Purpose
To examine the association of retinal vessel tortuosity with diabetic retinopathy and early nephropathy in type 1 diabetes.
Design
Cross-sectional.
Methods
A total of 1159 participants with type 1 diabetes aged 12 to 20 years, attending diabetes clinics in Children’s Hospital at Westmead, Sydney, Australia between 1990 and 2002, were included. Retinal photography and clinical examinations were performed during the baseline visit to assess diabetic retinopathy and albumin excretion rate (AER). Retinal vessel tortuosity was measured from digitized retinal photographs using a semi-automated computer program by a single grader masked to participants’ characteristics. Diabetic retinopathy was defined as ETDRS level ≥21 (mild nonproliferative retinopathy) and early kidney dysfunction was defined as AER ≥7.5 μg/min.
Results
Of 944 patients (81.4%), 85 (9.0%) had signs of retinopathy only, 250 (26.5%) had early kidney dysfunction only, and 85 (9.0%) had both retinopathy and early kidney dysfunction. In multivariate analysis, higher arteriolar tortuosity was associated with retinopathy (odds ratio [OR] 2.01, 95% confidence interval [CI] 1.23-3.29, the highest quartile vs the remaining 3 quartiles), early kidney dysfunction (OR 1.56, 95% CI 1.06-2.28, per standard deviation [SD] increase), or coexistence of both complications (OR 1.96, 95% CI 1.21-3.24, the highest quartile vs the remaining 3 quartiles).
Conclusions
Greater retinal arteriolar tortuosity was independently associated with retinopathy and early stage of nephropathy in type 1 diabetes. These findings may offer the potential of quantitative measurement of retinal vessel tortuosity for diabetic complication risk assessment.
Retinopathy and nephropathy are leading causes of morbidity and disability in children with type 1 diabetes. Despite the extensive research, the specific mechanisms underlying the pathophysiology of these microvascular complications remain uncertain. Long-established risk factors, including duration of diabetes and HbA1c, only explain certain amount of variation of these microvascular complications, highlighting the need for additional markers for the risk of diabetic microvascular complications.
The retinal microvasculature is the only part of the human circulation system available for direct and noninvasive observations. The association between systemic and retinal hemodynamic changes with diabetes is well documented and subtle variations in retinal vasculature, such as vessel caliber, have been shown to be potential markers of diabetic complications, including retinopathy and nephropathy. Further recognition of diabetes-associated changes in retinal microvasculature is therefore promising to provide early indications of the development of diabetic microvascular complications.
Recently, there has been increasing interest in retinal vessel tortuosity, which might not only be sensitive to early hemodynamic changes in diabetes, but is also more observable than other retinal vascular parameters. We have recently found that retinal arteriolar tortuosity was associated with high HbA1c, even before the presence of retinopathy. This suggests that variation in retinal vessel tortuosity may indicate early pathologic changes before the clinical manifestation of diabetic microvascular complications. In light of this, few studies have suggested that more tortuous retinal vessels are associated with disturbed blood flow and endothelial dysfunction, and may be markers of vascular endothelial growth factor (VEGF) production, which link to early pathology of diabetic microvascular changes. There has also been evidence showing that tortuous vessels are associated with diabetic retinopathy in both experimental and clinical studies. However, most previous studies have used subjective methods to assess retinal vessel tortuosity, which are imprecise and prone to measurement errors, and include small numbers of study subjects.
In this study, we aimed to examine the relationship between retinal vessel tortuosity, measured quantitatively using a computer program, and early diabetic microvascular complications, retinopathy, and early kidney dysfunction, in a large sample of young patients with type 1 diabetes.
Methods
Study Population
The Sydney Pediatric Diabetes Study is a clinic-based study of children/adolescents with type 1 diabetes, aged 12 to 20 years at baseline, who attended the Diabetes Complications Assessment Service at the Children’s Hospital at Westmead during a 12-year period from 1990 to 2002.
Details regarding participants of this study have been published elsewhere. Type 1 diabetes diagnosis followed the criteria of the Australasian Pediatric Endocrine Group Diabetes Register and National Guidelines.
Of 1159 participants with retinal photographs taken, we excluded 215 with ungradable photographs (18.6%), leaving 944 (81.4%) for analysis in this report. Diabetes-related risk factors including duration of diabetes, HbA1c, systolic blood pressure (SBP), body mass index (BMI), and cholesterol were assessed at baseline visits via interview and clinical and laboratory investigation.
Definition of Retinopathy and Early Kidney Dysfunction
Assessment of diabetes complications were also performed during a 2-hour baseline clinic visit with all participants. Details of these procedures have been previously published.
In brief, 7 stereoscopic standard-field retinal photographs, based on the Early Treatment Diabetic Retinopathy Study (ETDRS), were taken on film from both eyes after pupil dilation, using a Topcon fundus camera (TRC 50-VT; Tokyo Optical, Tokyo, Japan). Retinopathy was assessed and graded from these photographs by the same ophthalmologist, according to the ETDRS adaptation of the modified Airlie House classification. Retinopathy was defined as at least 1 microaneurysm/hemorrhage in either eye (ETDRS level 21, minimal nonproliferative diabetic retinopathy or greater). This assessment had a very good agreement, with a kappa value of 0.81.
Early kidney dysfunction was defined as early albumin excretion rate (AER) elevation, when AER ≥7.5 μg/min was found in 2 of 3 examinations.
Measurement of Retinal Vessel Tortuosity
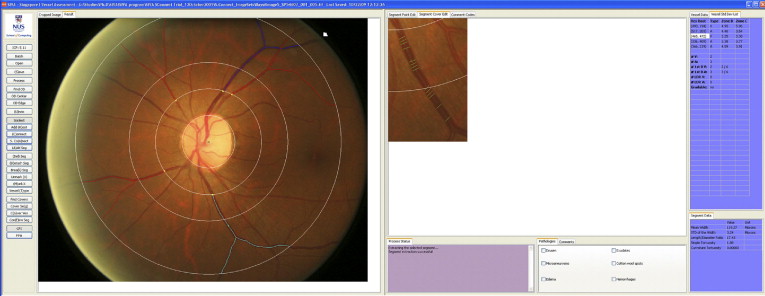
Quantitative measurement of retinal vessel tortuosity, curvature of vessel course, was performed on digitized disc-centered retinal photographs (field 1 of the ETDRS photographic fields) of right eyes, using a semi-automated computer program (Singapore I Vessel Assessment [SIVA]; Department of Computer Science, National University of Singapore, Singapore) ( Figure 1 ) . These measurement procedures have been previously published. In brief, for each retinal photograph, a trained grader, masked to participants’ identities, applied SIVA to the image to detect the center of the optic disc appropriately and divide the region into 3 concentric zones (A, B, and C), each surrounding the optic disc and located 0.5, 1.0, and 2.0 optic disc diameters away. Subsequently, the grader executed the program to trace all vessels. This software has an ability to appropriately detect arterioles and venules in 70% to 80% of the images it is applied to. The grader checked each image to determine if all arterioles and venules were correctly identified, based on information of parent vessels crossing between arterioles and venules and the color of the vessels. Corrections could be made if needed. In 100 randomly selected images, the intra- and inter-grader reliabilities in classification of arterioles and venules were nearly perfect, with kappa value 0.95 to 0.99.
All vessels of more than 40 μm width and routing through all 3 zones were measured. Images were considered poor quality if they were blurred or an incomplete representation of zone C, and classified as ungradable if there were less than 4 large arterioles or venules gradable in 1 image. At the end of the process, a summary of vessel tortuosity was estimated from the biggest 6 arterioles and 6 venules of the eye, and expressed in tortuosity index. It was calculated from the integral of the total squared curvature along the path of the vessel divided by the total length of the vessel arc, using an established formula as follows.
ζ(s)=∑|S|i=1[x′(ti)y′′(ti)−x′′(ti)y′(ti)]2[y′(ti)2+x′(ti)]2λ(s)
ζ ( s ) = ∑ i = 1 | S | [ x ′ ( t i ) y ′ ′ ( t i ) − x ′ ′ ( t i ) y ′ ( t i ) ] 2 [ y ′ ( t i ) 2 + x ′ ( t i ) ] 2 λ ( s )
This quantitative method has high reliability (intra-class coefficient 0.80 for curvature tortuosity and 0.90 for simple tortuosity).
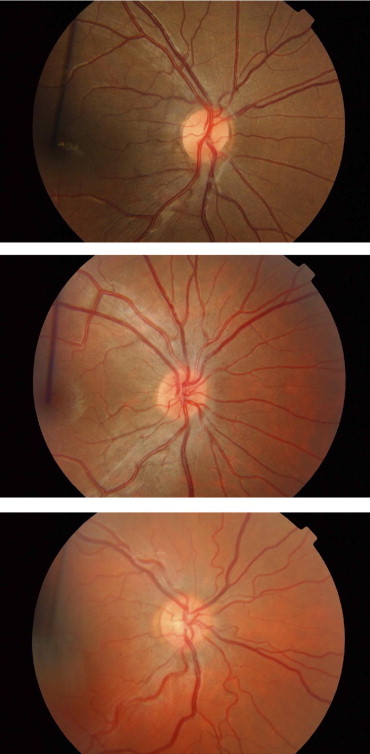
Figure 2 shows examples of 3 retinal images with different tortuosity degrees obtained from this sample. In 30 randomly selected vessels with different degrees of tortuosity, an independent photographic grader ranked these vessels based on the tortuosity index values obtained from SIVA, and this ranking was compared with the rankings performed independently by 3 ophthalmologists with different levels of experience, based on their intuitive examination of the images. The kappa values (all >0.80) indicated high levels of agreement between rankings by the grader (based on measurement from SIVA) and that by the ophthalmologists (based on their intuitive assessment) ( Table 1 ).