Purpose
To investigate clinical characteristics of Purtscher-like retinopathy and its clinical implications among patients with systemic lupus erythematosus (SLE).
Design
Observational case series.
Methods
setting : Tertiary medical center. patient population : Patients with SLE who were diagnosed with Purtscher-like retinopathy between 2002 and 2013. observation procedures : Assessment and follow-up in the ophthalmology department. main outcome measure : Visual acuity and funduscopic examination at presentation and at 6 month follow-up, with analysis of the association between Purtscher-like retinopathy and other systemic involvement of SLE and overall disease activity.
Results
Among 5688 patients with SLE evaluated, 8 cases of Purtscher-like retinopathy were diagnosed. Typical fundus abnormalities included Purtscher flecken, cotton-wool spots, retinal hemorrhages, macular edema, optic disk swelling, and a pseudo–cherry red spot. Fluorescein angiography abnormalities included areas of capillary nonperfusion corresponding to the retinal whitening, late leakage, peripapillary staining, precapillary occlusion, and slower filling of vessels. The prevalence of central nervous system lupus was significantly higher among those with Purtscher-like retinopathy (6/8) than among 240 patients randomly sampled from those without Purtscher-like retinopathy. A very high SLE Disease Activity Index (≥20) was present in all 8 patients with Purtscher-like retinopathy. All patients received corticosteroids combined with immunosuppressants. For the majority of patients, optic atrophy developed during follow-up with persistent low visual acuity.
Conclusion
As a rare and severe ophthalmic complication of SLE, Purtscher-like retinopathy was associated with central nervous system lupus and highly active disease. Visual acuity recovery was usually poor despite prompt treatment.
Purtscher retinopathy is characterized by a sudden loss of vision with bilateral or unilateral patches of retinal whitening and hemorrhage around the optic nerve and in the posterior pole in patients who have suffered from severe trauma, especially of the head and thorax. Cases not associated with trauma are known as “Purtscher-like retinopathy.” Commonly reported causes of Purtscher-like retinopathy include acute pancreatitis, renal failure, and autoimmune disease.
Systemic lupus erythematosus (SLE) is an autoimmune inflammatory disease that mainly affects women of childbearing age and involves multiple organ systems. Retinal abnormalities are found in 3% of well-controlled patients to 29% of patients with more active systemic disease. Purtscher-like retinopathy has rarely been described in the literature as a complication of SLE or as a distinct category of severe retinal vaso-occlusive disease in SLE. The pathogenesis of Purtscher-like retinopathy associated with SLE is not fully understood.
As a national referral center of rheumatic diseases, our hospital receives a high volume of patients with SLE and provides routine ocular evaluation for patients admitted. The purpose of this study was to describe the clinical characteristics of Purtscher-like retinopathy among patients with SLE and to investigate its clinical implications.
Methods
This study was an observational case series performed between January 1, 2002 and December 31, 2013 at a tertiary medical center. The ophthalmologic evaluation records of 5688 SLE patients admitted during the study period were reviewed. Eight patients were diagnosed with Purtscher-like retinopathy and were included in the study. The study was approved by the institutional review board of Peking Union Medical College Hospital. All data with patient-specific information were securely handled and de-identfied prior to analysis.
The diagnosis of SLE was based on 1982 American College of Rheumatology (ACR) criteria, which requires at least 4 of the following 11 criteria: malar rash, discoid rash, photosensitivity, oral ulcers, nonerosive arthritis, serositis, renal dysfunction, neurologic derangements (ie, seizures or psychosis), hematologic disorder (ie, anemia, leukopenia, thrombocytopenia), immunologic disorder (ie, anti-DNA antibody, and anti-Sm antibody), and presence of antinuclear antibodies. Purtscher-like retinopathy was defined as the presence of Purtscher flecken and cotton-wool spots (typically restricted to the posterior pole) with or without a low to moderate number (1–10) of retinal hemorrhages. Purtscher flecken are multiple distinctive polygonal patches of retinal whitening with an area of normal or clear retina between the retinal whitening and adjacent arterioles. These characters distinguish Purtscher flecken from the confluent retinal whitening seen in proximal occlusion of the retinal arteries and cotton-wool spots resulting from distal occlusion of the retinal capillaries, which are superficial and feather-shaped lesions with irregular borders that can obscure the blood vessels in the underlying retina. For all cases enrolled, other potential causes of Purtscher-like retinopathy were evaluated and ruled out.
The demographic and clinical information of included patients were extracted from medical records, including age, sex, and ocular and systemic examination results. Patients were followed every 3 months until the ocular condition was stable or the patient died. Those who missed their clinical appointments were contacted by phone. Ophthalmologic examinations included best-corrected visual acuity (VA) at diagnosis and follow-up, intraocular pressure, slit lamp, binocular indirect ophthalmoscopy, fundus fluorescein angiography (FFA), and optical coherence tomography (OCT). In addition, 1 patient underwent ultrasound of the eye and indocyanine green angiography (ICGA) and another patient had fundus autofluorescence (FAF) imaging.
Additional data collected included clinical manifestations that frequently occur in SLE patients, including skin rashes, photosensitivity, ulcers, arthritis/arthralgia, serositis, nephritis, and neurologic disorders. Laboratory data consisted of complete blood counts, urinalysis, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), complement, and antibody measurements, including antinuclear antibodies (ANA), anti–extractable nuclear antigen (ENA) antibodies, and antiphospholipid antibodies (APLA). Central nervous system (CNS) lupus was diagnosed by the presence of clinical manifestations (seizure, psychosis, organic brain syndrome, cerebrovascular accident, intractable headaches, and myelopathy), in combination with neurologic evaluations including cerebrospinal fluid (CSF) and brain magnetic resonance imaging (MRI) in the majority of patients. Lupus nephritis was defined as the presence of proteinuria or cellular casts containing red blood cells and hemoglobin. Disease activity was measured using the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) developed in 2000, categorized as no activity (SLEDAI = 0), mild activity (SLEDAI = 1–5), moderate activity (SLEDAI = 6–10), high activity (SLEDAI = 11–19), and very high activity (SLEDAI ≥20).
To evaluate the correlation between Purtscher-like retinopathy and other clinical characteristics of SLE, particularly CNS lupus, 240 control patients were randomly selected from all SLE patients without Purtscher-like retinopathy admitted during the study period, stratified by sex and 2 age categories (<18 years and ≥18 years). For patients with multiple admissions during the study period, only the first admission was included. In addition, secondary comparisons were performed on a smaller set of variables (age, sex, diagnosis of CNS lupus and lupus nephritis during hospitalization) using data available from the electronic medical record that included all patients without Purtscher-like retinopathy.
For ophthalmologic evaluations, descriptive statistical analysis was based on the number of eyes. Wilcoxon rank-sum test was used to compare variables measured on a continuous scale (eg, age, SLEDAI). Fisher exact test was used to compare categorical variables between groups (eg, sex and CNS lupus). Data were analyzed using Stata 12.0 (Stata Corp, College Station, Texas, USA). All hypothesis testing was 2-sided, with α level of 0.05.
Results
Characteristics and Clinical Course of Systemic Lupus Erythematosus–Associated Purtscher-like Retinopathy
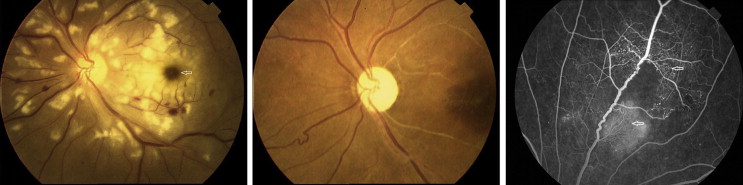
Among 5688 patients evaluated, 8 patients (7 women, 1 man) were diagnosed with Purtscher-like retinopathy. The overall prevalence of Purtscher-like retinopathy was 0.14%. The median age was 23.5 years (range: 8–39 years). The median time of follow-up was 13 months (range: 3 days–11 years). For all patients, both eyes of all the patients were involved and therefore were included in the analysis. All the patients reported blurring vision. Ophthalmic examination of anterior segments was normal in all eyes. On funduscopic examination, the most frequently encountered signs were Purtscher flecken and cotton-wool spots, which occurred in 16 of 16 eyes (100%) ( Figure 1 , Left, and Figure 2 , Left), followed by retinal hemorrhages (15/16, 94%). Other common findings included macular edema (13/16, 81%), optic disk swelling (12/16, 75%), and a pseudo–cherry red spot (7/16, 44%) ( Figure 2 , Left).
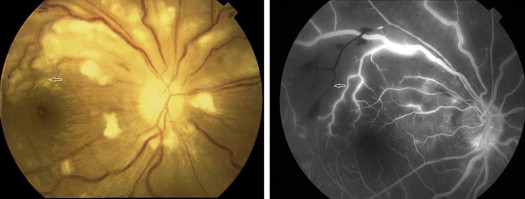
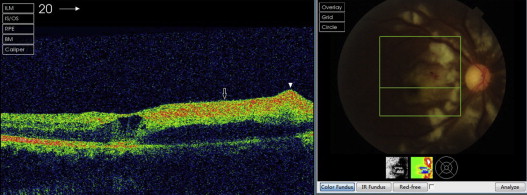
FFA was performed in 7 cases (1 patient died on day 3 of admission and was not evaluated) and showed areas of capillary nonperfusion corresponding to Purtscher flecken (14/14, 100%), late leakage (14/14, 100%), peripapillary staining (10/14, 71%), precapillary occlusion (10/14, 71%), and slower filling of vessels (9/14, 64%) ( Figure 1 , Right). OCT was performed in 7 cases and showed a hyperreflective area in the retinal nerve fiber layer (RNFL) in 14 eyes (14/14, 100%) and retinal edema in 10 eyes (10/14, 71%) ( Figure 3 ). ICGA performed in 1 case at presentation demonstrated intense hyperfluorescence in the posterior poles in the early phase, which faded with time and showed diffusely weak choroidal hyperfluorescence ( Figure 4 , Left). FAF imaging showed patchy hypoautofluorescence corresponding to Purtscher flecken ( Figure 4 , Right).
All patients received corticosteroids with initial dose ranging from 55 to 1000 mg/day, combined with immunosuppressants including cyclophosphamide or methotrexate. One patient died of acute respiratory failure at day 3. At 6 months of follow-up, VA of 7 patients was measured. VA was better than 20/40 in 4 eyes, between 20/200 and 20/40 in 4 eyes, and worse than 20/200 in 6 eyes. Funduscopic examination in these patients revealed optic atrophy (10/14, 71%), mottling of the retinal pigment epithelium (5/14, 36%) ( Figure 2 , Middle), and normalization of the retinal appearance (3/14, 21%). In cases with several signs, the most frequent combination was optic atrophy and mottling of retinal pigment epithelium. The eyes with pseudo–cherry red spots and total optic atrophy had poor VA. Two eyes of 1 patient developed retinal detachment at 9 months follow-up and underwent vitrectomy in both eyes. Retinal neovascularization developed in 2 eyes at 6 months and in 1 eye at 9 months follow-up ( Figure 2 , Right). Only 1 eye received retinal laser treatment.
Association Between Purtscher-like Retinopathy and Other Systemic Involvement of Systemic Lupus Erythematosus
Among 8 patients with Purtscher-like retinopathy, 6 (75%) were diagnosed as having CNS lupus. Symptoms of CNS lupus included seizure (3/6, 50%), headache (2/6, 33%), psychosis (2/6, 33%), cognitive dysfunction (1/6, 17%), cerebrovascular disease (1/6, 17%), and myelopathy (1/6, 17%). Antibodies to ribosomal P, which were highly associated with CNS lupus, were positive in 4 patients (4/8, 50%), including 1 patient without CNS manifestations. CSF evaluation was performed in all patients, which showed elevated levels of cell counts and total protein in 1 patient (1/8, 13%) and elevated opening pressure in 3 patients (3/8, 38%). MRI revealed multiple discrete white matter lesions in periventricular areas and/or frontal lobes in 3 patients, and cortical atrophy in 1 patient. All 8 patients had a SLEDAI above 20 at admission, indicating highly active disease.
Compared to the control group randomly selected from patients without Purtscher-like retinopathy, patients with Purtscher-like retinopathy had significantly higher prevalence of CNS lupus (75% vs 19%, P = .001) ( Table ). Several manifestations of CNS lupus were more common in the group with Purtscher-like retinopathy than in the control group, including seizure (38% vs 8%, P = .03), psychosis (25% vs 6%, P = .09), and headache (25% vs 5%, P = .06). The median SLEDAI at admission among patients with Purtscher-like retinopathy was significantly higher than that of the control group (26 vs 12, P = .001). The prevalence of nephritis was not different between groups. The prevalence of antiphospholipid antibodies including lupus anticoagulant (LA), anticardiolipin (aCL), and anti-β 2 -glycoprotein (anti-β 2 -GPI) was not different between groups. In addition, using data abstracted from the electronic medical record, the prevalence of CNS lupus and lupus nephritis were compared with the prevalence in all patients without Purtscher-like retinopathy and showed similar results ( Table ).
| Characteristics | Patients With Purtscher-like Retinopathy (n = 8) | Patients Randomly Selected From Inpatients Without Purtscher-like Retinopathy (n = 240) | P a | All Inpatients Without Purtscher-like Retinopathy b (n = 5680) | P c |
|---|---|---|---|---|---|
| Age, median years | 23.5 | 29 | .07 | 30 | .07 |
| Female sex | 7 (88) | 209 (87) | 1.0 | 4962 (87) | 1.0 |
| CNS lupus | 6 (75) | 45 (19) | .001 | 1164 (20) | .001 |
| Seizure | 3 (38) | 19 (7.9) | .03 | ||
| Psychosis | 2 (25) | 14 (5.8) | .09 | ||
| Cognitive dysfunction | 1 (13) | 21 (8.6) | .53 | ||
| Cerebrovascular accident | 1 (0) | 2 (0.8) | 1.0 | ||
| Headache | 2 (25) | 11 (4.6) | .06 | ||
| Myelopathy | 1 (13) | 1 (0.4) | .06 | ||
| Nephritis | 6 (75) | 122 (51) | .28 | 3244 (57) | .48 |
| Antiphospholipid syndrome | 0 (0) | 18 (7.5) | 1.0 | ||
| Antiphospholipid antibodies | |||||
| Lupus anticoagulant | 0 (0%) | 73/221 d (33) | .06 | ||
| Anticardiolipin | 3 (38%) | 76/217 d (35) | 1.0 | ||
| Anti-β2-glycoprotein | 0/5 d (0%) | 19/102 d (19) | .58 | ||
| SLEDAI, median | 25.5 | 12 | .001 | ||
| CRP or ESR elevation | 7 (88) | 165 (69) | .44 | ||
| Hypocomplementemia | 5 (63) | 153 (64) | 1.0 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


