Retinal Vein Occlusions (Evidence-Based Eye Care)
Paul Hahn MD, PhD
Sharon Fekrat MD, FACS
Introduction
Retinal vein occlusion (RVO), including both branch retinal vein occlusion (BRVO) and central retinal vein occlusion (CRVO), is a retinal vascular disorder with significant sight-threatening morbidity.1,2,3,4 BRVO is three times more common than CRVO and second only to diabetic retinopathy as the most common retinal vascular cause of visual loss.5,6,7 BRVO results from a blockage of blood flow in a branch retinal vein. This blockage typically occurs where a branch artery crosses over the branch retinal vein, resulting in a sectoral, wedge-shaped distribution of intraretinal hemorrhages, venous tortuosity and dilation, cotton wool spots, and/or cystoid macular edema (Fig. 9.1). In CRVO, a thrombus is suspected at the level of the lamina cribrosa, generally resulting in a sudden decrease in visual acuity (VA) with four quadrants of dilated tortuous retinal veins, intraretinal hemorrhages, cotton wool spots, optic disc swelling and hyperemia, and/or cystoid macular edema (Fig. 9.2).
The mechanism of RVO is multifactorial and poorly understood but is suggested by its associated risk factors, primarily systemic arterial disease such as hypertension, diabetes, hyperlipidemia, atherosclerosis, increased body mass index, and smoking.8,9,10,11,12,13,14,15 RVO is commonly an age-related disease, and individuals less than 60 years of age may have a greater association with hypercoagulable states and inflammatory conditions compared with older persons with a higher incidence of systemic vascular disease risk factors.16,17,18
Primary causes of visual loss with RVO include macular edema and neovascularization, with secondary vitreous hemorrhage and/or neovascular glaucoma. Until recently, the standard of clinical management had been dictated for over 20 years by the Branch Retinal Vein Occlusion Study (BVOS) and the Central Retinal Vein Occlusion Study (CVOS). These landmark studies recommended grid-pattern laser photocoagulation for perfused macular edema in eyes with BRVO5,19 and observation of macular edema in CRVO; panretinal laser photocoagulation (PRP) was recommended for the treatment of RVO-associated neovascularization.5,19 Recent clinical trials investigating novel therapies have significantly expanded our understanding of RVO pathogenesis and our therapeutic options, setting a new standard of care for RVO-associated macular edema. This chapter reviews major clinical trials, focusing on currently available therapies that have recently advanced our treatment of RVO.
The Branch Retinal Vein Occlusion Study
The BVOS was a multicenter, prospective, randomized, controlled trial sponsored by the National Eye Institute (Fig. 9.3).5,6 This trial was originally designed to study patients from 1977 to 1984 to determine whether peripheral argon laser photocoagulation can prevent the development of neovascularization and/or vitreous hemorrhage and whether grid-pattern laser photocoagulation can improve VA in eyes with perfused macular edema.
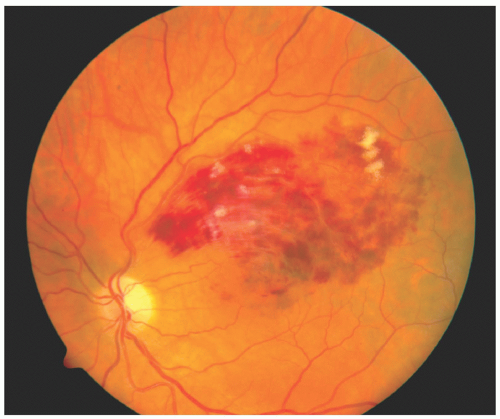 FIGURE 9.1 Fundus photograph of a branch retinal vein occlusion demonstrating typical features of sectoral intraretinal hemorrhages and cotton wool spots. |
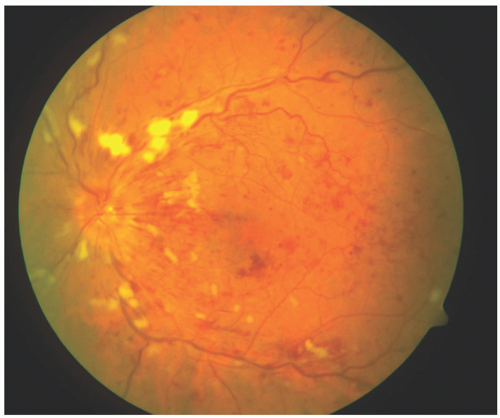 FIGURE 9.2 Fundus photograph of a central retinal vein occlusion demonstrating typical features of intraretinal hemorrhages, cotton wool spots, and venous tortuosity in four quadrants along with macular thickening. |
In the BVOS, eyes with a BRVO were placed into four groups. Group I eyes had a BRVO without neovascularization but with pathology covering at least five disc diameters in diameter, which was felt to place these eyes at high risk for developing neovascularization. Eyes in this group were randomized to sector PRP or no laser treatment to determine whether PRP prevented the development of neovascularization. Group II eyes had a BRVO with neovascularization of the disc or within one disc diameter of the disc and were at risk for the development of vitreous hemorrhage. The eyes were randomized to sector PRP or no laser treatment to determine whether PRP could prevent vitreous hemorrhage. Group III eyes had a BRVO with reduced vision to 20/40 or less and perfused macular edema, characterized by <5 disc diameters of retinal capillary nonperfusion; these eyes were randomized to grid-pattern laser photocoagulation or no laser treatment. Finally, eyes in Group X, with inclusion criteria similar to Group I, were recruited only after Group I recruitment
was closed and were followed up primarily to obtain natural history information.
was closed and were followed up primarily to obtain natural history information.
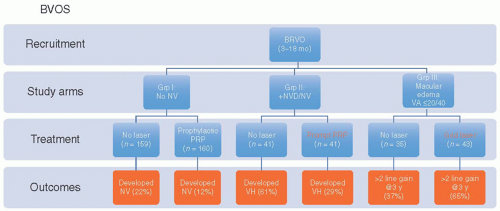 FIGURE 9.3 BVOS—statistically significant results are highlighted with orange boxes. BRVO, branch retinal vein occlusion; BVOS, Branch Retinal Vein Occlusion Study; PRP, panretinal laser photocoagulation; VA, visual acuity; NV, neovascularization; NVD, neovascularization at the disc; VH, vitreous hemorrhage. |
Spontaneous visual improvement in eyes with BRVO has been reported in smaller studies.20,21,22 In the BVOS, VA in untreated BRVO eyes improved a mean of 0.23 lines over 3 years. Based on the BVOS, however, it is difficult to fully understand the natural history of eyes with a BRVO.23 The BVOS natural history data involved only a small number of subjects, with 35 untreated eyes at 3 years.5 Furthermore, eyes with BRVO duration ranging from 3 to 18 months were grouped together, and natural history was then determined from this group of eyes. Moreover, as BVOS enrollment required eyes to have had a BRVO of at least 3 months duration, no natural history data can be ascertained from the onset of BRVO to 3 months. Only BRVO eyes with perfused edema without foveal hemorrhage were enrolled, so no natural history information is available from the BVOS regarding eyes with ischemic edema or foveal hemorrhage.
Grid-Pattern Laser Photocoagulation
The BVOS evaluated grid-pattern laser photocoagulation for the treatment of perfused macular edema, recommending grid laser in those eyes with a BRVO of 3 to 18 months duration, a reduced VA ≤ 20/40, and without foveal hemorrhage.5 The BVOS protocol involved focal laser in a grid-pattern in the area of leaking capillaries within two disc diameters of the foveal center but outside of the foveal avascular zone (Fig. 9.4). It is important to realize that eyes in the BVOS were not rigorously divided into categories of macular perfusion (i.e., perfused vs nonperfused macular edema) because the quality of the fluorescein angiograms was generally not adequate to differentiate.24 However, patients with “distinct” areas of capillary nonperfusion in the macula were excluded. Although the BVOS is the largest randomized trial comparing laser treatment to observation for macular edema, with 71 treated and 68 untreated eyes, the reported 3-year data were only from 43 treated and 35 untreated eyes.5 These small numbers and lack of precise angiographic differentiation of macular edema make the results difficult to interpret.
Nevertheless, the BVOS demonstrated a benefit of grid-pattern laser photocoagulation treatment for macular edema that met the criteria defined in the preceding text.5 At 3 years, 65% of 43 treated individuals gained at least 2 lines of vision compared with 37% of 35 eyes in the untreated control group (Fig. 9.3).5 This finding led to the recommendation that persistent BRVO-associated perfused macular edema and VA ≤ 20/40 be treated with grid-pattern laser photocoagulation, which had remained the standard of care until the recent development of intravitreal pharmacotherapy.
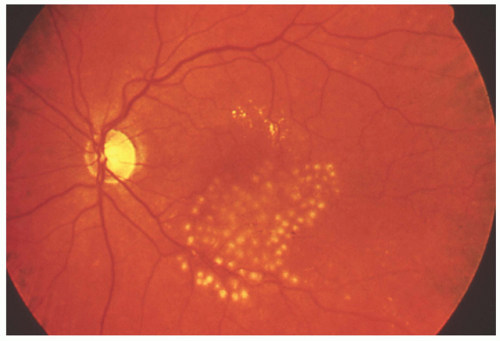 FIGURE 9.4 Fundus photograph of an inferotemporal branch retinal vein occlusion with macular edema treated in the Branch Retinal Vein Occlusion Study with grid laser photocoagulation. |
Scatter Laser Photocoagulation
The data from BVOS groups I and II demonstrated that scatter argon laser photocoagulation in the affected distribution effectively reduces the development of retinal neovascularization and vitreous hemorrhage when compared with BRVO eyes in the untreated group. In group I, it was found that 12% of 160 laser-treated eyes developed retinal neovascularization compared with 22% of 159 untreated eyes. In group II, 29% of 41 treated eyes developed a vitreous hemorrhage as compared with 61% of 41 untreated eyes. Thus, it was concluded that scatter laser effectively decreases the likelihood of developing neovascularization and/or vitreous hemorrhage.5,6 The BVOS did not directly address the optimal timing of PRP placement, but extrapolated data from both groups suggest that PRP placed after the development of neovascularization is as effective as prophylactic laser in reducing the incidence of vitreous hemorrhage. The BVOS therefore recommended that PRP be placed only after the development of neovascularization rather than prophylactically.
The Central Retinal Vein Occlusion Study
The CVOS was a multicenter, prospective, randomized, controlled clinical trial conducted between 1988 and 1992 (Fig. 9.5).25,26 The CVOS sought to understand the natural history of perfused CRVO, to determine the role of grid-pattern laser photocoagulation in the treatment of macular edema, and to determine optimal timing of PRP treatment for CRVO-associated neovascularization.
In the CVOS, eyes were categorized into three groups according to perfusion status: perfused, nonperfused, or indeterminate. A nonperfused CRVO exhibited >10 disc areas of retinal capillary obliteration on fluorescein angiography based on a defined photographic protocol using a conventional wide-angle fundus camera with sweeps of the mid-periphery 30 seconds after intravenous injection of sodium fluorescein. Interestingly, in contrast to the preceding BVOS, which defined nonperfusion based on disc diameters, the CVOS defined nonperfusion based on disc areas. The CVOS only included eyes with onset of CRVO within the preceding 12 months. Eyes were excluded from the CVOS if they had previous laser photocoagulation for any retinal vascular disease in the affected eye, presence of diabetic retinopathy, new or old branch arterial/venous occlusion, retinal neovascularization, vitreous hemorrhage, peripheral anterior synechiae, or concurrent eye disease that decreased VA.
Natural History
Nine clinical centers participated in the CVOS, enrolling 714 CRVO-affected eyes from 711 patients. The number of male patients was slightly more than that of female patients, and over 50% of the patients were 65 years or older. Sixty-one percent of the
patients had some evidence of hypertension. At the initial visit, 546 eyes (76%) were classified as perfused on angiography. Of eyes that were initially classified as perfused, 34% (185 of 547 eyes) converted to nonperfused status by 3 years.26 This progression was found to be strongly associated with duration of CRVO <1 month, VA worse than 20/200, and the presence of 5 to 9 disc areas of nonperfusion on the baseline fluorescein angiogram. Once a patient developed a CRVO in one eye, there was an annual risk of 0.9% of developing a CRVO in the fellow eye.25,26
patients had some evidence of hypertension. At the initial visit, 546 eyes (76%) were classified as perfused on angiography. Of eyes that were initially classified as perfused, 34% (185 of 547 eyes) converted to nonperfused status by 3 years.26 This progression was found to be strongly associated with duration of CRVO <1 month, VA worse than 20/200, and the presence of 5 to 9 disc areas of nonperfusion on the baseline fluorescein angiogram. Once a patient developed a CRVO in one eye, there was an annual risk of 0.9% of developing a CRVO in the fellow eye.25,26
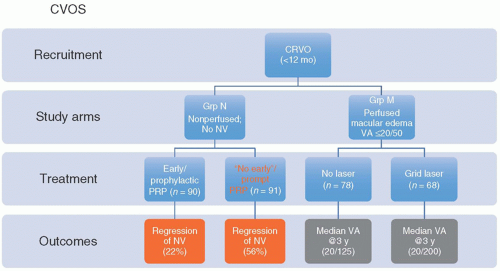 FIGURE 9.5 CVOS—statistically significant results are highlighted with orange boxes; gray boxes highlight nonsignificant, pertinent results. CRVO, central retinal vein occlusion; CVOS, Central Retinal Vein Occlusion Study; PRP, panretinal laser photocoagulation; NV, neovascularization; VA, visual acuity. |
Improvement in VA was strongly associated with the initial baseline acuity.26 In the CVOS, presenting VA was variable: 29% were 20/40 or better, 43% were between 20/50 and 20/200, and 28% were 20/200 or worse; median baseline VA was 20/80. Of the eyes with an initial VA of 20/40 or better, 65% retained VA at this level over 3 years, while the remaining worsened. Among individuals with intermediate VA between 20/50 and 20/200, 41% maintained the same level over 3 years, 21% improved to better than 20/50, and 38% deteriorated to worse than 20/200. Eyes with an initial VA <20/200 had an 80% chance of maintaining poor vision without improvement over 3 years (Table 9.1).
TABLE 9.1 The Central Retinal Vein Occlusion Study | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||
The CVOS demonstrated that eyes with a nonperfused CRVO had a higher risk of developing neovascularization of the iris or angle (NVI/NVA).26 Thirty-five percent of nonperfused eyes (61 of 176 eyes) developed NVI/NVA, compared with 10% (56 of 538) of perfused eyes. The median time to the development of NVI/NVA in nonperfused eyes was 61 days (range: 6 days to 8 months) after enrollment. The development of NVI/NVA was more likely in males and in eyes with a VA worse than 20/200 that had at least 30 disc areas of nonperfusion with moderate-to-severe venous tortuosity and retinal hemorrhage, or with CRVO duration <1 month.
Grid-Pattern Laser Photocoagulation
The CVOS Group M report investigated the role of grid-pattern argon laser photocoagulation in 155 eyes with perfused CRVO-associated macular edema and VA 20/50 or worse.19 Treatment resulted in decreased macular edema as detected by fluorescein angiography, prior to the availability of optical coherence tomography (OCT) imaging. At 12 months, 21 of 68 treated eyes (31%) had no angiographic macular edema compared with 6 of 78 (8%) untreated eyes (p < 0.0001). Despite this anatomic improvement, grid-pattern laser photocoagulation did not improve VA in eyes with CRVO. Initial median visual acuities of 20/125 (observation) and 20/160 (laser treated) were comparable to final median visual acuities at 36 months of 20/160 (observation) and 20/200 (laser treated). Damage to the perifoveal vascular zone has been hypothesized to contribute to this lack of visual recovery despite anatomic improvement. Based on these results, the CVOS concluded that grid-pattern laser photocoagulation in eyes with CRVO-associated macular edema was not visually beneficial. Until the recent identification of novel therapies for CRVO-associated macular edema, the standard of care had been observation.
Panretinal Laser Photocoagulation
Despite the absence of any supporting clinical trial data prior to CVOS, prophylactic PRP had already been widely accepted as the standard of care for the prevention of NVI/NVA in nonperfused CRVO. The optimal timing of PRP treatment had not been established, however, and the CVOS Group N report therefore examined whether PRP treatment should be initiated on a prophylactic basis immediately following the diagnosis of CRVO or delayed until the development of any NVI/NVA.27 Prophylactic PRP in eyes with nonperfused CRVO without neovascularization developed NVI/NVA in 18 of 90 treated eyes (20%), while 32 of 91 untreated eyes (35%) developed NVI/NVA; however, this difference was not statistically significant. Furthermore, once NVI/NVA developed, additional PRP was four times less effective in eyes that had already received prophylactic PRP (4 of 18 eyes; 22%) than control eyes (18 of 32 eyes; 56%) in inducing the regression of neovascularization. The CVOS therefore recommended prompt, but not prophylactic, PRP treatment immediately following the detection of anterior segment neovascularization.27 Prophylactic PRP may be considered in patients with risk factors for developing NVI/NVA (male gender, short duration of CRVO, extensive retinal nonperfusion, and extensive retinal hemorrhage) or when close ophthalmologic follow-up is impossible or unlikely. Persistent neovascularization following PRP must be followed closely, and additional PRP may be needed to halt its progression.
Corticosteroid Therapy
Numerous case reports and case series have suggested the efficacy of corticosteroids in treating RVO-associated macular edema.28,29,30,31,32,33,34 While the mechanism of action remains unknown, recent results from large, prospective, randomized, controlled clinical trials have demonstrated benefit of corticosteroids in treating RVO-associated macular edema. These trials include the National Eye Institute-sponsored Standard Care vs COrticosteroid for REtinal Vein Occlusion (SCORE) study and the Allergan-sponsored Global Evaluation of implaNtable dExamethasone in retinal Vein occlusion with macular edemA (GENEVA) trial, which investigated the role of intravitreal triamcinolone and a sustained-release intravitreal dexamethasone delivery system, respectively, for the treatment of RVO-associated macular edema.
SCORE Trial
Prior to the Food and Drug Administration (FDA) approval of pharmacotherapeutic agents for RVO, the SCORE study compared the efficacy and safety of an off-label intravitreal injection of 1 or 4 mg preservative-free triamcinolone acetonide (IVTA; Trivaris, Allergan, Inc., Irvine, CA) versus standard of care in the treatment of RVO-related macular edema.35,36 Of note, this formulation of triamcinolone is not commercially available. In these trials, hemiretinal vein occlusion (HRVO) was categorized as BRVO. Key
inclusion criteria included VA between 20/40 and 20/400, RVO-associated macular edema on clinical exam, and central subfield retinal thickness ≥250 µm by OCT. Key exclusion criteria included eyes with foveal atrophy, significant cataract, or a recent history of laser treatment, ocular surgery, or intravitreal or peribulbar steroid administration. Eyes were retreated every 4 months during the 12-month study period unless specific criteria were met, including (1) significant improvement (central subfield OCT thickness ≤225 µm, VA ≥20/25, or significant interval improvement with presumed potential for continued improvement without treatment), (2) contraindication due to significant adverse effect (e.g., significant rise in intraocular pressure [IOP]), or (3) additional treatment considered futile due to no improvement following two consecutive injections.
inclusion criteria included VA between 20/40 and 20/400, RVO-associated macular edema on clinical exam, and central subfield retinal thickness ≥250 µm by OCT. Key exclusion criteria included eyes with foveal atrophy, significant cataract, or a recent history of laser treatment, ocular surgery, or intravitreal or peribulbar steroid administration. Eyes were retreated every 4 months during the 12-month study period unless specific criteria were met, including (1) significant improvement (central subfield OCT thickness ≤225 µm, VA ≥20/25, or significant interval improvement with presumed potential for continued improvement without treatment), (2) contraindication due to significant adverse effect (e.g., significant rise in intraocular pressure [IOP]), or (3) additional treatment considered futile due to no improvement following two consecutive injections.
Standard of care for RVO-associated macular edema at the time of the study had been defined by BVOS and CVOS, which recommended grid-pattern laser for perfused macular edema in eyes with BRVO (and HRVO) and observation for macular edema with CRVO. With these different standard of care treatments, the SCORE study was designed with two distinct arms to separately evaluate the role of IVTA compared with standard of care for macular edema secondary to BRVO (411 eyes) and secondary to CRVO (271 eyes).
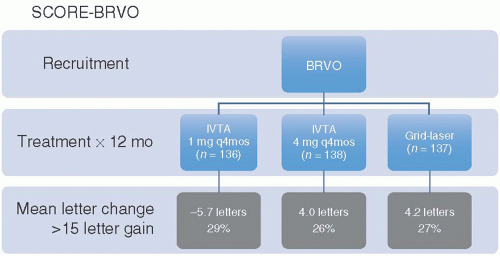 FIGURE 9.6 SCORE-BRVO—gray boxes highlight nonsignificant, pertinent results. BRVO, branch retinal vein occlusion; IVTA, intravitreal triamcinolone acetonide; SCORE, Standard Care vs COrticosteroid for REtinal Vein Occlusion. |
SCORE-Branch Retinal Vein Occlusion Arm. The SCORE-BRVO arm (Fig. 9.6) randomized eyes to 1 mg IVTA (n = 136), 4 mg IVTA (n = 138), or grid-pattern laser (n = 137).35 This study did not detect any difference in VA between eyes treated with IVTA or grid-pattern laser at 12 months. In the 1 mg IVTA, 4 mg IVTA, and grid-pattern laser groups, 29%, 26%, and 27%, respectively, gained ≥15 letters of VA at 1 year. A subgroup analysis of pseudophakic patients demonstrated a trend toward greater than 3 line gains in visual improvement with 1 mg (29%) or 4 mg (28%) IVTA compared with grid-pattern laser (20%), but these differences were not statistically significant. All treatments also resulted in equivalent improvement in mean VA of approximately 4 to 6 letters and similar reductions in macular edema as measured by OCT at 12 months.
The IVTA groups in SCORE-BRVO had an increased rate of side effects, particularly cataract progression and increased IOP, compared with the standard of care group. Cataract progression was noted in 25% of eyes in the 1 mg IVTA group and 35% in the 4 mg IVTA group compared with only 13% in the grid-pattern laser group. IOP-lowering medication was required in 7% and 41% of eyes in the 1 mg and 4 mg IVTA groups, respectively, compared with only 2% of eyes in the grid-pattern laser group. Endophthalmitis and retinal
detachment occurred in <1% of patients in all groups. There was no difference in systemic adverse events across all groups.
detachment occurred in <1% of patients in all groups. There was no difference in systemic adverse events across all groups.
Given the absence of any improvement in visual outcomes with IVTA compared with laser, particularly with a less favorable side-effect profile following IVTA treatment, the SCORE-BRVO trial recommended that grid-pattern laser remain the standard of clinical practice for treatment of BRVO-associated perfused macular edema. SCORE-Central Retinal Vein Occlusion Arm. In the parallel SCORE-CRVO arm (Fig. 9.7), intravitreal injection of 1 mg IVTA (92 eyes) or 4 mg IVTA (91 eyes) was found to confer significant visual benefit in the treatment of CRVO-associated macular edema compared with observation (88 eyes).36 At 1 year, 27% (1 mg) and 26% (4 mg) of patients treated with IVTA gained ≥15 letters compared with 7% of untreated patients. Mean change in VA was a loss of only 1.2 letters in both IVTA groups compared with a loss of 12.1 letters in the observation group. Improvements in central foveal thickness by OCT were only significant following treatment with 4 mg IVTA at 4 months, with a median change of -196 µm in the 4 mg IVTA group compared with -77 µm in the 1 mg IVTA group and -125 µm in the observation group.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


