tract, including allergic rhinitis, chronic rhinosinusitis, and asthma, share the system-wide expression of Th2 cytokines, such as interleukin (IL)-4, IL-5, and IL-13, as well as the proliferation and influx of cellular mediators, such as eosinophils. Elegant studies conducted by Braunstahl have shown that stimulation with antigen at one respiratory site can result in expression of these inflammatory cytokines at a location distant from the site of stimulation. These findings suggest that there is “inflammatory crosstalk” that occurs throughout the respiratory tract, and that inflammatory processes can therefore progress from one portion of the system to another without difficulty. The activation of Th2 lymphocytes in the nose can lead to the differentiation and activation of immune cells from precursors in the nasal mucosa and bone marrow, leading to recruitment of these newly generated cells throughout the respiratory system. This model of shared respiratory inflammation appears to provide a useful mechanism in understanding processes that occur in the unified airway, and provides a platform to direct future research studies in the area.
Laryngeal involvement in the unified airway
While there has been extensive discussion of how the upper and lower airways interact in acute and chronic illness, the role of the larynx has not been widely described and is currently not well understood. While clinicians have frequently considered the role of allergic rhinitis and asthma in their patients with laryngitis, dysphonia, and cough, systematic study in this area has been uncommon. The larynx possesses a unique anatomic role. It is situated between the upper and lower airways and is therefore a conduit for both upstream and downstream trafficking of mucus and mucopurulent secretions. Effects on the larynx that lead to symptoms of cough and dysphonia could therefore occur either through (1) direct effects of airway inflammation in the laryngeal structures, (2) manifestations of the trafficking of materials through this anatomic region, or (3) the development of secondary edema (particularly in the interarytenoid area as well as the vocal process of the arytenoids) as a result of the cough.
At the cellular level, two leukocyte populations are present and can participate in acute and chronic laryngeal inflammation: (1) mast cells and (2) eosinophils. Mast cells act as the primary cellular mediators of the acute allergic response. When exposed to an antigen in a previously sensitized individual, mast cells degranulate and release histamine and other vasoactive compounds rapidly into the local tissues. While mast cells are abundant in the mucosa of the epiglottis and immediate subglottis, they are not present in the mucosa of the true glottis and vocal folds. Pathophysiologically, these mast cell populations occur in those regions of the larynx that are most responsive to acute anaphylactic reactions: the supraglottis and subglottis. Edema of the vocal folds in the setting of anaphylaxis is less common and pronounced, and cellular infiltration of the larynx in anaphylaxis is often characterized by the presence of eosinophils at postmortem.
In chronic laryngeal inflammation, however, the most common presenting symptoms include dysphonia, transient throat clearing, and cough. In fact, nonproductive coughing episodes are often described as a primary complaint of patients with chronic allergic laryngitis. Diffuse laryngeal inflammation can be appreciated in acute laryngitis, especially in the epiglottis and immediate subglottis. In chronic laryngitis, however, inflammatory changes appear to be confined to the vocal folds, with minimal erythema and no compromise on the airway. In addition, animal models show the presence of eosinophils in the laryngeal mucosa among sensitized rats after exposure.
A small body of clinical research has discussed the effects of allergic influences on the larynx. Chadwick suggested that laryngeal dysfunction and symptom expression are influenced by both inflammatory and biomechanical laryngeal disturbances in allergic patients. These factors act synergistically to create chronic changes in the larynx and adjacent airway, and produce the range of symptoms commonly experienced by these patients, including dysphonia, throat clearing, and cough. In another paper, Corey and colleagues described two forms of allergic laryngitis: (1) acute, (anaphylactic) and (2) chronic. The acute, anaphylactic response represents an acute angioedema, in which there is rapid edema of the lips, tongue, pharynx, and larynx in response to exposure to a sensitized antigen. This type of acute response can also be accompanied by systemic symptoms, such as urticaria, dyspnea, and tachycardia, and can rapidly proceed to become life threatening. Acute asphyxia is the primary cause of death among these individuals. In contrast, chronic laryngeal allergy presents with a different symptom complex and a much less aggressive course. Symptoms include hoarseness, throat clearing, globus sensation, and cough, and are often seen coseasonally in patients with allergic rhinitis. Physical examination of these patients demonstrates mild vocal fold edema, increased presence of mucus in the endolarynx, mild to moderate erythema of the arytenoid mucosa, and thick mucus strands that can bridge the vocal folds.
Several researchers have examined the interaction between physiologic and behavioral factors in the pathogenesis of symptoms among patients with presumed laryngeal allergy. Cohn and colleagues, for example, have suggested that symptoms of allergic rhinitis, such as pharyngeal dryness and postnasal drainage, lead to mucosal irritation in the larynx and pharynx, which then provokes a sense of itching or tickling in the throat and leads to such behaviors as throat clearing and coughing. Abusive behaviors can then injure the vocal folds, leading to mucosal tears, hemorrhage, and Reinke edema. This cycle of inflammatory and biomechanical influences can result in a downward spiral among patients with respiratory allergy, and can lead to chronic changes in laryngeal anatomy and function.
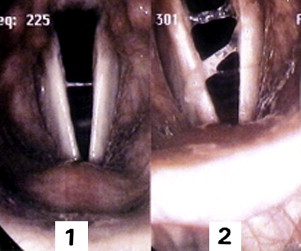
Direct stimulation of the larynx with antigen in sensitized individuals has also been shown to provoke observable adverse effects in the larynx and pharynx. In a series of experiments from our voice laboratory at Wayne State University Department of Otolaryngology–Head and Neck Surgery, Temple University School of Medicine, subjects demonstrated to be allergic to the house dust mite Dermatophagoides pteronyssinus by skin testing underwent direct inhalational challenge of the larynx with aerosolized antigen in increasing concentrations. With increasing exposure, subjects demonstrated not only the presence of increased mucus in the larynx, but also coughing and throat clearing with dyspnea ( Fig. 1 ). It was unclear whether this mucus was generated within the larynx itself or was transported to the larynx from the lungs during cough. In sensitized subjects, there was also a rapid decline in pulmonary function, suggesting immediate-onset bronchospasm with antigen challenge. These findings support the observation that increased mucus in the larynx and cough are two prominent and reproducible findings among patients with allergic laryngeal symptoms. In addition, the same laboratory has demonstrated that allergic individuals may perceive subtle voice changes even in the absence of more significant symptoms, such as cough.
Other researchers have confirmed the roles of increased mucus production and upstream and downstream mucus trafficking in patients with chronic laryngeal allergy. In observing a large number of patients from a professional voice practice, these researchers noted the common coexistence of irregular glottic edema, excessive sticky mucus secretions in the endolarynx, and dysphonia among symptomatic patients with allergic rhinitis. Some of these patients had symptoms of reflux, although many did not. In addition, about 25% of patients in this study demonstrated abnormalities in pulmonary function testing, again confirming that both upper and lower airway influences were present in many individuals. The study confirms the complex interaction that can occur in these allergic patients with dysphonia and cough.
Mucus, neurologic reflexes, and neurogenic inflammation
The many roles of mucus are important in both health and disease. Mucus is continuous from the nasal vestibule to the distal alveoli, and serves multiple functions including:
- •
Humidification of inspired air, which lowers oxygen tension for circulatory exchange and reduces dehydration of the mucosa
- •
Warming of the inspired air to provide temperature equilibration in the lungs
- •
Mechanical protection of the underlying mucosa, clearance of foreign particles (including bacterial, viral, and fungal elements), and preservation of ciliary function
- •
Communication between the upper and lower respiratory tracts to signal a protective response to caustic material and disease.
In addition, mucus gene expression is modified in response to different disease states, as well as exposure to infection, caustic inhalants, and particulate/irritant material.
Although the sinonasal-bronchial reflex has fallen out of favor as a predominant mechanism unifying the upper and lower airways, there is anecdotal evidence of neural reflexes in the airway based on clinical observation. These observations include:
- •
The tendency of a patient to cough when a flexible endoscope is first placed into the nares, and laryngeal “guarding” (adduction) when the scope is advanced into the pharynx
- •
Perceived shortness of breath with new-onset nasal obstruction or placement of bilateral nasal packing
- •
The smooth muscle constriction present in bronchial hyperreactivity (and in response to upper respiratory stimulation of the unified airway) is under both local as well as neurologic control
- •
Neurologic reflexes present in cough involve vagal nuclei that have broad influence within the respiratory as well as digestive tracts.
The autonomic nervous system has been implicated in reflexive behavior associated with nonallergic/vasomotor rhinitis, allergic rhinitis, and gastroesophogeal reflux disease associated with bronchial hyperreactivity. In the example of vasomotor rhinitis, Loehrl and colleagues demonstrated a hypoactive sympathetic nervous system relative to the parasympathetic nervous system compared with controls. Furthermore, disruption of the cervical sympathetic supply to the nose has been shown to result in chronic inflammation and nasal eosinophilia on the affected side, providing support for the interaction of the autonomic nervous system and the inflammatory response. Also, Lodi and colleagues demonstrated significant autonomic dysfunction in patients with gastroesophogeal reflux disease and asthma.
The inflammatory process is now known to involve submucosal mediators, such as substance P, and other mediators that modulate sensory nerve excitability. This nerve excitability is responsible for instigating a cough response, and also potentially plays a central role in impaired laryngeal sensory feedback, which is common in many voice disorders. Although the concept of “neurogenic inflammation” is still controversial, it makes sense that neurogenic mediators are present and that these mediators link (1) surveillance (by the mucus, inflammatory mediators, and resulting altered mucus gene expression), (2) sensory nerve sensitivity modulation, and (3) a systemic nervous system response. However, the clinical importance of these links has yet to be determined.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


