Purpose
To characterize the microscopic anatomy of the lacrimal punctum and canaliculi in relation to the tarsal plate, muscle of Riolan, and Horner muscle; and to report a novel technique to excise the horizontal canaliculus in severe dry eye patients.
Design
Observational anatomic study and a retrospective case series.
Methods
The microscopic anatomy was studied in 86 eyelids of 25 cadavers (age range: 45–96 years, mean: 79.5 years). Surgery was performed on 18 canaliculi of 7 patients with dry eyes (age range: 37–69 years, mean: 59.9 years). In the microscopic study, 32 eyelids were incised sagittally, 38 eyelids were incised horizontally (1 mm from the eyelid margin), and 16 eyelids were incised parallel to the tarsal plate. All specimens were stained with Masson trichrome. In the surgical group, probe-guided horizontal canalicular excision with incision of the Horner muscle to the lateral edge of the lacrimal caruncle was performed. Both canalicular stumps were cauterized.
Results
In the microscopic anatomic study, the punctum and the vertical canaliculus were part of the tarsal plate with the muscle of Riolan, whereas the horizontal canaliculus was surrounded by the Horner muscle. In the surgical group, all the operated canaliculi were completely occluded without recanalization 12 months postoperatively. No complications were recorded.
Conclusions
Based on microscopic anatomic findings that the lacrimal punctum and the vertical canaliculus are part of the tarsal plate, and that the horizontal canaliculus is surrounded by the Horner muscle, excision of the horizontal canaliculus may be an effective technique to treat patients with severe dry eyes.
Surgical occlusion of the puncti is considered the last treatment option for patients with severe dry eyes. Although many of the reported techniques are usually efficacious, there are still cases of failure attributable to recanalization. Although the exact reason for such recanalization is not clear, understanding the anatomic relationships between the lacrimal punctum, lacrimal canaliculus, and the surrounding tissues is essential for a successful surgical punctal occlusion.
It was shown that the lacrimal punctum is encircled by a dense, sclerous fibrous tissue, which can occasionally generate a driving force that opens a surgically occluded punctum. Although the vertical canaliculus is also considered to be encircled by this thick fibrous tissue, the anatomy of this part of the lacrimal system was not studied in detail and so its role in recanalization is not clear.
Studies show that the muscle of Riolan passes in the tarsal plate and the dense fibrous tissue of the eyelid margin, and then inserts onto the lacrimal punctum and the vertical canaliculus. Another researcher postulates that the muscle of Riolan encompasses these parts of the lacrimal drainage system. Since the muscle of Riolan, the tarsal plate, and the dense fibrous tissue constitute the tight eyelid margin, revealing the exact extension of the muscle of Riolan over the lacrimal punctum and the vertical canaliculus may clarify whether these lacrimal portions are indeed tarsal components. Although the fibrous tissue around these parts of the lacrimal system was considered continuous with the tarsal plate, this is not supported by any anatomic studies.
The horizontal canaliculus is rarely targeted in lacrimal occlusion surgery. The horizontal canaliculus is surrounded by the Horner muscle ( Figure 1 , Top), which originates from the posterior lacrimal crest and runs convexly anterolateral to the tarsal plate. The muscle is continuous with the pretarsal part of the orbicularis oculi muscle and the muscle of Riolan. Since the Horner muscle has a major role in maintaining the lacrimal drainage process, any injury to this muscle or disruption of its function may result in epiphora. In cases of traumatic horizontal canaliculus laceration repair, postoperative epiphora can result even after successful reconstruction. In such cases, the cause may be injury and loss of function of the Horner muscle.
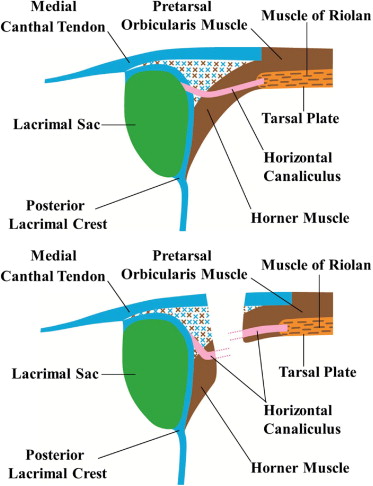
In patients with a recent canalicular laceration, it is often seen that the nasal stump of the canaliculus is tugged medially and posteriorly to the posterior lacrimal crest by the medial stump of the Horner muscle, whereas the temporal stump is pulled laterally and anteriorly by the lateral stump of the Horner muscle and the pretarsal orbicularis muscle. This results in the edges of each stump being pulled in opposite anteroposterior and horizontal directions. This is typically seen when the more nasal part of the canaliculus is involved ( Figure 1 , Bottom). We used this phenomenon to design a technique for surgical occlusion of the horizontal canaliculus in patients with dry eyes.
In this study, we examined the microscopic anatomy surrounding the punctum and canaliculus with special emphasis on their relations with the tarsal plate, muscle of Riolan, and Horner muscle. We also report the surgical outcome of our novel technique of excising the horizontal canaliculi in patients with severe dry eyes.
Methods
Microscopic Anatomic Study
Eighty-six eyelids (23 upper right, 23 upper left, 20 lower right, and 20 lower left) of 25 cadavers (mean age at death, 79.5 years; range, 45–96 years) were examined microscopically. None of the cadavers had a history or any clinical evidence of lacrimal or eyelid diseases. All specimens were fixed in 10% buffered formalin before use.
The method of removing and preparing the eyelid samples has been previously described.
Specimens for microscopic examination were then prepared from the removed tissues. Thirty-two eyelids (7 upper right, 9 upper left, 7 lower right, and 9 lower left) were incised sagittally at 10 mm and 5 mm lateral to the lacrimal punctum, at the level of the punctum, and 5 mm medial to the punctum. We examined the characteristics of the eyelid margin at each area. Thirty-eight eyelids (11 upper right, 8 upper left, 11 lower right, and 8 lower left) were incised horizontally at 1 mm from the eyelid margin (both in the upper and the lower eyelids). The relationships between the vertical lacrimal canaliculus, the fibrous tissue in the eyelid margin including the tarsal plate, and the muscle of Riolan were studied. Sixteen eyelids (5 upper right, 3 upper left, 5 lower right, and 3 lower left) were incised parallel to the tarsal plate to include the lacrimal punctum and the vertical canaliculus. The continuity between the fibrous tissue of the eyelid margin or the tarsal plate with the punctum, and the vertical and horizontal canaliculi was examined.
The specimens were dehydrated, embedded in paraffin, and cut into 7-μm-thick slices. These were stained with Masson trichrome. Photographs were taken with a digital camera system attached to a microscope (Moticam 2000; Shimadzu Rika Kikai, Tokyo, Japan). Photomerging was done with Adobe Photoshop CS2 software (Adobe Systems Co Ltd, Tokyo, Japan).
Interventional Study Group
We performed a retrospective chart review of all patients who underwent horizontal canalicular excision surgery for severe dry eyes between September 2, 2008 and April 28, 2010. Seven patients were included (5 eyes of 3 male patients and 8 eyes of 4 female patients; mean age, 59.9 years; range, 37–69 years) ( Table ). The degree of dryness was judged by a Schirmer test I (without topical anesthesia) and the decrease in tear meniscus height (TMH). All our patients failed insertion of punctal plugs as well as artificial eyedrops and sodium hyaluronate eyedrops. When the punctal plugs were inserted, the patients had clinical improvement with no significant epiphora; however, since the plugs constantly extruded, the patients remained symptomatic, and surgical intervention was required. Preoperatively, 1 patient had bilateral plugs in the upper puncti and another patient had a plug in the lower-right punctum. The other 5 patients had no punctal plugs.
| Preoperative (Right/Left) | Postoperative (Right/Left) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Patient | Sex | Age | Occluded Canaliculus | Diagnosis | TMH | A | D | TMH | A | D |
| 1 | M | 37 | Right-upper/-lower | GVH | 0.05 | 2 | 3 | 0.3 | 0 | 0 |
| 2 | M | 55 | Bilateral lower | Idiopathic | 0.1/0.1 | 2/2 | 3/3 | 0.2/0.2 | 0/0 | 0/0 |
| 3 | F | 60 | Bilateral lower | Idiopathic | 0.1/0.1 | 2/2 | 3/3 | 0.15/0.15 | 1/1 | 1/1 |
| 4 | M | 65 | Bilateral lower | Idiopathic | 0.1/0.1 | 2/3 | 3/2 | 0.15/0.15 | 1/1 | 1/1 |
| 5 | F | 66 | Bilateral-upper/-lower | Idiopathic | 0.05/0.05 | 3/2 | 2/3 | 0.15/0.15 | 0/0 | 0/0 |
| 6 | F | 67 | Bilateral-upper/-lower | OCP | 0.1/0.1 | 1/1 | 2/3 | 0.15/0.15 | 0/0 | 0/0 |
| 7 | F | 69 | Bilateral upper | Idiopathic | 0.1/0.1 | 2/2 | 2/2 | 0.2/0.2 | 1/1 | 1/1 |
All patients underwent surgery to remove part of the horizontal canaliculi. Some patients chose to spare 1 of the canaliculi. These patients had newly inserted plugs in the nonoperated puncti except the puncti already having plugs. Basically, the lower puncti were chosen for surgical occlusion. One patient, who already had a plug in the lower-right punctum, chose to undergo upper canalicular surgeries and insertion of a plug in the lower-left punctum.
Six months postoperatively, probing and irrigation was used to confirm complete obstruction of the operated canaliculi. In addition, we measured the TMH and the degree of superficial punctate keratopathy (SPK) preoperatively and 6 months postoperatively. TMH was measured in magnified slit-lamp photographs using a millimeter ruler. The AD classification (A: area; D: density) was used to quantify the degree of SPK after staining with topical fluorescein. The area of SPK was graded as A0 when there was no punctate staining, A1 when the staining involved less than one-third of the cornea, A2 when it involved one-third to two-thirds of the cornea, and A3 when the staining involved more than two-thirds of the cornea. The density of SPK was graded as D0 when there was no punctate staining, D1 when the density was sparse, D2 when the density was moderate, and D3 when the density was high and the lesions overlapped.
The paired t test was used to compare the TMH measurements and the Wilcoxon signed rank test was used to compare the AD scores. Statistical analysis was performed with SPSS II for Windows (SPSS Japan Inc, Tokyo, Japan). P < .05 was judged as statistically significant.
Results
Microscopic Anatomic Study
In the sagittal specimens incised 10 mm lateral to the punctum, the eyelid margin was composed of the tarsal plate and a dense fibrous tissue with the muscle of Riolan ( Figure 2 , Top left). Similar findings were demonstrated in the sagittal specimens incised 5 mm lateral to the punctum ( Figure 2 , Top right). The sagittal sections through the punctum demonstrated a dense fibrous tissue and the muscle of Riolan encircling the punctum and the vertical canaliculus. The vertical canaliculus was predominantly surrounded by the muscle of Riolan ( Figure 2 , Bottom left). The sagittal specimens incised 5 mm medial to the punctum showed that the horizontal canaliculus was encircled by the Horner muscle ( Figure 2 , Bottom right). Similar findings were demonstrated in both the upper ( Figure 2 ) and lower eyelids ( Figure 3 ) .
The horizontal sections incised 1 mm from the eyelid margin showed that the vertical canaliculus was completely surrounded by the muscle of Riolan ( Figure 4 ) . The conjunctival surface curved anteriorly just nasal to the vertical canaliculus, from which the fibrous tissue with the muscle of Riolan continued laterally without a demarcation. These tissues corresponded to the tarsal plate. Similar findings were demonstrated in both the upper ( Figure 4 , Top) and lower eyelids ( Figure 4 , Bottom).



