Proliferative Diabetic Retinopathy: Clinical Trials
Dean Eliott MD
I. DIABETIC RETINOPATHY STUDY
Introduction
Eyes that develop proliferative diabetic retinopathy (PDR) have at least a 50% probability of becoming blind within 5 years without treatment.1,2,3 Retinal photocoagulation, introduced by Meyer-Schwickerath in 1960 with the xenon arc, appeared to have a beneficial effect on neovascularization; however, there was uncertainty as to its exact role.4 The xenon arc was used to treat patches of surface neovascularization directly, while the ruby laser and, subsequently, the argon laser, were used in the same manner as well as in an indirect scatter pattern. Results of several small clinical trials in the late 1960s suggested that photocoagulation might be a promising new treatment for retinal neovascularization.5 The Diabetic Retinopathy Study (DRS) was organized in the 1970s to determine the effect of photocoagulation on diabetic retinopathy. This was the first prospective, multicenter, randomized controlled trial (RCT) sponsored by the newly formed National Eye Institute of the National Institutes of Health. In addition to its historical importance, the DRS has contributed tremendously to our understanding of the role of photocoagulation in the management of PDR.6,7
Background and Study Questions
When the DRS was organized, visual loss from diabetic retinopathy was a growing public health problem. There was no consensus regarding the treatment of PDR and diabetic macular edema (DME), the two major causes of blindness in patients with diabetes. The DRS, which attempted to seek answers to an important public health issue, was unprecedented in its scope and size.
To describe fundus findings in a consistent manner, the DRS used a modified version of the Airlie House Classification of diabetic retinopathy.8 The original Airlie House Classification was developed in 1968 at a symposium where the most up-to-date knowledge of diabetic retinopathy was discussed. Despite a symposium among more than 50 international experts in retinal disease, the best approach for the management of diabetic retinopathy was unknown.9,10
It was in this historical context that the DRS was established. The DRS sought to determine whether photocoagulation (xenon or argon) was effective in the treatment of diabetic retinopathy. Specifically, it attempted to determine whether photocoagulation could prevent severe visual loss in eyes with PDR, whether there was a difference in safety and efficacy between xenon arc and argon laser, and whether certain stages of retinopathy demonstrated different responses to treatment.6,7
Patients Included in the Study
Approximately 1,750 patients with PDR in at least one eye or severe nonproliferative diabetic retinopathy (NPDR) in both eyes, and visual acuity of at least 20/100 in both eyes were enrolled.11
Severe NPDR was defined by the DRS as cotton-wool spots (see Fig. 7C.1), venous beading (see Fig. 7C.2), and intraretinal microvascular abnormalities (see Fig. 7C.3) in at least two of four contiguous photographic fields or two of these findings and moderately severe hemorrhages and/or microaneurysms
(see Fig. 7C.4) in at least one photographic field. There are seven standard 30-degree photographic fields (see Fig. 7C.5).8,11
(see Fig. 7C.4) in at least one photographic field. There are seven standard 30-degree photographic fields (see Fig. 7C.5).8,11
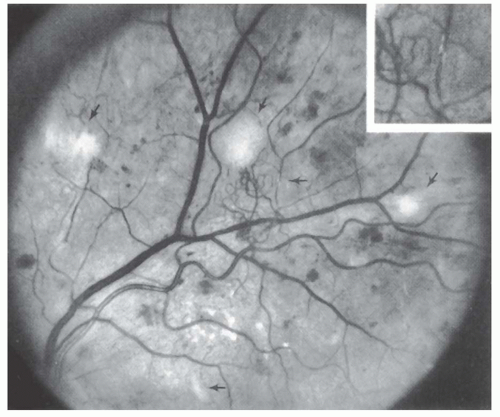 FIGURE 7C.1 Diabetic Retinopathy Study standard photograph 5, the more severe of two standards for soft exudates. There are four soft exudates (cotton-wool spots) in the upper half of this photograph: two (almost confluent) at the 9:30 position, one just above the center, and one at the 3 o’clock position. This photograph also shows hard exudates (lipid) below the center of the picture and a small segment of arteriolar sheathing (inset). Some of the abnormal vessels at the center of the photograph are intraretinal microvascular abnormalities and some are new vessels. (From Diabetic Retinopathy Study Research Group. A modification of the Airlie House Classification of diabetic retinopathy. DRS Report No. 7. Invest Ophthalmol Vis Sci. 1981;21(1): 210-226 and from Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs—an extension of the modified Airlie House Classification. ETDRS Report No. 10. Ophthalmology. 1991;98:786-806.)12 |
Neovascularization of the disc (NVD) was defined by the DRS as the presence of abnormal vessels on or within one-disc diameter of the optic disc (see Fig. 7C.6), and neovascularization elsewhere (NVE) as the presence of abnormal vessels located more than one-disc diameter from the disc (see Fig. 7C.7).
Intervention and Outcome Measures
One eye of each patient was randomized to receive treatment, either with the xenon arc or the argon blue-green laser, and the other eye served as a control and was observed without treatment. All treated eyes received both direct photocoagulation to surface neovascularization (NVE only) and scatter panretinal photocoagulation from the vascular arcades to beyond the equator (laser burns separated by one burn width). In addition, eyes randomized to argon laser treatment also had NVD treated directly only in the initial part of the study (this was not possible with xenon). Argon laser burns were generally smaller and less intense than xenon arc burns (see Fig. 7C.8).
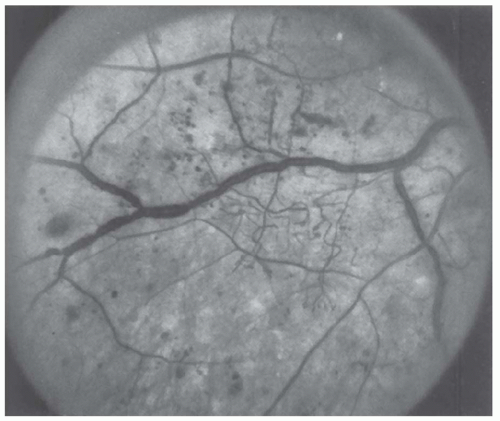 FIGURE 7C.2 Diabetic Retinopathy Study standard photograph 6B, more severe standard for venous beading. Most venous branches, both large and small, are involved by severe beading. (From Diabetic Retinopathy Study Research Group. A modification of the Airlie House Classification of diabetic retinopathy. DRS Report No. 7. Invest Ophthalmol Vis Sci. 1981;21(1):210-226 and from Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs—an extension of the modified Airlie House Classification. ETDRS Report No. 10. Ophthalmology. 1991;98:786-806.)12 |
Outcome measures included severe visual loss, defined as visual acuity less than 5/200 at each of two consecutive visits 4 months apart.
Major Findings
The DRS demonstrated a 50% reduction in severe visual loss in eyes that received photocoagulation (see Fig. 7C.9).13,14 This
finding was so impressive that the protocol was amended to allow the control group to receive photocoagulation.14
finding was so impressive that the protocol was amended to allow the control group to receive photocoagulation.14
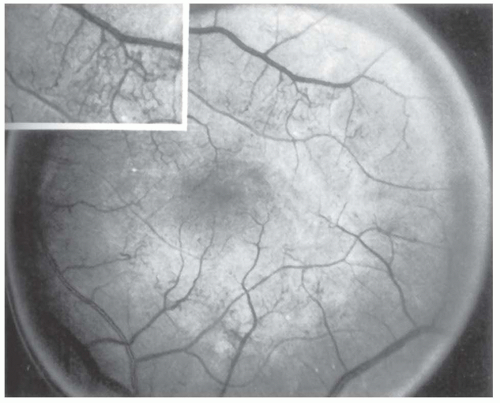 FIGURE 7C.3 Diabetic Retinopathy Study standard photograph 8B, more severe standard for intraretinal microvascular abnormalities (IRMA). This photograph shows IRMA in all quadrants. Inset shows IRMA superotemporal to the center of the macula. (From Diabetic Retinopathy Study Research Group. A modification of the Airlie House Classification of diabetic retinopathy. DRS Report No. 7. Invest Ophthalmol Vis Sci. 1981;21(1):210-226 and from Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs—an extension of the modified Airlie House Classification. ETDRS Report No. 10. Ophthalmology. 1991; 98:786-806.)12 |
The study also identified features that were associated with a particularly high risk of severe visual loss.14,15,16,17 These risk factors were based on the presence, location, and severity of neovascularization, as well as the presence of vitreous or preretinal hemorrhage. Specifically, these risk factors were defined as (a) the presence of new vessels; (b) the location of new vessels on or within one-disc diameter of the optic disc (NVD); (c) the severity of new vessels, defined for NVD as equal to or greater than one-fourth to one-third disc area in extent (equal to or greater than standard photograph 10A) (Fig. 7C.6),8 or for NVE, equal to or greater than one-half disc area; and (d) preretinal or vitreous hemorrhage. Eyes with at least three of these risk factors were considered to be at high risk for severe visual loss, and these eyes demonstrated the most benefit from photocoagulation (see Table 7C.1, Fig. 7C.10).
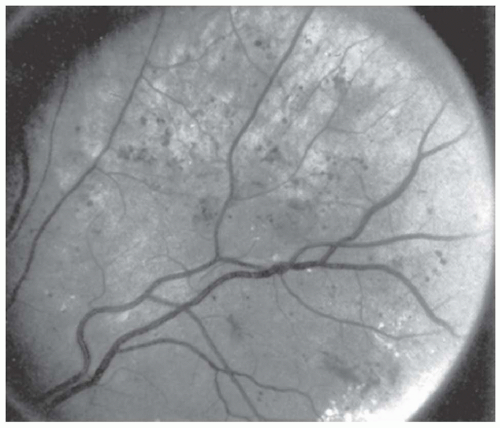 FIGURE 7C.4 Diabetic Retinopathy Study standard photograph 2B, severe standard for hemorrhages and microaneurysms. (From Diabetic Retinopathy Study Research Group. A modification of the Airlie house classification of diabetic retinopathy. DRS Report No. 7. Invest Ophthalmol Vis Sci. 1981;21(1):210-226 and from Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs—an extension of the modified Airlie House Classification. ETDRS Report No. 10. Ophthalmology. 1991;98:786-806.) |
After 2 years of follow-up in the DRS, severe visual loss occurred in 26% of eyes in the control group as compared with 11% in the treated group for eyes with high-risk characteristics (HRC). After 4 years, 44% of control eyes and 20% of treated eyes developed severe visual loss, and the unequivocal benefit of photocoagulation was substantiated in all additional reports with longer follow-up.18,19 Prompt photocoagulation was recommended for eyes with HRC.
For eyes with PDR and less than high-risk retinopathy, the risk of developing severe visual loss at 2 years was 7% for the control group and 3% for the treated group. For eyes with severe NPDR, these rates were even lower. The DRS did not recommend prompt treatment for these categories of eyes.
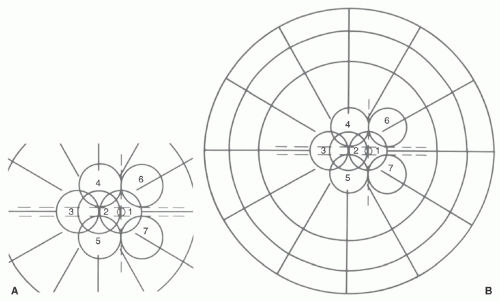 FIGURE 7C.5 Seven standard photographic fields of the modified Airlie House Classification shown for the right eye. Field 1 is centered on the optic disc; field 2 on the macula; field 3 temporal to the macula. Fields 4 through 7 are tangential to horizontal lines passing through the superior and inferior edges of the optic disc and to a vertical line passing through its center. (From Diabetic Retinopathy Study Research Group. A modification of the Airlie House Classification of diabetic retinopathy. DRS Report No. 7. Invest Ophthalmol Vis Sci. 1981;21(1):210-226 and from Olk RJ, Lee CM. Review of national collaborative studies. In: Diabetic Retinopathy: Practical Management. Philadelphia, PA: JB Lippincott Co; 1993:22.) |
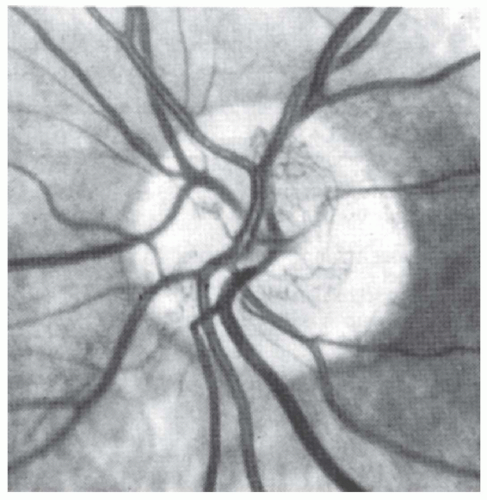 FIGURE 7C.6 Diabetic Retinopathy Study standard photograph 10A demonstrating neovascularization of the disc, one-fourth to one-third disc area in extent. (From Diabetic Retinopathy Study Research Group. Photocoagulation treatment of proliferative diabetic retinopathy: the second report of Diabetic Retinopathy Study findings. Am J Ophthalmol. 1978;85:82-106 and from Early Treatment Diabetic Retinopathy Study Research Group. ETDRS Report No. 10. Grading diabetic retinopathy from stereoscopic color fundus photographs—an extension of the modified Airlie house classification. Ophthalmology. 1991;98:786-806.) |
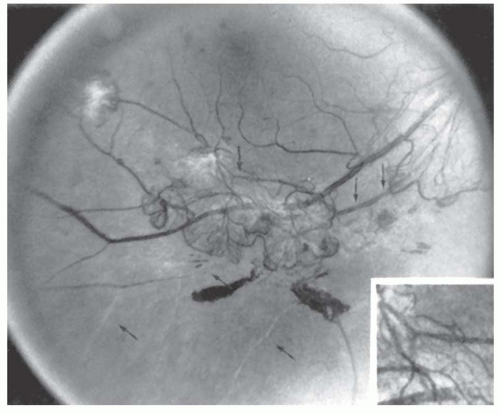 FIGURE 7C.7 Diabetic Retinopathy Study standard photograph 7 demonstrating the lower boundary of severe new vessels elsewhere. This photograph also shows new vessels within 1 disc diameter from the disc (neovascularization of the disc) in the upper right part of the picture, focal arteriolar narrowing, arteriolar sheathing, “white threads” (completely opaque arteriolar branches), and small preretinal hemorrhages. (From Diabetic Retinopathy Study Research Group. A modification of the Airlie House Classification of diabetic retinopathy. DRS Report No. 7. Invest Ophthalmol Vis Sci. 1981;21(1):210-226 and from Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs—an extension of the modified Airlie house classification. ETDRS Report No. 10. Ophthalmology. 1991;98:786-806.)12 |
Regarding the safety and efficacy of argon versus xenon photocoagulation, the DRS demonstrated that decreased visual acuity and constricted visual fields were more common in the xenon group. Persistent visual acuity loss of one line occurred in 19% of xenon-treated eyes as compared with 11% in the argon group; a loss of two or more lines occurred in 11% for xenon and 3% for argon. A modest loss of visual field (measured on Goldmann perimetry using the largest test object, IVe4) occurred in 25% of xenon-treated eyes as compared with 5% of argon-treated eyes; more severe field loss occurred in an additional 25% in the xenon group.14,18
Implications for Clinical Practice
The DRS conclusively demonstrated that photocoagulation was effective in the treatment of PDR, and the overwhelming benefit associated with treatment had important public health implications.
The DRS identified four retinopathy risk factors for severe visual loss in eyes with PDR that met the inclusion criteria. Eyes with at least three of these risk factors were considered to be at high risk. Since these eyes demonstrated a 50% reduction of severe visual loss with photocoagulation, prompt treatment was recommended for eyes with PDR and HRC as defined by the DRS.
Three clinical situations were thus characteristic of eyes with high-risk retinopathy: (a) NVD equal to or greater than one-fourth to one-third disc area (greater than photograph 10A); (b) less extensive NVD with preretinal or vitreous hemorrhage; (c) NVE equal to or greater than one-half disc area with preretinal or vitreous hemorrhage (Table 7C.1).
For high-risk eyes, the risk of severe visual loss was substantially reduced at 2 years and 4 years using either xenon or argon photocoagulation, and the beneficial effects far outweighed the side effects of either modality. Nevertheless, argon was recommended rather than xenon arc because of similar benefits and less harmful effects.
Before a protocol amendment, the initial DRS protocol included direct treatment of NVD in eyes randomized to argon laser. Since this was associated with an increased risk of hemorrhage at the time of treatment without an increase in NVD regression, this treatment technique was discontinued.
Unanswered Questions
Although prompt photocoagulation was recommended for eyes with PDR and HRC as defined by the DRS, the DRS did not provide a clear recommendation for eyes with early PDR or those with severe NPDR. The question remained as to whether photocoagulation performed at an earlier stage of retinopathy would be more beneficial. At the other end of the spectrum, the DRS did
not address the surgical management of late complications of diabetic retinopathy, such as severe fibrovascular proliferation and vitreous hemorrhage.
not address the surgical management of late complications of diabetic retinopathy, such as severe fibrovascular proliferation and vitreous hemorrhage.
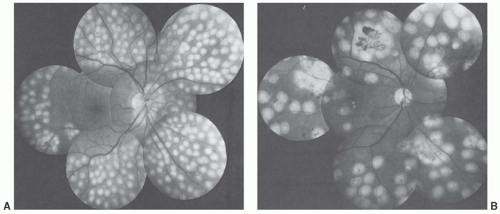 FIGURE 7C.8 (A) Twenty-four-hour posttreatment photographs after Diabetic Retinopathy Study argon technique. Note extensive 500-µ scatter burns, focal treatment of neovascularization of the disc adjacent to the disc, and confluent focal treatment of two small patches of neovascularization elsewhere (NVE) along the inferotemporal artery inferotemporal to the macula. (B) Twenty-four-hour posttreatment photographs after DRS xenon technique. Scatter burns are less evenly spaced than the argon burns in Figure 7C.8A. Confluent focal treatment has been applied to four patches of NVE. A small preretinal hemorrhage within the NVE superotemporal to the disc has occurred since treatment. Focal treatment has been applied to microaneurysms (thought to be the cause of mild macular edema) temporal to the macula. (From Diabetic Retinopathy Study Research Group. Photocoagulation of proliferative diabetic retinopathy: clinical applications of DRS findings. DRS Report 8. Ophthalmology. 1988;88:583-600.) |
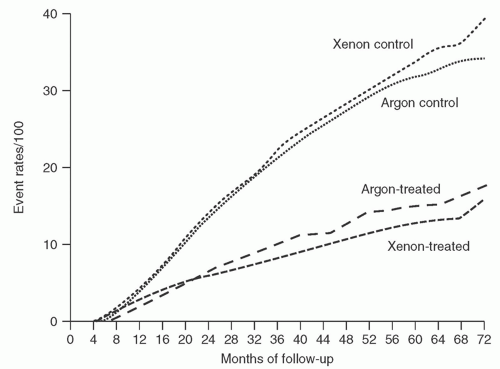 FIGURE 7C.9 Cumulative rates of severe visual loss for argon-treated and xenon-treated groups and controls. (From Diabetic Retinopathy Study Research Group. Photocoagulation of proliferative diabetic retinopathy: clinical applications of DRS findings. DRS Report 8. Ophthalmology. 1988;88:583-600.) |
In addition to PDR, DME remained a significant cause of visual loss in diabetic patients. In the DRS, panretinal scatter photocoagulation was associated with
progression of macular edema in some patients.20 The DRS did not adequately assess this effect, nor did it evaluate the potential benefit of focal photocoagulation.
progression of macular edema in some patients.20 The DRS did not adequately assess this effect, nor did it evaluate the potential benefit of focal photocoagulation.
TABLE 7C.1 Eyes with at Least Three of These Risk Factors (High-Risk Characteristics) Were Considered to Be at High Risk for Severe Visual Loss, and These Eyes Demonstrated the Most Benefit from Photocoagulation | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
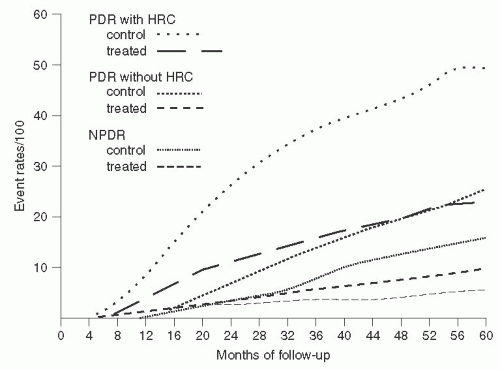 FIGURE 7C.10 Cumulative rates of severe visual loss for eyes classified to have proliferative diabetic retinopathy (PDR), high-risk characteristics (HRC), and nonproliferative diabetic retinopathy (NPDR) at baseline. Argon and xenon groups combined. (From Diabetic Retinopathy Study Research Group. Photocoagulation of proliferative diabetic retinopathy: clinical applications of DRS findings. DRS Report 8. Ophthalmology. 1988;88:583-600.) |
II. DIABETIC RETINOPATHY VITRECTOMY STUDY
Introduction
The Diabetic Retinopathy Vitrectomy Study (DRVS) has provided tremendous value to our understanding of the sight-threatening complications related to PDR. While the DRS addressed laser treatment for eyes with PDR and severe NPDR, the DRVS sought to evaluate the surgical management of eyes with more severe complications, and it attempted to define the role and timing of vitrectomy. Specifically, the DRVS was established by the National Eye Institute to evaluate the risks and benefits of performing early pars plana vitrectomy in eyes with advanced PDR.
Conducted in the late 1970s and early 1980s, this multicenter, prospective, RCT comprised three studies.21,22,23,24,25 One was a natural history study that included eyes with severe PDR but without severe vitreous hemorrhage, and these eyes were followed up with conventional management.21 The other two studies were RCTs involving vitrectomy. The first of these randomized trials compared
early vitrectomy (before 6 months) versus deferral of surgery (1 year) in eyes with severe nonclearing vitreous hemorrhage,22,25 and the second compared early vitrectomy versus conventional management in eyes with advanced, active PDR (severe fibrovascular proliferation) and useful vision.23,24 Each of these studies is addressed separately.
early vitrectomy (before 6 months) versus deferral of surgery (1 year) in eyes with severe nonclearing vitreous hemorrhage,22,25 and the second compared early vitrectomy versus conventional management in eyes with advanced, active PDR (severe fibrovascular proliferation) and useful vision.23,24 Each of these studies is addressed separately.
III. NATURAL HISTORY STUDY
Background and Study Questions
Despite the early success obtained with vitrectomy, the procedure had a high rate of complications and some patients lost all perception of light. As technical advances were made, vitrectomy was offered to an increasing number of patients with the sequelae of PDR. It was difficult for clinicians to determine the proper role of vitrectomy because of a lack of sufficient information regarding the natural course of the disease.
It was in this context that a natural history study was undertaken. Eyes with severe PDR but without severe vitreous hemorrhage were followed up with conventional management for 2 years.
Patients Included in the Study
A total of 744 eyes (622 patients) with very severe PDR were enrolled. There were three subgroups, defined by the dominant retinopathy at baseline: eyes with severe new vessels at least four disc areas in size and visual acuity 10/50 or better, eyes with extramacular traction retinal detachment at least four disc areas in extent and visual acuity 10/50 or better, and eyes with vitreous hemorrhage obscuring at least one-half of at least three standard photographic fields with visual acuity 10/200 or better or between 5/200 and hand motion.
Intervention and Outcome Measures
Patients were followed up with conventional management, including photocoagulation, over a 2-year period. Patients were offered vitrectomy only if they developed retinal detachment involving the center of the macula or if they developed severe vitreous hemorrhage that did not clear after 1 year of follow-up. The primary outcome measure was visual acuity, assessed at 1 and 2 years. Good vision was defined as 10/20 or better, and poor vision was less than 5/200.
Major Findings
Decreases in visual acuity were more frequent during the first year of follow-up than during the second year, and were related to retinopathy severity and baseline visual acuity. In eyes with more than four disc areas of new vessels and visual acuity of 10/30 to 10/50 at baseline, visual acuity decreased to < 5/200 in 45% at 2 years. In contrast, in eyes with traction retinal detachment not involving the center of the macula and without active new vessels or fresh vitreous hemorrhage at baseline, visual acuity decreased to < 5/200 in only 14%. Vitrectomy, which was required only if a macula-involving retinal detachment occurred or if severe vitreous hemorrhage did not clear after 1 year, was performed in 25% of eyes during the 2-year follow-up period.21
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


