Retinopathy of Prematurity (ROP)
Emmanuel Chang MD, PhD
Antonio Capone MD
1st edition contributions from Anna Ells, MD, FRCS (C).
Introduction and Background of Retinopathy of Prematurity
Retinopathy of prematurity (ROP) is a vasoproliferative retinopathy affecting premature infants of low birth weight. With the advancing medical technology to sustain newborns of very young gestational age, there is a resurgence of ROP despite restricted oxygen saturation monitoring. It is the leading cause of preventable blindness in children.1,2 ROP also remains a leading cause of blindness worldwide3: developed countries are seeing an increase in ROP as neonatologists have the ability to improve survival of the extremely young gestational age infants < 24 weeks, and developing countries are seeing an increase in survival of premature infants due to improved access to neonatal equipment.4 This chapter will provide a basic clinical foundation and understanding of ROP and review the landmark clinical trials conducted over the last 20 years.
Pathogenesis of Retinopathy of Prematurity
ROP is multifactorial in origin, with incomplete retinal vascularization as a consequence of prematurity a prerequisite. Retinal vascular development begins prior to 16 weeks gestation and grows steadily from the optic nerve toward the ora serrata.5 Vascular development of the immature, incompletely vascularized retina is highly influenced by systemic oxygen concentration levels and is regulated in part by vascular endothelial growth factor (VEGF). Normal vasculogenesis during early fetal development is determined by local “physiological” hypoxia as a consequence of increasing retinal thickness, which creates an increase in metabolic demand in advance of the developing intraretinal vessels. Astrocytes in this hypoxic leading edge respond by secreting VEGF that promotes vascular development to meet the increasing metabolic demand of the maturing avascular retina, resulting in normal vasculogenesis from the optic nerve to the ora serrata.6,7
ROP occurs as a result of an oxidative insult that inhibits normal retinal vasculogenesis of the maturing avascular retina. The prematurely born neonate is exposed to dramatically elevated oxygen levels (relative to intrauterine physiologic oxygen concentration), resulting in retinal hyperoxia, vasospasm, and shutdown of sections of the developing retinal vasculature. The ensuing retinal ischemia stimulates a reactive overproduction of VEGF, which leads to the pathologic vasculogenesis known as ROP.7,8
Insulin-like growth factor-1 (IGF-1) has also been implicated in controlling VEGF activation where low levels of IGF-1 prevent vascular development. Oxygen-independent IGF-1 and oxygen-dependent VEGF are complementary and synergistic vascular signaling mechanisms.9 Genetic factors, such as defects in Norrie disease gene and Frizzled-4 gene, have also been implicated in the pathogenesis of ROP,10,11 suggesting that some preterm babies may have a genetic predisposition to ROP.12 This line of research suggests opportunities for therapies targeting the production of specific isoforms of VEGF or intervening at various steps of misregulated vasculogenesis.
In the normally developing eye, regression of the vitreohyaloidal vascular network occurs concurrently with retinal vasculogenesis. Imbalances of VEGF and other growth factors may also impair normal regression of vitreohyaloidal vasculature, impacting vitreous development and organization in the developing neonate as well.
International Classification of Retinopathy of Prematurity— (ICROP-II)
The International Classification of ROP (ICROP)13,14,15 provides a widely accepted vocabulary describing the clinical features of ROP.
Location of Retinopathy: The retina is divided into three concentric circles or zones, centered on the optic disc. The lower the zone, the more severe the disease (Fig. 13.1).
Zone I—the posterior pole, consisting of a circle whose radius is twice the distance from the optic disc to the macula.
Zone II—a doughnut-shaped area of retina that extends from the edge of zone I to a position tangential to the nasal ora serrata and around an area near the temporal anatomic equator.
Zone III—the outermost residual crescent of retina anterior to zone II.
Severity of the Retinopathy: The severity of the disease is attributed to the stage of the disease. The higher the stage, the more severe the disease.
Stage 1: a demarcation line separating the normally developing retina from avascular, peripheral retina
Stage 2: ridge of mesenchymal tissue with height and width in the region of the demarcation line
Stage 3: the ridge develops extraretinal fibrovascular proliferation (EFP) or neovascularization (Fig. 13.2)
Stage 4: partial retinal detachment (Fig. 13.4) Stage 4A—detachment that does not include the macula Stage 4B—detachment that does involve the macula
Stage 5: complete retinal detachment
Extent of Retinopathy: The extent of the disease is reported according to the circumferential accumulation of ROP, reported in clock hours in the appropriate zone.
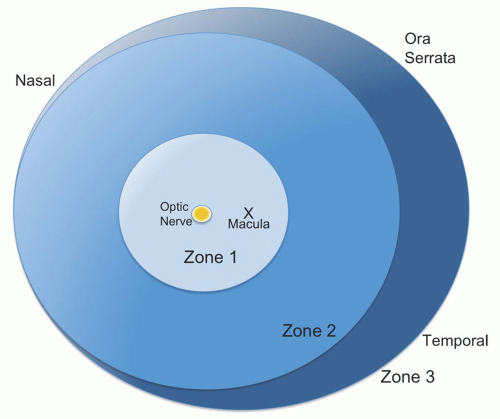 FIGURE 13.1 Diagram illustrating zones and clock hours used in the classification of retinopathy of prematurity. |
Plus Disease
The presence of dilatation and tortuosity of posterior retinal vessels in at least two quadrants that may later increase in severity to include iris vascular engorgement,
poor pupil dilation in response to medication (rigid pupil), and vitreous haze are the characteristic features of “plus disease” (Fig. 13.3). Vitreous haze occurs as a consequence of blood-ocular barrier compromise and is associated with a particularly poor prognosis. Plus disease may be superimposed on any stage of ROP and is a sign that ROP is, or may become, severe.16,17
poor pupil dilation in response to medication (rigid pupil), and vitreous haze are the characteristic features of “plus disease” (Fig. 13.3). Vitreous haze occurs as a consequence of blood-ocular barrier compromise and is associated with a particularly poor prognosis. Plus disease may be superimposed on any stage of ROP and is a sign that ROP is, or may become, severe.16,17
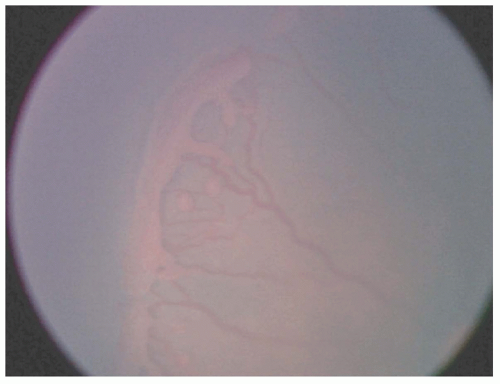 FIGURE 13.2 Photograph of right eye highlighting stage 3 extraretinal fibrovascular proliferation and several “popcorn” lesions (early fibrotic neovascular buds). Note avascular retina anterior to stage 3 retinopathy of prematurity. |
Advanced plus disease is obvious, but mild plus diseases can sometimes be difficult to delineate in ROP when classic EFP is not apparent. A standard photograph can be used to define the minimum amount of vascular dilatation and tortuosity required to make the diagnosis of plus disease, and this approach has been used extensively in multicentered clinical trials.
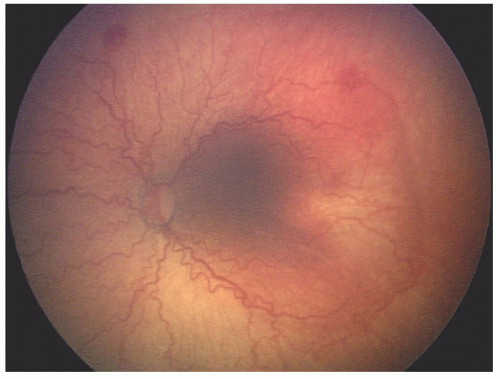 Figure 13.3 This photograph demonstrates vascular changes of the posterior pole vessels consistent with plus disease in all four quadrants. Note zone I, temporal, “flat” neovascularization and circumferential vessels, as seen in aggressive posterior retinopathy of prematurity. |
The description so far refers to the acute phases of ROP. After the acute phase, regression of abnormal fibrovascular tissue can lead to late features, including cicatricial distortion of retinal architecture, with dragging of the retina usually toward the temporal retinal periphery and collapse of the temporal vessel arcade angle (Fig. 13.4).18
Revision of the International Classification of Retinopathy of Prematurity (2005)—ICROP-II15
The 1984-1987 classification has recently been revisited and published for the first time, in its entirety. As a result of research and experiences gained over the last 20 years, the following amendments have been made:
Clarification of zone I. If the disc is seen at the edge of the retinal image when examining the retina with a 25 or 28 D lens, the approximate limit of zone I will be visualized at the opposite edge of the condensing lens.
Addition of pre-plus to the classification. Pre-plus is defined as increased dilation and/or tortuosity of retinal arteries and/or veins in at least two quadrants, which is not severe enough to meet the criteria of plus disease (Fig. 13.5). These dilated and/or tortuous vessels are often present peripherally, initially near the ridge and progress posteriorly with increasing VEGF activity. Therefore, it is important to evaluate the vasculature near the ridge since simply evaluating the vasculature near the optic disc may miss early pre-plus clinical findings. Over time, the vessel abnormalities of pre-plus may progress to frank plus disease or revert to normal.
Addition of “aggressive, posterior ROP” (AP-ROP). This is a once uncommon severe form of ROP, which presents earlier and
progresses rapidly to stage 4 and 5 if left untreated (Fig. 13.6). AP-ROP has the following characteristics:
Posterior location—Usually zone I
Plus disease without prominent ridge proliferation or classic stage 3
Low-lying, tangled web of vessel (sometimes called “flat neovascularization”)
Typically extends circumferentially
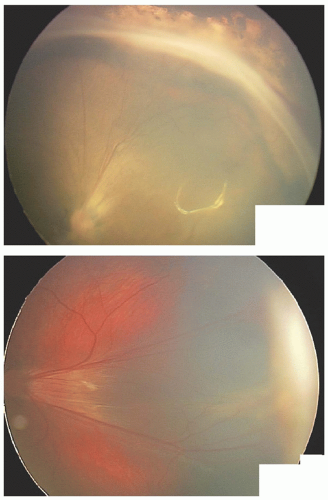 Figure 13.4 Wide-angle photograph of cicatricial retinopathy of prematurity. Note dragging of retinal vessels and significant collapse or narrowing of the temporal arcade angle. Also note peripheral elevated fibrotic membrane, remnant of a stage 4B detachment, forming a macular fold. |
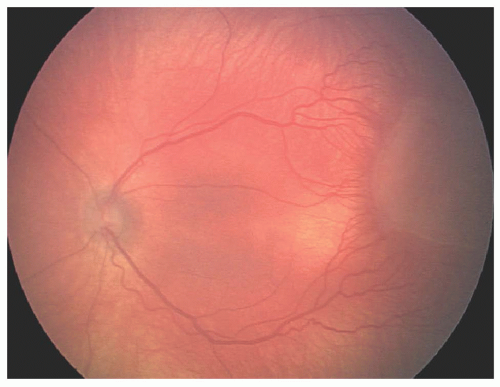 FIGURE 13.5 Photograph demonstrating pre-plus vascular changes in the temporal quadrants, forming a “notch-type” configuration of stage 3 disease. |
Major Clinical Trials in Retinopathy of Prematurity
The Multicenter Trial of Cryotherapy for Retinopathy of Prematurity (CRYO-ROP)—1990
Supplemental Treatment of Oxygen Protocol for Retinopathy of Prematurity— 2000
The Early Treatment for Retinopathy of Prematurity Study—2003
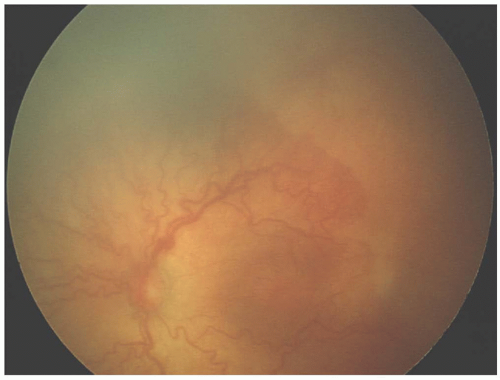 FIGURE 13.6 Photograph demonstrating aggressive posterior retinopathy of prematurity (posterior, flat neovascularization, associated with plus disease in all four quadrants). |
The Multicenter Trial of Cryotherapy for Retinopathy of Prematurity
A multicenter randomized trial by the Cryotherapy for ROP Cooperative Group, which published its first outcome report in 1990.
Study Question
Does retinal ablation using cryotherapy of the peripheral avascular retina reduce the risk of significant visual loss (stage 4 or above; macular retinal fold; vision less than 20/200) in the treated eye?
Using natural history data from nontreated eyes, what are the factors associated with development of severe ROP and unfavorable outcomes?
Inclusion Criteria
Birth weight less than 1,251 g
Survived at least 28 days
Exclusion Criteria
The presence of lethal congenital abnormalities
Major ocular abnormalities
Progression beyond threshold disease in either eye, prior to randomization
Transfer of infant to a nonstudy hospital or follow-up not feasible
Definition of Threshold Retinopathy of Prematurity
Five continuous or eight noncontinuous clock hours of stage 3 ROP, in the presence of plus disease. This definition was based on natural history ROP data, indicating that there was a “threshold” of amount of severe disease, which predictably resulted in significant cicatricial ROP and subsequent poor visual outcome.
Study Design
This is a multicenter, randomized interventional study with a longitudinal natural history cohort. During serial biweekly or weekly ROP examinations, if both eyes developed “threshold ROP,” one eye was randomized to receive treatment of the peripheral avascular retina for 360° using cryotherapy or no treatment. If only one eye reached threshold ROP, then only that eye was randomized to cryotherapy or no treatment. Cryotherapy was performed within 72 hours of determination of threshold disease, to limit the risk of progression of disease to stage 4.
A detailed fundus examination was performed independently by two investigators at 3 and 12 months after cryotherapy and
stereophotographs of the posterior pole and the anterior segment of the eye were then sent to a Fundus Photograph Reading Center where photographs were graded as “unfavorable outcome” or “favorable outcome.”
stereophotographs of the posterior pole and the anterior segment of the eye were then sent to a Fundus Photograph Reading Center where photographs were graded as “unfavorable outcome” or “favorable outcome.”
Unfavorable Outcome: An unfavorable structural outcome referred to a retinal fold involving the macula or a retrolental tissue. An unfavorable visual outcome referred to Snellen visual acuity less than 20/200.
Favorable Outcome: A favorable structural outcome referred to no retinal fold through the macula, with an attached retina. A favorable visual outcome referred to Snellen visual acuity of 20/200 or better.
Summary of Major Findings (Table 13.1)
The average number of clock hours of stage 3 at determination of “threshold” was 9.6 in both treated and nontreated eyes.
Infants who reach “threshold ROP” should be treated because the risk of blindness is predicted to approach 50% at this level of disease severity. A total of 50.6% of the control eyes were categorized as being blind or having low vision, whereas only 31.9% of the treated eyes showed acuity results in the blind or low vision category at the 1-year outcome.
Peripheral retinal ablation with cryotherapy reduced the incidence of retinal detachment by 50% and reduced the incidence of “unfavorable” visual outcome from 56.3% to 35.0% in the treated eyes.
Long-term follow-up of these children confirms the continued benefits of treatment, but despite the best available treatment at that time, over 50% of children had a visual acuity of <20/200 in the treated eye at 10 years.19 The proportion of eyes with visual acuity 20/200 or better was 25.9% in the control group and 48.9% in the treated group at the 15-year examination.
TABLE 13.1 Summary of the CRYO-ROP Outcomes Published to Date | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
Implications for Clinical Practice
The question of whether or not cryotherapy ablating the avascular retina in the presence of a significant amount of EFP (threshold ROP) would decrease cicatricial ROP and the resultant loss of vision or blindness led first to the unification of the ROP classification and then publication of the ICROP. The formation of the Cryotherapy for ROP Cooperative Group soon followed to study the question of treatment using cryotherapy for this potentially blinding disease. This clinical trial was not the first study addressing treatment of ROP but it was the first multicenter randomized clinical trial in the treatment of ROP.23,24
With the advent of argon and diode lasers in treating other retinal diseases, and the publication of smaller studies demonstrating that ablation of the peripheral avascular retina reduced the likelihood of visual loss and blindness, photocoagulation of the avascular retina for threshold ROP quickly replaced cryotherapy in many centers throughout North America and the world.25,26,27,28,29,30 Transpupillary diode and argon retinal laser photocoagulation has subsequently been shown in small clinical studies to reduce
the amount of myopia and improve visual outcomes from less pigment disruption in the macula, when compared with cryotherapy.31,32
the amount of myopia and improve visual outcomes from less pigment disruption in the macula, when compared with cryotherapy.31,32
An enormous amount of information about the natural history of ROP was documented as the secondary objective of the CRYO-ROP study in the 1-, 5-, 10-, and 15-year outcome reports. The salient points with clinical applications are summarized as follows:
Age of Onset of ROP: ROP develops over a relatively narrow postmenstrual age (PMA) range and is related more to the stage of development of the infant, by PMA, than neonatal events.33,34
Zone of involvement: The propensity for severity is governed to a large extent by the state of retinal vascularization at birth, so that zone is perhaps the most important predictor of outcome.17,35 Thus, incomplete vascularization in zone I carries a 54% risk of reaching threshold, but this falls to only 8% when vessels have reached zone II.
Progression of Disease: The more premature the neonate, the more posterior the zone or location of the retinopathy and the greater the potential for progression of the disease. Thus, zone I disease is very likely to progress to stage 3 needing treatment, but ROP confined entirely to zone III rarely requires treatment. As with the onset, the rate of progression is also governed predominantly by developmental age (i.e., PMA) rather than by postnatal age, or neonatal events.33 The median PMA at which the various stages develop is as follows: stage 1, 34 weeks; stage 2, 35 weeks; stage 3, 36 weeks, and for threshold ROP, 37 weeks PMA (Fig. 13.7). In the CRYO-ROP study, babies were randomized for treatment within 72 hours of diagnosis of threshold ROP, which was at a mean age of 37.7 weeks PMA (range 32-50 weeks).20 This was confirmed by comparing the rate of progress in CRYO-ROP and LIGHT-ROP trials.36 It is important to note the extremes of this range. Subhani et al.37 reported threshold ROP at 31 weeks PMA, but almost all infants will develop severe ROP by 46.3 weeks PMA. The no-treatment, natural history arm of the CRYO-ROP trial showed that once threshold develops, there is progression to an unfavorable outcome in approximately 50% of eyes.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


