Purpose
To report a series of 4 recurrent orbital varices after resection, 2 of which were embolized with cyanoacrylate glue before surgery.
Design
Retrospective case series.
Methods
Charts of all patients seen by a single orbital surgeon from January 1986 through June 2013 with presumed or histologically confirmed orbital varix were reviewed retrospectively. Four patients were identified with recurrence of symptoms after resection of the varix, 2 after embolization with n-butyl cyanoacrylate and 2 via a right frontal craniotomy. Each had initial complete resolution of their symptoms followed by recurrence to a lesser degree. Characteristics and common features in each case were reviewed.
Results
After initial resection, these 4 patients had recurrence of their symptoms within 8 months to 12 years. A common feature among them included an active lifestyle involving significant heavy lifting.
Conclusions
Orbital varices may be recurrent, even after n-butyl cyanoacrylate embolization, with repeated Valsalva-type maneuvers.
Orbital varices are distensible venous malformations. The classic presentation is an intermittent exophthalmos, typically brought on by elevation of venous pressure of any cause, including the Valsalva maneuver, posture-related factors, and coughing. Resting, ipsilateral enophthalmos of the affected side can be seen with long-term follow-up. Proptotic episodes may be associated with a deep orbital pain. Although most of these lesions can be observed, recurrent progressive pain and thrombosis may be an indications for intervention. Preoperative determination of the extent of the lesion and intraoperative hemostasis can be quite challenging. Embolization with cyanoacrylate glue followed by surgical excision has been reported previously to facilitate excision. To date, 2 patients at our institution have undergone primary resection of their varix via a craniotomy approach, and 9 patients underwent an orbital varix treated with n-butyl cyanoacrylate embolization and immediate postembolization resection. We report 4 recurrences despite prior resection; 2 of these patients underwent embolization before surgery with n-butyl cyanoacrylate and 1 of them was included previously in a case series (Patient 1).
Methods
We retrospectively reviewed the charts of all patients treated by a single orbital surgeon (J.A.G.) from January 1986 through June 2013, with presumed or histologically confirmed orbital varix. The patients were identified using a personal surgical log. Informed consent was obtained from all patients for all treatment. This retrospective study was performed with the approval of the Mayo Clinic Institutional Review Board and was conducted in accordance with the tenets of the Declaration of Helsinki. Charts were reviewed for intervention, time to recurrence, history of physical activity, and location of recurrence. A presumptive diagnosis of an orbital varix was made based on history consistent with positional or Valsalva-induced pain or proptosis, objective increase in exophthalmos in a dependant position, and imaging consistent with a varix, in most cases including a computed tomography scan with and without Valsalva or prone and supine positioning. All patients who had undergone an initial debulking of their orbital varix and demonstrated recurrence were reported. The procedure used for embolization with n-butyl cyanoacrylate under fluoroscopy and DynaCT (Siemens AG, Berlin, Germany) guidance has previously described been.
Results
Between January 1986 and June 2013, 17 patients were seen with a presumptive diagnosis of orbital varix and 11 patients with histologically confirmed orbital varix. Two patients underwent exploration for diagnostic purposes and varix was confirmed. Another 2 patients underwent resection of their varix via a craniotomy approach, followed by late recurrence, both managed with embolization and resection through a lateral orbitotomy. Seven of the lesions initially were embolized with n-butyl cyanoacrylate followed by resection via an appropriate orbitotomy approach. Of the 7 who initially underwent embolization and resection, 2 have demonstrated symptomatic recurrence, 1 of whom has undergone a second embolization and resection procedure. The 5 patients underwent percutaneous embolization without known recurrence with an average follow-up of 4.9 years (range, 4.4 to 5.5 years). The remaining 17 patients were observed. The characteristics and intervention for patients with recurrence of their symptoms are summarized in the Table .
| Patient No. | Age (y) | Sex | Location | Preoperative Symptoms | First Intervention | Symptoms with Recurrence | Second Procedure | Time from Primary Procedure to Recurrence |
|---|---|---|---|---|---|---|---|---|
| 1 | 18 | M | Superior nasal | Pain, proptosis | Superomedial orbitotomy with intraoperative embolization and excision | Pain, recurrent proptosis | None to date | 8 mos |
| 2 | 43 | M | Inferior | Pain, proptosis, diplopia | Percutaneous embolization, lateral orbitotomy with bone flap | Lower eyelid filling with discomfort | Percutaneous embolization, inferior swinging eyelid orbitotomy | 5 y |
| 3 | 29 | M | Inferior apex | Pain, proptosis | Right frontal craniotomy | Pain, proptosis | Percutaneous embolization, lateral orbitotomy | 12 y |
| 4 | 33 | F | Inferior lateral orbit and lateral rectus | Pain, proptosis | Left frontal craniotomy | Pain | Percutaneous embolization, lateral orbitotomy | 18 y |
All 4 patients with recurrence of their symptoms were young and physically active because of their occupation or athletics; 3 were disabled because of pain, and 1 experienced recurrent eyelid filling and discomfort ( Table ). Two of the patients initially underwent varix resection via a frontal craniotomy and orbitotomy, and the other 2 patients underwent varix embolization with n-butyl cyanoacrylate followed by immediate surgical resection via an appropriate orbitotomy approach. Each patient experienced transient postoperative diplopia with extreme gaze, but demonstrated resolution of all other symptoms and resolution of the Valsalva-induced proptosis. They were able to resume their active lifestyles. The 4 patients showed recurrence of symptoms, all to a much milder extent than the original lesion, between 8 months and 18 years after surgery. A common feature among these patients included a lifestyle involving frequent heavy lifting. One patient reported filling of his lower eyelid without pain when performing pushups. A second patient experienced recurrent proptosis and pain with weight lifting in particular. The third patient installed heavy granite countertops and experienced episodes of pain and proptosis while lifting. The fourth patient is an avid long distance runner who also lifts weights daily; her symptoms began to recur during prolonged exertion while running or on the elliptical training device.
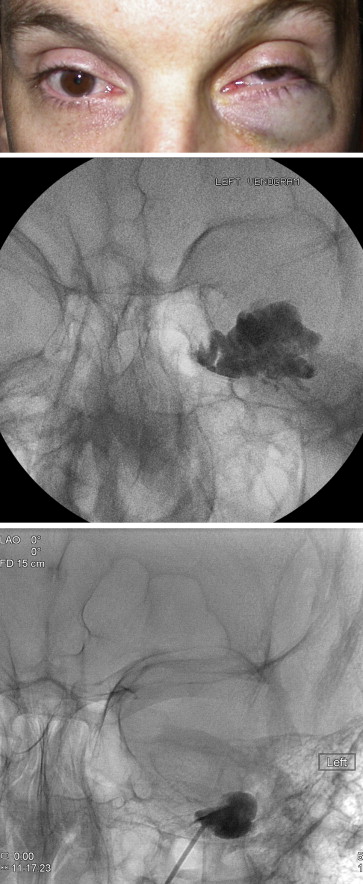
Three of the four patients with recurrence underwent a second procedure involving percutaneous embolization with n-butyl cyanoacrylate immediately followed by an appropriate orbitotomy approach to debulk the embolized vascular mass. Review of imaging revealed the recurrence to be immediately adjacent to, but not in the exact same area as, the initial distention and debulking ( Figures 1 and 2 ). Short-term follow-up (mean, 137 days; range, 19 to 186 days) of the 3 patients who underwent a second procedure revealed resolution of their positional and Valsalva-induced symptoms without further complications.