Purpose
To correlate surgical difficulty of epiretinal membrane (ERM) removal with characteristics of ERM adherence seen by spectral-domain optical coherence tomography (SD-OCT).
Design
Prospective observational case series.
Methods
Surgical difficulty was correlated with extent of ERM adherence by SD-OCT using masked observers in consecutive eyes undergoing ERM removal (N = 31). Surgical videos were analyzed and difficulty of ERM removal (grade 1-3) was determined in 4 quadrants as well as the fovea by consensus of observers masked to SD-OCT findings. Extent of ERM adhesion was categorized (focal, broad, or complete) by masked observers using SD-OCT. The presence of fibrillary changes between the ERM and retinal nerve fiber layer (RNFL) was also evaluated. Surgical difficulty of ERM removal for each quadrant and fovea was compared to extent of ERM adherence and presence of fibrillary changes.
Results
Assessment of ERM adherence using SD-OCT between masked observers was highly concordant (kappa = 0.9178). Surgical difficulty of ERM removal was strongly associated with more extensive ERM adherence to the retina observed by SD-OCT. Complete ERM adherence correlated with an 8.6-fold increased surgical difficulty of ERM removal compared to focal adherence ( P < .0001). The presence of fibrillary changes between the ERM and RNFL also correlated with a 25.5-fold increased difficulty of surgical removal compared to the absence of fibrillary changes ( P < .0001).
Conclusion
Extent of ERM-retinal adhesion and presence of fibrillary changes determined by SD-OCT provide reliable preoperative assessment of surgical difficulty. Furthermore, SD-OCT analysis may help localize surgically advantageous coordinates to initiate ERM removal.
Epiretinal membranes (ERMs) cause distortion of the retina and vision loss. Initial classifications of these membranes include the classic work by Gass. Ophthalmoscopic grading includes early disease, also termed grade 0 or cellophane maculopathy, in which a sheen from the inner retinal surface is observed with no distortion. This is followed by grade 1 or crinkled cellophane maculopathy, when membrane contraction causes small irregular folding of the inner retina surface. Gass emphasized fine superficial radiating folds that can be seen extending from membrane epicenters. Grade 2 includes an opaque or semi-opaque membrane causing significant vessel dragging. More recently, optical coherence tomography (OCT) has allowed visualization of membranes and their relationship to the retinal surface. However, the predictive value of OCT and clinical examination for surgical planning and for determining ease or difficulty of surgical removal remains unclear.
Time-domain OCT studies have shown that primary epiretinal membranes are more often adherent “globally” to broad areas of the retina, as opposed to membranes that occur after retinal breaks or detachment, which are more often focally adherent. More recently, spectral-domain optical coherence tomography (SD-OCT) analysis of epiretinal membranes has allowed determination of points of adhesion and relationships of the epiretinal membrane to the internal limiting membrane with a higher degree of detail. Although SD-OCT allows better definition of the geometry of membrane adhesion to the retina and it is suggested that membranes may be globally or focally adherent, ERM structure may not correlate with vision. Since the treatment of vision distortion from ERMs is surgical, correlation of ERM-retinal adherence with degree of surgical difficulty may aid in surgical planning.
In this study, we evaluated preoperative structural characteristics of epiretinal membranes including extent of retinal adhesion and presence of fibrillary changes using SD-OCT. These structural findings were correlated with ease or difficulty of surgical removal by reviewing surgical videography using masked observers.
Methods
Surgical difficulty and extent of ERM-retinal adhesion was evaluated in a consecutive series of eyes (N = 31) undergoing idiopathic macular ERM removal. Inclusion criteria included visual acuity of 20/50 or worse or metamorphopsia. All patients underwent a 3-port 25-gauge pars plana vitrectomy with core vitrectomy and posterior hyaloid removal. Epiretinal membranes were removed with or without triamcinolone (TCA) dusting (400 mg/mL) or indocyanine green (1.25 mg/mL) as a negative stain during a period of 8 months performed by a single experienced retinal surgeon. Since the surgeon was masked to preoperative OCT findings, the quadrant to initiate ERM peeling was randomized and peeling was performed using an ILM forceps tip (Revolution; Grieshaber, Fort Worth, Texas, USA). The intended surgical plane was to remove the epiretinal membrane without removal of the internal limiting membrane. Epiretinal membranes with a known etiology of uveitis, diabetic retinopathy, and previous retinal tears or detachments were excluded. Epiretinal membranes with lamellar macular holes were also excluded. Informed consent was obtained from all participants.
Surgical videography was recorded using an AVI adaptor mounted on a surgical microscope (Leica Microsystems, Wetzlar, Germany). Images were acquired using a 640 × 480 pixels digital video camera (Sony 3 CCD ExwaveHAD, Tokyo, Japan) mounted onto the surgical microscope. Digital feed was recorded directly onto a computer hard drive at DV resolution (Apple Macbook, Apple Computer, Cupertino, California, USA). Surgical videos were reviewed by 2 observers masked to preoperative SD-OCT imaging. Each masked observer was an experienced retinal surgeon and did not participate in ERM removal in this series of eyes. Degree of difficulty of membrane removal was determined for each quadrant of the macula and foveal area (total 5 areas per eye) following consensus by both reviewers. A grading scale (grade 1-3) was assigned according to surgical difficulty as follows: grade 1, peeling occurs easily with no evidence of retinal traction; grade 2, some evidence of retinal traction but retina retracts quickly following membrane removal; grade 3, appreciable retinal traction is observed with difficulty in ERM separation from the retina and retina remains elevated after ERM removal.
SD-OCT images (Spectralis OCT, Heidelberg Engineering, Vista, California, USA) of ERM structure along the vertical and horizontal meridians over the fovea (central 1000 μm) and macular quadrants (superior, inferior, nasal, and temporal) were also evaluated in a masked fashion by 2 observers. Thus, each eye was evaluated in a total of 5 areas (fovea, 4 quadrants). Both vertical and horizontal scanning meridians were obtained for each macular quadrant and foveal area was assessed for extent of ERM-retinal adhesion as well as for the presence of fibrillary changes along both vertical and horizontal scanning meridians. Calipers were used to measure the length of ERM-retinal adherence and divided by the total length of ERM to obtain ERM-retinal adhesion percentage. The extent of ERM-retinal adhesion was then categorized as focal, broad, or complete. Focal adhesion was defined as ERM-retinal adhesion <50%; broad adhesion between 50% and 90%; and complete adhesion >90%.
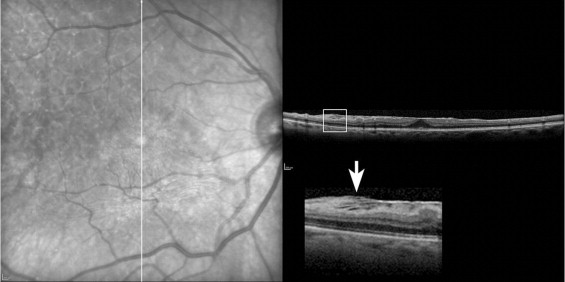
Fibrillary changes were defined as the presence of alternating linear hyperreflective and hyporeflective signals observed by SD-OCT extending between the ERM and retinal nerve fiber layer (RNFL) that were not parallel to the retinal surface ( Figure 1 ). Fluorescein angiography was performed preoperatively in all eyes to exclude choroidal neovascularization or other non-ERM pathology.
All analyses used generalized estimating equations to account for intra-eye variations (the SAS system, Generalized Estimated Equations [GEE] analysis).
Results
ERM-retinal adherence pattern resulted in complete concordance (kappa = 1) in each quadrant between the horizontal and vertical meridians for each observer. In addition, assessment of ERM-retinal adherence resulted in an extremely high concordance between masked observers (kappa = 0.9178). Therefore, categorization of ERM-retinal adherence by 1 observer was used for statistical analysis.
Among 31 consecutive eyes, ERM-retinal adherence pattern was evaluated preoperatively in a total of 149 areas since no evidence of an ERM was seen in 6 areas. The mean age of our patients in this study (female =14, male = 17) was 67.8 ± 11.4 years. Complete ERM-retinal adherence was observed in the majority of areas (86/149) evaluated ( Table ). The presence of fibrillary changes was similarly distributed among all quadrants in 13 patients.
| Characteristics | Fovea (N) | Nasal (N) | Temporal (N) | Superior (N) | Inferior (N) | Total (N) |
|---|---|---|---|---|---|---|
| Focal | 2 | 3 | 1 | 6 | 12 | 24 |
| Broad | 2 | 13 | 9 | 8 | 7 | 39 |
| Complete | 26 | 13 | 20 | 15 | 12 | 86 |
| Fibrillation (+) | 2 | 4 | 2 | 6 | 8 | 22 |
| Fibrillation (−) | 28 | 25 | 28 | 23 | 23 | 127 |
Surgical difficulty of ERM removal was also evaluated in the same 149 areas. ERM tissue was easily removed over 59 areas with no evidence of retinal traction (grade 1) ( Figure 2 and Supplemental Video 1 [available at AJO.com ]). Difficult ERM removal (grade 3) ( Figure 3 and Supplemental Video 2 [available at AJO.com ]) was observed in 46 areas with appreciable retinal traction and retinal elevation. Intermediate difficulty in surgical removal (grade 2) of ERM tissue was observed in 44 areas. A partial-thickness retinal defect occurred during ERM removal in 1 case over a single quadrant in which the presence of fibrillary changes was noted preoperatively. No other complications occurred.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


