Purpose
To assess the prognostic value of the Ocular Trauma Score in patients with combined open globe injuries and facial fractures.
Design
Retrospective cohort study.
Methods
A comprehensive chart review was conducted on 25 patients (28 eyes) identified from the Elmhurst City Hospital Trauma Registry between January 1, 2000 and June 30, 2012. Elmhurst City Hospital is a level 1 trauma center located in Elmhurst, New York, USA.
Results
Average age was 52 (range 18–88) and patients were predominantly male (84%). The majority of patients had an Ocular Trauma Score of 1 (87.5%), and of these patients, 76% and 14% had final visual acuities of no light perception (NLP) and light perception/hand motion (LP/HM), respectively. These corresponded to 74% and 15% predicted by the original Ocular Trauma Score guidelines (100% sensitive and 100% specific). Ocular Trauma Score of 1 was associated with zone 3 eye wound location ( P = .02). Independent of Ocular Trauma Score, initial visual acuity and frontal bone fractures were predictive of NLP ( P = .006 and P = .047). Nonblindness was associated with nasal bone fractures ( P = .047).
Conclusion
This study validates the use of the Ocular Trauma Score in patients with combined facial fracture and open globe injury. The presence of facial fractures does not appear to influence visual prognosis for open globe injuries with an Ocular Trauma Score of 1. In the absence of data to calculate a full Ocular Trauma Score, initial visual acuity was the strongest predictor of final visual outcome.
There is a lack of consistent prognostic data on the visual outcomes of patients with combined open globe injuries and facial fractures. In the majority of cases of orbital trauma, impact forces are absorbed by the eyeball itself or by the facial bone structure, leading to either globe injury or orbital fracture, respectively. However, there is a subpopulation of patients in which the impact force overcomes both globe and bone strength, leading to combined open globe injury with orbital fracture. These patients represent a population with higher morbidity and unique management questions.
Ophthalmic care in these cases requires combined expertise of oral maxillofacial surgery; ear, nose, and throat; plastic surgery; oculoplastics; cornea; and retina teams. Providers of varying specialties are often at odds in deciding the management of these patients. Ophthalmologists advocate for salvaging the eye first without the potential for further ocular damage from fracture repair such as open reduction internal fixation (ORIF). From the perspective of plastic surgeons, it is important to attend to the aesthetic consequences of traumatic injuries quickly. It is well known that patients with combined open globe injury and facial fractures have a very guarded visual prognosis. However, clinical studies on this population vary in terms of which characteristics are reported to be associated with specific visual outcomes and are difficult to use when assessing patients in such emergent circumstances.
In 2002, a comprehensive system, the Birmingham Eye Trauma Terminology System (BETT), was developed classifying the subtypes of ocular trauma to the globe. Open globes are injuries in which there is a full-thickness wound to the eyeball. They can be secondary to rupture caused by a blunt object or laceration caused by a sharp object, and can be further stratified into penetrating (entrance wound), perforating (entrance and exit wounds), or intraocular foreign body injuries. In contrast, closed globe injuries can be classified as contusions or lamellar lacerations, in which there is only a partial-thickness wound. Classification of open globe injuries should also include stratification of visual acuity, the presence or absence of a relative afferent pupillary defect (RAPD), and the zone of injury, which classifies the extent of corneal involvement.
Prior to 2002, many systems were proposed for predicting expected visual outcomes in patients with open globe injuries. These systems were simplified based on standardized terminology with the advent of the Ocular Trauma Score, which was developed using databases of the United States and Hungarian Eye Injury Registries. The Ocular Trauma Score supplies patients with the likelihood of various visual acuity scores after serious eye injury by calculations based on initial visual acuity, presence of rupture, development of endophthalmitis, perforating injury, retinal detachment, and RAPD. The prognostic value of the Ocular Trauma Score has previously been evaluated in retrospective case series for pediatric open globe injuries, deadly weapon–related open globe injuries, and patients with ocular trauma after firecracker exposure.
The sensitivity and specificity of the Ocular Trauma Score were calculated in predicting the final visual acuity of 48 patients (54 eyes) that incurred perforating injury from ocular firecracker trauma in Zhengzhou, China. For this subset of patients, the Ocular Trauma Score was concluded to predict final visual acuity less than 20/200 with 100% sensitivity and specificity. In pediatric patients with open globe injuries, the Ocular Trauma Score was found to be significantly prognostic, even when evaluation of RAPD was not possible at initial examination and could not be included in score calculations. In 82 patients (88 eyes) with open globe injuries secondary to deadly weapon–related trauma, final visual acuities were comparable to those predicted by the Ocular Trauma Score in all categories aside from patients predicted to have light perception/hand motion (LP/HM) with an Ocular Trauma Score of 2. This study aims to assess the predictive value and applicability of the Ocular Trauma Score in patients with combined open globe injury and facial fractures.
Methods
This was a retrospective cohort study in which patients with International Classification of Diseases, Ninth Revision (ICD-9) code classifications for both open globe injury and facial fractures were identified from the Elmhurst City Hospital Trauma Registry between January 1, 2000 and June 30, 2012. The study protocol received prospective institutional review board approval from the Queens/Elmhurst Research Committee to conduct a comprehensive paper chart review. Elmhurst Hospital Center is a level 1 trauma center in Elmhurst, New York, USA affiliated with the Icahn School of Medicine at Mount Sinai. Retrospective chart review noted visual outcomes and clinical characteristics of patients, including demographics, mechanism of injury, initial and final visual acuity, eye zone wound location, fracture type, and the type of and time to surgical intervention. The presence or absence of ocular trauma signs such as lid laceration, retinal detachment, afferent pupillary defect (APD), hyphema, and uveal prolapse were also noted.
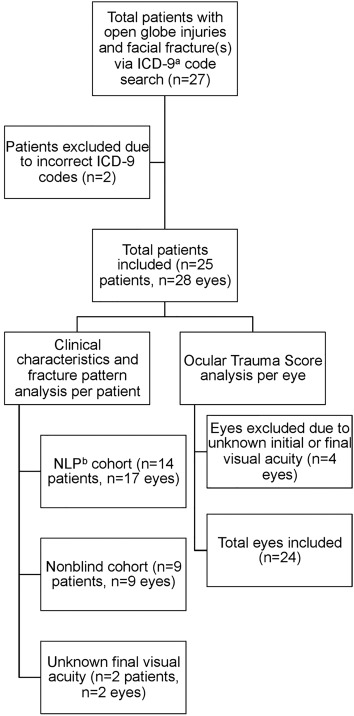
Of 1986 patients identified with open globe injury and/or facial fracture, 27 (1.4%) had both injuries based on ICD-9 codes. Two patients were excluded after comprehensive review of paper charts because they were coded incorrectly as having open globe injuries ( Figure ). Of the 25 remaining patients included in this study, 28 open globe injuries occurred, with 3 patients (12%) incurring bilateral open globe injuries. The no light perception (NLP) cohort consisted of 14 patients with 17 blind eyes. The nonblind cohort consisted of 9 patients with 9 nonblind eyes, where nonblind was considered any visual acuity other than NLP. The final visual acuity was unknown for 2 patients, 1 of whom was lost to follow-up and the other of whom was transferred to a different hospital system where medical records could not be obtained.
For patients with bilateral open globe injury, ophthalmologic data were recorded and analyzed individually for each eye and demographic and facial fracture data were recorded and analyzed for each patient. Eye zone wound locations were classified based on ophthalmology examination notes, operative reports, and the Ocular Trauma Classification Group system. This defines zone I as wounds involving only the cornea, zone II as wounds involving the cornea with extension into the anterior 5 mm of the sclera, and zone III as wounds involving the sclera extending more than 5 mm from the limbus.
For the purpose of Ocular Trauma Score calculations and analyses, an additional 4 eyes were excluded ( Figure ). The charts for these eyes noted many ocular trauma signs, thus making them relevant for clinical characteristic and fracture pattern analysis. However, medical records lacked initial or final visual acuity data, so the Ocular Trauma Score either could not be calculated at all or could not be interpreted after calculation. A total of 24 eyes were analyzed in regard to the Ocular Trauma Score. Raw Ocular Trauma Scores were calculated based on summation of values assigned to relevant clinical characteristics at presentation. In calculation, the following points were assigned to each initial visual acuity: NLP +60, LP/HM +70, 1/200–19/200 +80, 20/200–20/50 +90, and ≥20/40 +100. The following points were subtracted: rupture -23 (all open globe injuries), endophthalmitis -17, perforating injury -14, retinal detachment -11, and APD -10. Raw scores were then converted to Ocular Trauma Score categories (1–3). By virtue of the fact that all patients in our cohort incurred open globe injuries, no patient had an Ocular Trauma Score of 4 (81–91 raw points) or 5 (92–100 raw points). All started at a baseline of 77 raw points before consideration of other clinical factors in score calculations. Actual final visual outcomes were compared to those predicted by the original Ocular Trauma Score study ( Table 1 ). Sensitivity and specificity were then calculated for each Ocular Trauma Score category ( Table 2 ).
| Predicted Final Visual Acuities Based on Ocular Trauma Score System | ||||||
|---|---|---|---|---|---|---|
| Raw Score | Ocular Trauma Score | NLP | LP/HM | 1/200–19/200 | 20/200–20/50 | ≥20/40 |
| 0–44 | 1 | 74% | 15% | 7% | 3% | 1% |
| 45–65 | 2 | 27% | 26% | 18% | 15% | 15% |
| 66–80 | 3 | 2% | 11% | 15% | 31% | 41% |
| Actual Final Visual Acuities In Open Globe Injury and Facial Fracture Cohort (N = 24) | ||||||
|---|---|---|---|---|---|---|
| Raw Score | Ocular Trauma Score | NLP | LP/HM | 1/200–19/200 | 20/200–20/50 | ≥20/40 |
| 0–44 | 1 | 16 (76%) | 3 (14%) | 1 (4.8%) | 0 (0%) | 1 (4.8%) |
| 45–65 | 2 | 1 (50%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (50%) |
| 66–80 | 3 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (100%) |
| Visual Acuity | Actual Number of Eyes | Predicted Number of Eyes From Ocular Trauma Score | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|
| NLP | 17 | 17 | 100 | 100 |
| LP/HM | 3 | 4 | 100 | 95 |
| 1/200–19/200 | 1 | 1 | 100 | 100 |
| 20/200–20/50 | 0 | 1 | — | 96 |
| ≥20/40 | 3 | 1 | 33 | 100 |
There were marked differences in notation style of medical records among all patients, leading to missing data points that were marked as unknown in our analysis. Statistical analysis was performed using SPSS (SPSS Inc. Released 2009. PASW Statistics for Windows, Version 18.0. Chicago: SPSS Inc.). The Student t test and Fisher exact test were used to compare average values and proportions, respectively. The cutoff for P value significance was P < .05 (2-tailed) at a 95% confidence interval.
Results
Average age was 52 (range 18–88) and 21 of 25 patients (84%) were male ( Table 3 ). The overall blindness rate was 17 of 28 eyes (61%). Blunt trauma accounted for 9 of 14 blinding injuries (64%). Penetrating trauma accounted for 5 of 14 blinding injuries (36%), with 4 out of 5 penetrating injuries occurring owing to gunshot wounds. Two gunshot wound victims incurred bilateral open globe injuries. The remaining patient with bilateral open globe injury suffered blunt trauma from a motor vehicle collision. All 5 penetrating injuries led to a final visual outcome of NLP.
| Variable | NLP | Nonblind | Unknown Final Visual Acuity | P Value [95% CI] |
|---|---|---|---|---|
| Eyes | 17 | 9 | 2 | |
| Patients | 14 | 9 | 2 | |
| Age | 50 (18–88) | 56 (35–72) | .49 | |
| Mechanism of injury | ||||
| Blunt | 9 (64%) | 9 (100%) | 2 (100%) | .12 [0.32–0.79] |
| Penetrating | 5 (36%) | 0 (0%) | 0 (0%) | |
| Injury severity | ||||
| 1 | 7 (50%) | 5 (55.6%) | 2 (100%) | 1 [0.15–4.3] |
| 2 | 7 (50%) | 4 (44%) | 0 (0%) | |
| Initial visual acuity | ||||
| NLP | 14 (82%) | 1 (11%) | 0 (0%) | *.006 |
| LP | 2 (12%) | 4 (44%) | 0 (0%) | |
| >20/400 | 1 (6%) | 2 (22%) | 2 (100%) | |
| Unknown | 0 (0%) | 2 (22%) | 0 (0%) | |
| Eye zone wound location | ||||
| Zone I only | 0 (0%) | 1 (11%) | 0 (0%) | .27 |
| Zone II only | 1 (6%) | 3 (33%) | 1 (50%) | |
| Zone III only | 8 (47%) | 4 (44%) | 0 (0%) | |
| Zone I & II | 4 (23.5%) | 1 (11%) | 1 (50%) | |
| Unknown | 4 (23.5%) | 0 (0%) | 0 (0%) | |
| Afferent pupillary defect at presentation | ||||
| Yes | 14 (82%) | 5 (56%) | 0 (0%) | .19 [0.61–22.9] |
| No | 3 (18%) | 4 (44%) | 2 (100%) | |
| Hyphema at presentation | ||||
| Yes | 7 (41%) | 7 (78%) | 0 (0%) | 1 [0.11–9.2] |
| No | 2 (12%) | 2 (22%) | 2 (100%) | |
| Unknown | 8 (47%) | 0 (0%) | 0 (0%) | |
| Uveal prolapse at presentation | ||||
| Yes | 12 (71%) | 5 (56%) | 0 (0%) | .12 [0.85–108.7] |
| No | 1 (6%) | 4 (44%) | 2 (100%) | |
| Unknown | 4 (23.5%) | 0 (0%) | 0 (0%) | |
| Eyelid laceration | ||||
| Yes | 5 (29%) | 3 (33%) | 1 (50%) | 1 [0.15–4.7] |
| No | 12 (71%) | 6 (67%) | 1 (50%) | |
| Retinal detachment or vitreous hemorrhage | ||||
| Yes | 5 (29%) | 6 (67%) | 0 (0%) | .39 [0.06–2.2] |
| No | 7 (41%) | 3 (33%) | 2 (100%) | |
| Unknown | 5 (29%) | 0 (0%) | 0 (0%) | |
| Extraocular movements | ||||
| Limited | 10 (59%) | 3 (33%) | 0 (0%) | .21 [0.44–101.7] |
| Intact | 1 (6%) | 2 (22%) | 2 (100%) | |
| Unknown | 6 (35%) | 4 (44%) | 0 (0%) | |
| Extraocular muscle entrapment | ||||
| Yes | 2 (12%) | 2 (22%) | 0 (0%) | .59 [0.05–4.0] |
| No | 15 (88%) | 7 (78%) | 2 (100%) | |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


