The optimal treatment of chordomas is maximal safe resection followed by radiation therapy. Data have shown that the use of protons has increased the local control of chordomas. Because of their physical properties, proton therapy has a sharp decline at its distal range, thereby minimizing collateral damage. However, this choice of radiation therapy has been limited based on the availability of resources. Given the high cost of proton facilities and improved techniques for other forms of radiation therapy, this article evaluates whether proton therapy is still superior to other radiation techniques in the treatment of chordomas.
Chordomas are rare tumors with an incidence of less than 0.1 per 100,000 per year. Originating from the remnant of embryonal notochord, such lesions can occur along the spinal axis, including the base of skull. Optimal treatment consists of maximal surgical resection followed by local radiation therapy. Given the increased experience with endoscopic skull-based techniques; improved instrumentation; and, when necessary, the use of arterially based mucosal flaps for cerebrospinal fluid leak closure, the ability to approach resections of these lesions has significantly improved. However, obtaining a complete surgical resection, given the anatomic constraints and infiltrative nature of the lesion, is challenging in this region. Accordingly, the role of radiation therapy in this location is ever important. Data have shown an increase in local control and survival with the use of proton therapy, although several radiation techniques have been used to improve local control. Although the senior surgeon (D.W.K) has had a patient with a 19-year disease-free period after combined endoscopic resection and proton therapy, the question arises whether, in the era of more modern techniques, the additional cost of proton therapy is validated by outcomes.
| EBM Question | Level of Evidence | Grade of Recommendation |
|---|---|---|
| Is proton beam therapy superior to other radiation techniques in patients with chordoma? | 4 | C |
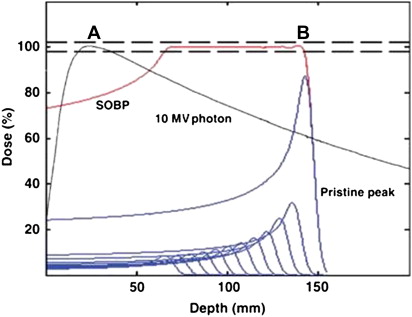
Radiation therapy can be delivered with several techniques. Most therapies use photons. The dose distribution of photons enters the body, delivers the dose, and then has a long tail dose ( Fig. 1 ). In the era of intensity-modulated radiation therapy (IMRT), the dose distribution of photons remained the same; however, technology in the linear accelerator allowed modulation of the photon beam. This modulation allowed better conformality (shaping of the dose to the tumor) around critical structures by using several beams or angles to deliver dose. However, this technology came at a price because the integral dose received by the body was greater than that in the 3-dimensional (3D) era.
Stereotactic radiation (photon) therapy involves immobilization and image guidance to decrease treatment margins and better spare normal tissue, all while delivering high doses in 1 to 5 treatment fractions. There are several delivery systems available, including the Gamma Knife (Elekta, Sweden) and the CyberKnife (Accuray, Sunnyvale, CA, USA). Given the increased number of beam angles available, conformality was greater with this technique, allowing delivery of high doses of radiation.
Proton beam therapy is a particle beam therapy that has a different dosimetric distribution of dose (see Fig. 1 ). Although the photon beam has a tail that delivers dose past the tumor target, the beam has a sharp steep falloff with no dose to tissues past the range of tumor. Theoretically, this falloff allows for delivery of high doses, yet allows sparing of tissue beyond the tumor. In the skull base, this feature is critical, given the critical structures at risk after treatment. The critical structures at risk include the optic nerves, optic chiasm, cranial nerves, cochlea, brainstem, pituitary gland, and temporal lobes. The goal of radiation therapy is to deliver high enough doses to the tumor while maintaining low dose to critical structures. The close proximity of the tumor to critical structures at the skull base makes this location one of the most difficult to treat.
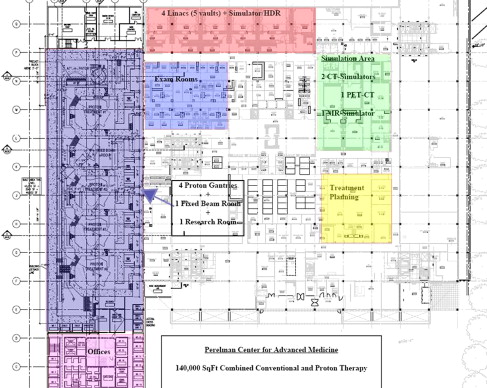
Because of the significant potential advantages of proton therapy, the University of Pennsylvania elected to invest in a proton facility (the Roberts Proton Therapy Center, Figs. 2 and 3 ). Such technology does not come cheaply, with a total investment of approximately $250 million ($140 million for the proton component and $110 million for the remaining radiation equipment, software, and facility). The cyclotron required to produce the proton beam weighs more than 250 metric ton, and, when combined with the system required to distribute the beam to the gantries; this occupies an area the size of a football field and is surrounded by 17 ft of shielding concrete. However, because proton therapy is frequently combined with conventional photon therapy, the Penn facility was designed with a unique advantage of having both modalities on the same site ( Fig. 4 ).

Early treatment of chordomas (1950–1980) with radiation therapy included photon radiation therapy delivered at a total dose of 55 Gy using conventional 2-dimensional techniques. In this early report, 25 patients treated had a freedom from progression of 32 months with an overall survival at 5 and 10 years of 44% and 17%, respectively. At Princess Margaret Hospital, the median survival was 62 months, with a pain response of 85% and a neurologic response of 45%. The median time to progression was 35 months, and, when the investigators examined the role of hypofractionated regimens, they found no benefit. The importance of a maximal safe resection was documented in a study from the Mallinckrodt Institute of 21 patients with chordoma. Although disease-free survival was not different among the groups reviewed, those with surgery alone compared with those with biopsy and radiation therapy had an improvement in the 10-year survival. The Mayo Clinic reviewed the role of postoperative radiation therapy after various surgical modalities and found an increase in disease-free survival and an increase in overall survival dependent on the extent of surgical resection (55% resection vs 36% for biopsy only). Multivariate analysis showed that younger age and diplopia were prognostic of longer survival.
Given the poor outcomes with photon therapy alone in the 1960s and 1970s, proton therapy was evaluated, with the first proton references in the literature regarding treating primary brain tumors appearing in the 1960s in murine models. Early work was done in skull base tumors, in which the benefit of proton therapy was best seen in chordomas and chondrosarcomas of the base of skull. Reports in 1982 showed that treatment of 10 patients with doses of 76 cobalt Gray equivalent (CGE) were feasible without significant morbidity. Massachusetts General Hospital (MGH) reported on the use of fractionated proton radiation therapy in 1989 in 68 patients who received postoperative radiation therapy at a median dose of 69 CGE, with a 5-year actuarial local control rate of 82% and disease-free survival of 76%. Some temporal lobe damage was reported by the same institution in 1998 in a study of 96 patients with chordomas and chondrosarcomas of the base of skull. All patients were treated with either 66.6 or 72 CGE with conventional fractionation. Ten patients developed temporal lobe damage with a cumulative damage incidence of 13.2% at 5 years. Despite the different temporal lobe damage rates related to age, tumor volume, number of surgical procedures before radiation therapy, and prescribed doses to the tumor, only gender was a significant predictor of damage ( P = .0155) using a univariate (log-rank) test. In a stepwise Cox regression that included gender as a variable, no other baseline variable improved the prediction of damage.
A review of cases at MGH published in 1999 showed a 10-year local control rate of combined proton-photon therapy that was highest for chondrosarcomas, intermediate for chordomas in men, and lowest for chordomas in women (94%, 65%, and 42%, respectively). A similar review at the Loma Linda University Medical Center in 58 patients with skull base chordomas and chondrosarcomas treated with total doses between 64.8 and 79.2 CGE showed local control rates of 92% for chondrosarcoma and 76% for chordomas. Actuarial 5-year survival rates were 100% for patients with chondrosarcoma and 79% for patients with chordoma. Grade 3 and 4 late toxicities (those requiring increased medical intervention or hospital admission, Table 1 ) were observed in 4 patients (7%) and were symptomatic in 3 patients (5%).
| Grade 1 | Mild, asymptomatic or mild symptoms, clinical or diagnostic observations only, intervention not indicated |
| Grade 2 | Moderate; minimal, local, or noninvasive intervention indicated; limiting age-appropriate instrumental activities of daily living |
| Grade 3 | Severe or medically significant but not immediately life-threatening, hospitalization or prolongation of hospitalization indicated, disabling, limiting self-care activities of daily living |
| Grade 4 | Life-threatening consequences, urgent intervention indicated |
| Grade 5 | Death related to adverse event |
The Centre de Protontherapie D’Orsay France treated 45 patients with a median total dose delivered within the gross tumor volume of 67 CGE (range, 60–70 CGE). With a mean follow-up of 30.5 months, the 3-year local control rates for chordomas and chondrosarcomas were 83.1% and 90%, respectively, and 3-year overall survival rates were 91% and 90%, respectively. Young age at the time of radiotherapy influenced local control positively ( P <.03) in univariate analysis but not in multivariate analysis. Only 2 patients presented grade 3 or 4 complications. A further review of 67 patients (including some cervical spine) treated showed 3-year local control rates of 71% and 85% for chordomas and chondrosarcomas, respectively, and 3-year overall survival rates of 88% and 75%, respectively. Once again, on multivariate analysis, only age was an independent prognostic factor of local control.
Although promising, given the limited availability of protons and the inability of many patients to travel long distances, there is clearly a need to consider other radiation options. In the 1980s, there were series published examining the role of brachytherapy in the treatment of chordomas. In patients requiring reirradiation, iodine 125 was used to treat 5 chordomas. Of the 5 patients, 3 had stable disease or regression of their disease. In treating recurrent clival chordomas with iodine 125, a dose of 40 Gy was given, and, although the patient numbers were small, there was a regression to tumor as well as symptomatic relief of symptoms.
In the 1990s, the era of 3D conformal photon therapy, an increase in dose to 66.6 Gy brought an increase in overall survival to 80%. Although these results were promising, around the same time, the increased use of stereotactic radiosurgery was heralding a new technique for the treatment of base of skull chordomas. The University of Pittsburgh documented a small series in 1991 using Gamma Knife radiosurgery in patients with recurrent chordomas after surgery alone. The volume was small (<3 cm), and a dose of 20 Gy was given at the tumor margin. With a mean follow-up of 20 months, two-thirds did not have progressive tumor, whereas one-third had a reduction in tumor size. Of the 6 patients, half had improvement in neurologic deficit, whereas the others remained stable.
The North American Gamma Knife Consortium recently published their review of 6 institutions treating base of skull chordomas with Gamma Knife radiosurgery as the primary, adjuvant, or salvage management. With a median follow-up of 5 years, of the 71 patients treated, 23 had died of tumor progression. Overall survival at 5 years was 93% for patients who had not received prior radiation therapy and 43% for those who had received prior therapy. Patients of younger age and with longer disease-free interval before Gamma Knife radiosurgery, no prior radiation therapy, less than 2 cranial nerve deficits, and small tumor volume were associated with a longer survival. Tumor control rate at 5 years was 69% in the group without prior radiation and 62% for those with prior radiation. As expected, older age, prior radiation therapy, recurrence, and large tumor volume were associated with worse tumor control. Most patients went on to get other modalities of therapy after Gamma Knife radiosurgery.
The use of CyberKnife for stereotactic treatment has introduced a new treatment technique particularly useful for chordomas when they occur in the spinal region, although there are literature reports also for its use in skull base lesions. These techniques are typically fractionated regimens (1–5 fractions) that facilitate treatment of larger tumors with high doses per fraction. As expected, patients with prior radiation therapy were at a higher risk of complications and poorer tumor control. In 18 patients treated with a median follow-up of 65 months, the local control was 59% and overall survival was 74%, with a disease-specific survival of 88.9%.
As 3D photon therapy continued to evolve, so did the software as well as technology for photon treatment delivery. Multiple institutions examined the role of IMRT in the treatment of chordomas and chondrosarcomas. However, there are several abstracts published that have examined the role of IMRT alone in the treatment of base of skull chordomas. IMRT offers the advantage of the ability to shape the dose around critical structures such as the optic apparatus and brainstem. To date, these have not been published in a full article form, likely because of short follow-up. However, IMRT also shows promise in providing local control. Although traditional proton therapy has been able to spare normal tissue via a “patching” technique, this is time consuming and laborious. Given the feasibility of IMRT and its widespread availability across the country, the need to consider IMRT as a treatment option is now surfacing more than ever.
As photon technology has evolved, so has the proton beam, and, in the next generation of treatment, the use of spot scanning (single pencil proton beams that can be modulated or conformed, ie, IMRT) to mimic current photon technique is taking precedence. The Paul Scherrer Institut, Switzerland, treated 29 patients with chordomas and chondrosarcomas using spot-scanning proton radiotherapy with a median dose of 74 and 68 CGE, respectively. With a median follow-up of 29 months, the 3-year local control rates were 87.5% and 100% for chordoma and chondrosarcoma, respectively. At 3 years, actuarial progression-free survival and overall survival was 90% and 93.8%, respectively. Actuarial 3-year complication-free survival was 82.2%. Radiation-induced pituitary dysfunction was observed in 4 (14%) patients (Common Terminology Criteria for Adverse Events grade 2). No patient presented with postradiation brainstem or optic pathway necrosis or dysfunction. In univariate analysis, age (≤40 years at the time of proton therapy) favorably affected the progression-free survival ( P = .09). An update in 2009 showed actuarial 5-year local control rates of 81% for chordomas and 94% for chondrosarcomas. Five-year rates of overall survival were 62% for chordomas and 91% for chondrosarcomas. High-grade late toxicity consisted of 1 patient with grade 3 and 1 patient with grade 4 unilateral optic neuropathy and 2 patients with grade 3 central nervous system necrosis. No patient experienced brainstem toxicity. Actuarial 5-year freedom from high-grade toxicity was 94%. These results compare favorably to those of other combined proton-photon therapy ( Table 2 ).



