Purpose
To compare the clinical outcomes of the EX-PRESS glaucoma filtration device placed under a partial-thickness scleral flap with trabeculectomy.
Design
Randomized, prospective, multicenter trial.
Methods
A total of 120 eyes in 120 subjects were analyzed, including 59 eyes treated with EX-PRESS and 61 eyes treated with trabeculectomy. Both the EX-PRESS and the trabeculectomy groups were treated intraoperatively with mitomycin C and followed postoperatively for 2 years. Surgical success was defined as 5 mm Hg ≤ intraocular pressure ≤ 18 mm Hg, with or without medications, without further glaucoma surgery.
Results
Mean intraocular pressure was significantly reduced compared with baseline in both groups ( P < 0.001). Average intraocular pressure and number of medications were similar in both groups during follow-up, with mean intraocular pressure at 2 years after surgery of 14.7 ± 4.6 mm Hg and 14.6 ± 7.1 mm Hg in the EX-PRESS and trabeculectomy groups, respectively ( P = 0.927). At 2 years after surgery, the success rate was 83% and 79% in the EX-PRESS and trabeculectomy groups, respectively ( P = 0.563). Although visual acuity (logMAR) was significantly decreased on day 1 in both groups, the vision was not significantly different compared with baseline at 1 month after EX-PRESS implant ( P = 0.285) and 3 months after trabeculectomy ( P = 0.255). The variance of early postoperative intraocular pressure values was similar between groups on the first postoperative day but higher after trabeculectomy compared with EX-PRESS implant on day 7 ( P = 0.003). The total number of postoperative complications was higher after trabeculectomy than after EX-PRESS implantation ( P = 0.013).
Conclusions
Mean intraocular pressures, medication use, and surgical success were similar at 2 years after treatment with the EX-PRESS device and trabeculectomy. Vision recovery between groups was also similar throughout the study, although return to baseline vision was more rapid in the EX-PRESS group. Intraocular pressure variation was lower during the early postoperative period, and postoperative complications were less common after EX-PRESS implantation compared with trabeculectomy.
The EX-PRESS glaucoma filtration device (Alcon Laboratories, Fort Worth, Texas, USA) is a small, nonvalved implant that lowers intraocular pressure (IOP) by shunting aqueous humor from the anterior chamber into the subconjunctival area near the limbus. In the earliest clinical procedure for implantation, the device was inserted under the conjunctiva through full-thickness sclera, which was associated with erosion through the conjunctiva, hypotony, and other adverse effects. Subsequent modification of the procedure has decreased complications by placing the device under a partial thickness sclera flap, which provides resistance to aqueous outflow and reduces the risk for conjunctival erosion. The procedure is an alternative to trabeculectomy in the clinical management of patients with glaucoma. However, unlike trabeculectomy, no sclerectomy is performed during placement of the EX-PRESS device under a partial-thickness scleral flap. Also, although surgeons may or may not routinely perform iridectomy during their trabeculectomy surgeries, iridectomy is not performed during implantation of the EX-PRESS device under a partial-thickness scleral flap.
Several retrospective and small prospective studies have compared the results of EX-PRESS implantation and trabeculectomy. In this multicenter, prospective, randomized study, our purpose was to compare clinical outcomes after trabeculectomy with outcomes following EX-PRESS glaucoma filtration implant placed under a partial-thickness scleral flap.
Methods
This was an investigator-initiated, randomized, prospective, multicenter clinical trial of eyes treated with the EX-PRESS glaucoma filtration device or trabeculectomy, with a 2-year postoperative follow-up period (sites listed in Supplemental Table at AJO.com ). The institutional review board’s (IRB’s) review was prospective, and the protocol was approved by the IRB at each institution ( Supplemental Table at AJO.com ). The protocol conformed to the requirements of the United States Health Insurance Portability and Privacy Act (HIPPA). In addition to standard consent for surgery, written informed consent was obtained from all participants to participate in the research study before their entry to the study. The trial was registered with http://clinicaltrials.gov (identifier NCT00444080 ).
The EX-PRESS glaucoma filtration device is intended to reduce IOP in patients with glaucoma in whom medical and conventional surgical treatments have failed. Individuals older than 18 years of age who required primary glaucoma surgery were considered candidates for the study. Eligible subjects were diagnosed with open-angle glaucoma (including primary open-angle glaucoma, pseudoexfoliation glaucoma, and pigmentary glaucoma); had been treated with ocular hypotensive medications; were candidates for glaucoma surgery with intraoperative mitomycin C; and had IOP ≥18 mm Hg. Subjects were included if they had histories of laser trabeculoplasty or cataract phacoemulsification surgery, and the treatment had occurred at least 2 months prior to the study. Subjects were excluded if they had diagnoses of angle-closure glaucoma, normal tension glaucoma, or neovascular glaucoma. Additional exclusion criteria included history of previous incisional glaucoma surgery, penetrating keratoplasty, extracapsular cataract extraction, visually significant cataract planned for extraction at the time of filtering surgery or within 12 months thereafter, any significant ocular disease or history in the operated eye other than glaucoma and cataract, ocular pathology that could interfere with accurate IOP measurements, vitreous present in the anterior chamber for which vitrectomy is anticipated, and participation in any other concurrent ophthalmic clinical trial.
After the subjects had signed informed consent forms, baseline evaluation was performed, including measurement of visual acuity and IOP, anterior segment and fundus examination, and visual field examination. At all visits, the IOP was measured using Goldmann applanation tonometry, recording the mean of 2 measurements or, when measurements differed by more than 2 mm Hg, the median of 3 measurements. Randomization was performed separately for each study site. Each subject was assigned a 3-digit identifying number, and all subjects were randomized using a computer-based random-number generator to undergo treatment with EX-PRESS glaucoma filtration implant under scleral flap or trabeculectomy, both with intraoperative mitomycin C (0.25 mg/mL for 1 to 2 minutes, with the exact exposure time left to the discretion of the site investigator). Site investigators were required to have experience with at least 5 previous cases using the EX-PRESS implant prior to the study, and they were provided with standardized descriptions of the procedures. The EX-PRESS implant was a model P-50, implanted through a 25-gauge needle incision. Site investigators were not masked to the treatment received by the subjects.
After surgery, subjects were followed for 2 years. Postoperative follow-up visits included days 1 and 7 (days 7 through 14 accepted for this visit); and months 1 (± 7 days), 3 (± 14 days), 6 (± 21 days), 12 (± 30 days), 18 (± 30 days), and 24 (± 30 days). Additional visits were performed and recorded as required for the management of the subjects’ conditions, according to the site investigators. Results of all visits were recorded on standardized case-report forms. Primary outcome measures were mean IOP, medication reduction, and surgical success. Secondary outcome measures were logMAR vision, early postoperative (initial 2 weeks after surgery) IOP, and surgical complications. There were no differences in primary outcome measures among the study sites. Adverse events were reported by site investigators on the report forms as well as on separate adverse-event forms. All serious adverse events were reported to the site’s IRB according to their guidelines.
The early postoperative period was defined as the first 2 weeks after surgery. Success was defined as 5 mm Hg ≤IOP ≤18 mm Hg on 2 consecutive visits, with or without medications and without further glaucoma surgery. Subjects with IOPs that measured outside of this range on 2 consecutive visits (scheduled or unscheduled) were classified as failures. Hypotony was defined as intraocular pressure <5 mm Hg. Laser suture lysis, needling of the bleb, 5-fluoruracil injection, anterior chamber reformation, and bevacizumab injection were not considered as treatment failures. Best-corrected Snellen visual acuity measurements were converted to the logMAR scale values prior to statistical analysis. A target sample size of 60 in each group was calculated so as to allow detection of a 2–mm Hg difference of IOP between groups, with an expected standard deviation of 4 mm Hg, at a power of 0.80. The study was powered to detect a difference in IOP between the 2 groups, which was a primary outcome measure. Previous studies of IOP following EX-PRESS implant vs trabeculectomy have shown conflicting results. In order to detect differences in complication rates between the 2 groups, a substantially larger sample size would have been required. Statistical consultation and review were provided by the University of Virginia School of Medicine, Department of Public Health Sciences, Division of Biostatistics. Comparisons were performed using the unpaired t test for continuous variables and the χ 2 , Fisher exact, and comparison of proportions (z) test for categorical data. Success was analyzed using Kaplan-Meier survival analysis curves and the Gehan-Wilcoxon test. Variance of IOP was calculated in the early postoperative period and compared using the Brown-Forsythe test of equal variance. P values of <0.05 were considered statistically significant.
Results
The EX-PRESS device was implanted under a scleral flap in 59 eyes of 59 patients, and trabeculectomy was performed in 61 eyes of 61 patients, for a total of 120 eyes in 120 patients in the per-protocol analysis. In this study, 134 eyes were screened for eligibility, but 7 patients did not qualify for the study due to exclusion criteria and 6 patients withdrew consent. One subject was deemed eligible for the study and was randomized to receive treatment but was withdrawn from the study by the investigator prior to surgery because of thin sclera. Subjects were enrolled over a 21-month period at 7 sites, and enrolled subjects were followed for 2 years. There were no statistically significant differences between groups in baseline characteristics, including age, gender, self-identified race, lens status, previous laser therapy, glaucoma diagnosis, visual acuity (logMAR), preoperative IOP, or number of glaucoma medications ( Table 1 ).
| EX-PRESS n = 59 (100%) | Trabeculectomy n = 61 (100%) | P value | |
|---|---|---|---|
| Age, years (mean ± SD) | 69.4 ± 11.6 | 67.8 ± 10.4 | 0.428 |
| Range, years | 42.8–88.7 | 49.3–89.4 | |
| Gender, male/female, n (%) | 32 (54.2)/27 (45.8) | 33 (54.1)/28 (45.9) | 0.867 |
| Race, African-American/Caucasian/ a Other, n (%) | 30 (50.8)/25 (42.4)/4 (6.8) | 36 (59.0)/20 (32.8)/5 (8.2) | 0.555 |
| Eye, right/left, N (%) | 22 (37.3)/37 (62.7) | 31 (50.8)/30 (49.2) | 0.191 |
| Lens status, N (%) | |||
| Phakic | 34 (57.6) | 35 (57.4) | 0.612 |
| Aphakic | 0 (0.0) | 1 (1.6) | |
| Pseudophakic | 25 (42.4) | 25 (41.0) | |
| Previous glaucoma surgery, n (%) | 0 (0) | 0 (0) | 1.000 |
| Previous Laser therapy, n (%) | |||
| Laser trabeculoplasty | 29 (49.2) | 31 (50.8) | 0.994 |
| Laser iridotomy | 3 (5.1) | 4 (6.6) | 0.969 |
| Glaucoma diagnosis, n (%) | |||
| Primary open-angle glaucoma | 53 (89.8) | 56 (91.8) | 0.923 |
| Pseudoexfoliation glaucoma | 5 (8.5) | 4 (6.6) | |
| Pigmentary glaucoma | 1 (1.7) | 1 (1.6) | |
| Preoperative IOP (mm Hg), mean ± SD | 25.1 ± 6.0 | 26.4 ± 6.9 | 0.274 |
| Range, mm Hg | 18.5–44.5 | 18–45 | |
| Preoperative number medications, mean ± SD | 3.1 ± 1.1 | 3.1 ± 1.2 | 1.000 |
| Range | 0–5 | 0–5 | |
| Preoperative visual acuity (logMAR), mean ± SD | 0.30 ± 0.46 | 0.25 ± 0.35 | 0.503 |
| Range | −0.10–2.40 | 0.00–2.40 |
a Other included 2 Asian and 2 American Indian in the EX-PRESS group and 1 Asian, 3 American Indian, and 1 Hispanic in the trabeculectomy group.
During the surgical procedures, the conjunctival flap was fornix-based in 37 eyes (62.7%) and 29 eyes (47.5%) or limbal-based in 22 eyes (37.3%) and 32 eyes (52.5%) for the EX-PRESS implant and trabeculectomy procedures, respectively ( P = 0.110). There were more complications in patients treated with fornix-based compared with limbal-based flaps ( P = 0.013); however, there was no significant difference in complication rates in the EX-PRESS group and the trabeculectomy group in complications resulting from the type of conjunctival flap ( P = 0.713, Fisher exact test). Mitomycin C (0.25 mg/mL) was applied intraoperatively in 57 eyes (96.6%) treated with the EX-PRESS implant and 61 eyes (100%) treated with trabeculectomy. The average time of exposure of mitomycin C was 1.8 ± 0.5 minutes during EX-PRESS implantation and 1.7 ± 0.4 minutes during trabeculectomy ( P = 0.228). Viscoelastic was used in 17 eyes (28.8%) during the EX-PRESS procedure and in 11 eyes (18%) during trabeculectomy ( P = 0.227). Analysis of eyes treated with viscoelastic during surgery showed no statistically significant differences in mean IOP in the 2 groups. The mean ± standard deviation number of sutures used to close the partial-thickness scleral flap was 2.9 ± 1.4 during EX-PRESS implantation and 2.9 ± 0.9 during trabeculectomy ( P = 1.000).
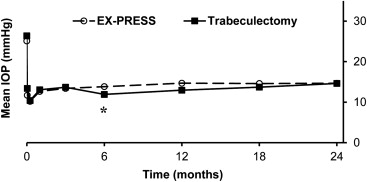
As shown in Figure 1 , the mean pre- and postoperative IOPs were similar at in both groups. The mean ± SD baseline (preoperative) IOP was 25.1 ± 6.0 mm Hg in the EX-PRESS group and 26.4 ± 6.9 mm Hg in the trabeculectomy group ( P = 0.274). In both groups, the mean IOP was significantly lower compared with baseline IOP at all time points after surgery ( P < 0.001). During the postoperative period, there were no significant differences in mean IOP between the 2 groups, except at the 6-month time point (13.8 ± 4.7 mm Hg after EX-PRESS and 11.9 ± 4.6 mm Hg after trabeculectomy, P = 0.027). At 2 years after surgery, the mean ± SD IOP was 14.7 ± 4.6 mm Hg after EX-PRESS implantation and 14.6 ± 7.1 mm Hg after trabeculectomy ( P = 0.927). Longitudinal regression analysis showed no statistically significant differences in the IOP curves after treatment with the EX-PRESS device and trabeculectomy (repeated measures ANOVA, P = 0.330).
The mean number of glaucoma medications pre- and postoperatively is shown in Figure 2 . There was a significant decrease in the number of medications required after surgery compared with before surgery in both groups ( P < 0.001), and there were no significant differences between the groups at any time point in the study. At baseline, the average ± SD number of medications was 3.1 ± 1.1 in the EX-PRESS group and 3.1 ± 1.2 in the trabeculectomy group ( P = 1.00). At 2 years after surgery, the EX-PRESS implant group required an average of 0.9 ± 1.3 medications, compared with 0.7 ± 1.2 medications for the trabeculectomy group ( P = 0.383). Longitudinal regression analysis showed no significant difference in the number of glaucoma medication curves after treatment with EX-PRESS and trabeculectomy (negative binomial generalized estimating equation model ANOVA, P = 0.490).
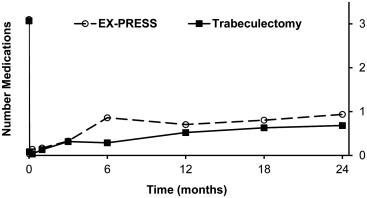
Figure 3 shows the pre- and postoperative visual acuity (logMAR) in both groups. The visual acuity in the EX-PRESS and trabeculectomy groups, respectively, was 0.3 ± 0.46 and 0.25 ± 0.35 at baseline ( P = 0.503), and 0.28 ± 0.28 and 0.37 ± 0.39 at 2 years after surgery ( P = 0.150). Visual acuity was significantly reduced from baseline ( P < 0.001) at day 1 in both groups and recovered (was not significantly different from baseline) at 1 month in the EX-PRESS group ( P = 0.285) and 3 months in the trabeculectomy group ( P = 0.255), with no significant differences compared with baseline for the remaining time points. Comparisons between the groups undergoing EX-PRESS implant or trabeculectomy were not statistically significantly different at any time points in the study. Survival analysis showed a significant difference in the time to return to baseline vision after EX-PRESS implantation compared with trabeculectomy (log rank, P = 0.041). According to the Turnbull-Kaplan-Meier estimation, the median time for return to baseline vision was 0.7 months (95% CI: 0.03 to 1.6 months) after EX-PRESS device implantation and 2.2 months (95% CI: 0.9 to 5.2 months) after trabeculectomy.
The survival analysis is shown in Figure 4 , with success defined as 5 mm Hg ≤IOP ≤18 mm Hg, with or without medications and without additional glaucoma surgery. Surgical success was 90% and 87% at 1 year, and 83% and 79% at 2 years in the EX-PRESS and trabeculectomy groups, respectively ( P = 0.563). The reason for surgical failure was increased IOP in all instances, with no patients classified as failure due to hypotony. Thirteen subjects had further glaucoma surgery, including 5 subjects in the EX-PRESS group and 8 subjects in the trabeculectomy group (11 subjects had glaucoma drainage implant surgery, 1 had surgical revision, and 1 had trabeculectomy). In the EX-PRESS and trabeculectomy groups, respectively, the number of eyes remaining in the analysis was 59 and 60 at 1 year, and 57 and 57 at 2 years. In the EX-PRESS and trabeculectomy groups, there were 2 and 4 subjects, respectively, lost to follow-up (2 subjects in the EX-PRESS group and 3 subjects in the trabeculectomy group died during the follow-up period). Additional survival analyses, using different thresholds for elevated IOP, showed similar results ( Supplemental figures at AJO.com ). Success of achieving IOP ≤21 mm Hg was 92% and 92% at 1 year, and 86% and 84% at 2 years after EX-PRESS implantation and trabeculectomy, respectively ( P = 0.747). IOP ≤15 mm Hg was achieved in 73% and 70% at 1 year, and 58% and 56% at 2 years after the EX-PRESS procedure and trabeculectomy, respectively ( P = 0.401).
During the early postoperative period (first 2 weeks after surgery), IOP was measured before any treatment (initial-visit IOP values), and after laser suture lysis, removal of releasable sutures, or digital massage (final-visit IOP value). The IOP measurements on days 1 and 7, before and after any treatment, are shown in a Figure 5 , top. As shown in Figure 5 , bottom, the variance in both initial and final IOP measurements on postoperative day 7 was significantly lower after EX-PRESS implant under scleral flap compared with trabeculectomy ( P = 0.003 and 0.039, respectively). A total of 8 subjects (13.6%) in the EX-PRESS group and 11 subjects (18.0%) in the trabeculectomy group developed hypotony during the early postoperative period ( P = 0.682).



