Options for Refractive Surgery
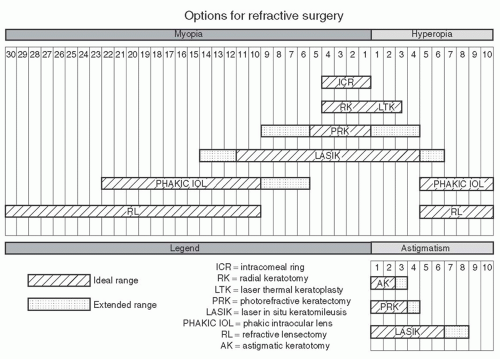
Before discussing the results of the various studies on refractive surgery, it is first necessary to provide a brief outline of each of the procedures available in the armamentarium of the refractive surgeon and the indications for each procedure (see
Fig. 5.1). The reader should note that the indications for each refractive procedure are rapidly changing as new technologies become available and replace other procedures.
LASIK and
photorefractive keratectomy (PRK) remain the mainstay of the armamentarium of refractive surgery. For PRK, the ideal treatment for maximum spherical myopia is -6.0 D (extended range up to -10.0 D). For LASIK, the ideal treatment for maximum myopia treatment is now -10.0 D (extended range -12.0 D). Other factors that influence the amount of correction include corneal thickness, flap thickness, pupil size, and the amount of ocular aberrations. Mitomycin-C (MMC) is used intraoperatively with higher myopic PRK,
1 and after more than a decade, MMC has been found to be effective when used for the prevention and treatment of corneal haze.
1,2 The limits of the hyperopic corrections have been reduced because of regression and disturbances in night vision associated with the smaller postoperative hyperopic optical zones noted with corrections over +3.0 D spherical equivalent.
Cochrane reviews of PRK versus LASIK for myopia and hyperopia have been conducted. For myopia, the effectiveness of these two procedures is comparable, but LASIK gives faster visual recovery than PRK.
3 For hyperopia, no robust, reliable conclusions could be reached, but the nonrandomized trials reviewed resulted in comparable efficacy for either procedure.
4 High-quality, well-planned open randomized control trials are needed in order to obtain a more robust base of clinical evidence.
Custom wavefront PRK and LASIK are now being performed for the same refractive range as conventional LASIK. Currently, wavefront treatments are available for up to -11.0 D of myopia and -4.0 D of astigmatism. Custom wavefront procedures have not consistently demonstrated superiority in terms of visual acuity and low aberration outcomes when
compared with conventional LASIK and PRK; however, the induction of higher order aberrations is reduced.
5
Laser epithelial keratomileusis (LASEK) is a hybrid of PRK and LASIK. LASEK utilizes an epithelial flap created by exposing the cornea to ethanol. Proponents of LASEK believe that it reduces the risk of intraoperative flap complications and preserves posterior corneal stroma. Critics are concerned about the slow visual recovery and the risks of corneal haze. However, numerous reported studies have shown quicker visual recovery and reduced postoperative pain levels after LASEK than after PRK.
6 A recent meta-analysis of studies involving LASEK versus PRK concluded that LASEK-treated eyes had no significant benefits over PRK-treated ones with regard to clinical outcomes, but there was less corneal haze observed with LASEK-treated eyes at 1 to 3 months after surgery.
7
Epi-LASIK is a variation of LASEK. For epi-LASIK, the epithelial flap is created with a modified microkeratome or femtosecond laser. Proponents state that the flaps created with Epi-LASIK heal faster and the results are comparable to LASIK, although no randomized clinical trials have been conducted to confirm these claims.
In 2005, it was estimated that nearly 70% of all LASIK patients in the United States chose to have the procedure performed with the femtosecond laser, if given the option.
8 Early comparisons between the femtosecond laser and the microkeratome in LASIK flap creation showed that the femtosecond laser group had significantly more diffuse lamellar keratitis postoperatively and the microkeratome
group had significantly more epithelial defects intraoperatively.
9 Earlier femtosecond lasers required higher total energy to cut a flap.
10 Morphologic alterations in the corneal stroma produced by the currently available models of the IntraLase (Abbott Medical Optics Inc., Santa Ana, CA) laser are comparable to those produced by mechanical microkeratomes.
10 Advances have resulted in a reduction in the total amount of energy delivered by the laser when it cuts the flap, and there is a decrease in the inflammatory response associated with femtosecond flap formation to the point that it is indistinguishable from the microkeratome at the cellular level.
10 Current models of the femtosecond laser, the 150 kHz IntraLase machine, can create a flap in about 10 seconds. This is half the time that was required by the previous 60 kHz system.
The improved results of faster visual recovery and uncorrected visual acuity (UCVA) and enhanced safety profile, including less post-LASIK dry eye, have led to most surgeons choosing the femtosecond laser for flap creation.
11,12,13 A systematic review concluded that while LASIK with the IntraLase femtosecond laser may offer limited benefit over LASIK with microkeratomes in regard to safety and efficacy, it has advantages in predictability of target refraction and flap thickness.
14Conductive keratoplasty (CK) has been approved by the U.S. Food and Drug Administration (FDA) for the treatment of hyperopia.
15 The thermal corneal burns are applied with a radiofrequency probe down to about 90% of the corneal depth (500 µm). It is hoped that the deeper corneal penetration will help avoid the problems with regression associated with laser thermal keratoplasty (LTK).
16,17 CK is no longer performed by most refractive surgeons; however, it is occasionally used to create “blended vision” in one eye for the correction of presbyopia.
Intracorneal rings (ICRs) or
Intacs (Contact Addition Technology, Des Plaines, IL) are now rarely used to treat myopia but have been applied for specific situations to treat post-LASIK ectasia
18 or keratoconus.
19 While the initial ICR FDA studies were promising,
20 the procedure never gained widespread acceptance because of the inability to treat astigmatism, difficulty in duplicating the initial FDA results, competition from LASIK, and the high explantation rate.
Phakic intraocular lenses (IOLs) and
refractive lensectomy (RL) remain the main options for the correction of extreme ametropias. Advances in
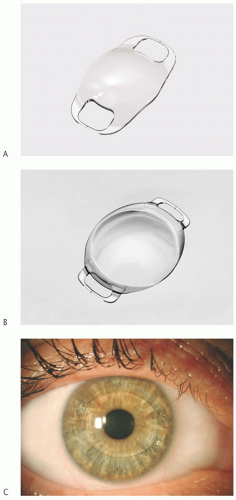
phakic IOLs include the Verisyse™ lens (Abbott Medical Optics Inc., Santa Ana, CA), also known as the Artisan® lens outside of the United States, that clips onto the iris stroma in the anterior chamber (
Fig. 5.2). The U.S. FDA clinical trials have shown that the Verisyse phakic IOL provides excellent refractive outcomes, with endothelial cell loss within a mean of 5.0% over 3 years, or 1.8% per year, and few complications.
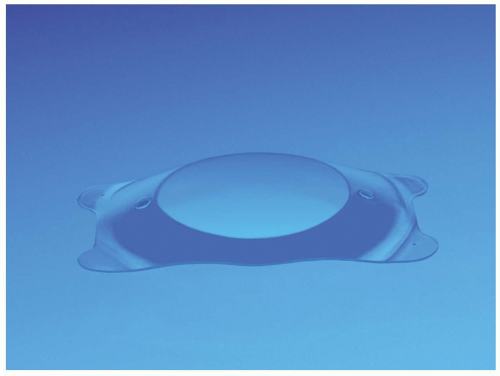
21 Another phakic IOL that is currently awaiting FDA approval is the Alcon (Fort Worth, TX) angle-supported Acrysof CACHÉ lens (
Fig. 5.3).
22 The Visian ICL (implantable collamer lens, Staar Surgical, Monrovia, CA) is implanted behind the iris in the posterior chamber and was U.S. FDA approved in 2005 (
Fig. 5.4).
23,24
RL, also known as
clear lens extraction (CLE) for myopia, has benefited from the availability of low diopter power IOLs; however, concerns about the increased risk of retinal detachment remain.
25 RL for hyperopia has used pig-gyback IOLs for eyes requiring heavy corrections
26; however, high-power customized foldable IOLs (e.g., up to 60.0 D CT Xtreme D, from Carl Zeiss Canada Ltd., Toronto, Ontario, not yet FDA approved) may make this less necessary in the future.
Multifocal, accommodating, and diffractive IOLs such as the ReZoom, previously Array (AMO, Santa Ana, CA), Crystalens, previously AT-45 (Eyeonics, Aliso Viejo, CA), and the ReSTOR IOL (Alcon Laboratories, Fort Worth, TX) have been under development for over two decades. Several modifications have been made to improve distance, intermediate, and near vision compared with their predecessors. Unfortunately, these modifications have also resulted in unwanted side effects such as glare and halos, decreased contrast sensitivity in multifocal lenses, and inconsistent nearvision results in accommodating IOLs. Careful patient selection is crucial for successful results.
27
Femtosecond laser cataract surgery has recently arisen in the forefront of refractive cataract surgery. There are four platforms approved by the FDA at the time of preparing this manuscript, including the LensAR (LensAR Inc., Winter Park, FL), LenSx (Alcon Laboratories, Fort Worth, TX), Catalys Precision Laser System (OptiMedica Corp., Sunnyvale, CA), and the VICTUS Laser System (Bausch & Lomb/Technolas
Perfect Vision, Munich, Germany). Various functions “depending on the machine” have received U.S. FDA approval (corneal incisions, astigmatic keratotomies, capsulorhexis, nucleus fragmentation or softening). The LenSx laser was the first to receive FDA approval and in initial studies, femtosecond laser lens fragmentation on grade 3 and 4 cataracts resulted in a 43% reduction in phacoemulsification power and a 51% decrease in effective phacoemulsification time.
28 In the initial series of procedures performed on human eyes, femtosecond laser capsulotomy and lens fragmentation was complete with no operative complications.
28 When compared with manual capsulorhexis for IOL implantation, femtosecond laser capsulotomy formation improved the predictability of the effective lens position.
29 Much additional study is underway to determine if femtosecond laser-assisted cataract surgery will significantly improve the refractive outcomes of cataract surgery.
Radial keratotomy (RK) is no longer performed,
30 as other refractive procedures offer a more predictable and stable outcome. For RK, a diamond knife was used to create radial incisions in the cornea.
LTK is no longer performed for low hyperopia, and the bankruptcy of the laser manufacturer officially ended its tenure. For LTK, peripheral thermal burns were applied to the peripheral cornea for the correction of small degrees of hyperopia.
LASIK, PRK, LASEK, and epi-LASIK are the main methods for the treatment of astigmatism. Astigmatic keratotomy and limbal relaxing incisions are generally used in conjunction with
other intraocular procedures to partially reduce astigmatism. The limits for the treatment of astigmatism by PRK, LASEK, or LASIK have been expanded by utilizing the cross-cylinder ablation or bitoric ablation technique originally proposed by Vinciguerra et al.
31 Toric pseudophakic and phakic IOLs are also available for the treatment of astigmatism associated with lens implantation.
32