Purpose
To report glaucoma outcomes after Boston type 1 keratoprosthesis (KPro) surgery, in particular, glaucoma prevalence, progression, and treatment.
Design
Consecutive, retrospective, interventional case series.
Methods
setting: Tertiary care institution. study population: Thirty-eight eyes in 38 patients. intervention: KPro surgery. main outcome measures: Visual acuity (VA), intraocular pressure, visual fields, optic nerve status, and glaucoma treatment.
Results
Glaucoma diagnosis was known before surgery in 29 patients (76%; 14 had undergone previous surgery) and was diagnosed after surgery in 34 patients (89%) after a mean ± standard deviation of 16.5 ± 4.7 months of follow-up. The number of patients taking intraocular pressure-lowering medications increased from 19 (50%) before surgery to 28 (76%) after surgery ( P = .017). Twenty-four patients (63%) were taking at least 1 additional glaucoma medication at their most recent postoperative visit. Eight patients (21%) had glaucoma progression (visual field progression, need for surgery, or both). Fifteen patients (40%) had a cup-to-disc ratio of 0.85 or more. Five patients required glaucoma surgery. VA was limited by glaucoma in 14 patients (37%), 11 of whom had a VA of 20/200 or worse. Five such patients (13%) had a dramatic improvement in VA, then progressed to end-stage glaucoma with fixation loss. Visual fields were limited by glaucoma in 25 patients (66%; mean Swedish Interactive Threshold Algorithm Fast mean defect, −20.3 ± 8.8 decibels; n = 18).
Conclusions
Most KPro candidates have glaucoma, which may deteriorate in a subset of patients after surgery. Dramatic VA improvement after KPro surgery does not preclude the need for rigorous monitoring for glaucoma progression. A low threshold should be used to treat suspicion of even slightly elevated intraocular pressure.
The Boston type 1 keratoprosthesis (KPro; Massachusetts Eye and Ear Infirmary, Boston, Massachusetts, USA) is an increasingly accepted treatment for corneal blindness. KPro surgery can restore vision in patients who are poor candidates for penetrating keratoplasty (PK). Corneal disease is the second most common cause of legal blindness in developing nations. Because eye banking is restricted in these countries, there exists great potential for this procedure to have a positive impact on millions of patients. The rate of extrusion and endophthalmitis after KPro surgery is significantly lower since the introduction of bandage contact lenses, prophylactic antibiotics, and an improved threadless design. Despite these advances, glaucoma can compromise visual rehabilitation even with the maintenance of a clear optical window in these patients. Candidates for KPro often have advanced anterior segment disease and a history of multiple prior surgeries, and therefore are at particularly high risk for glaucoma. The purpose of the present study is to report glaucoma outcomes after KPro surgery at a single institution and in particular to determine the prevalence, rate of progression, and treatment of glaucoma in these patients.
Methods
A retrospective, interventional case series was conducted including all eyes that underwent KPro implantation between October 2008 and November 2009 at a single center. Patients eligible for KPro surgery were judged to have a minimal chance of long-term visual recovery with PK.
A thorough chart review was conducted. Preoperative data included ophthalmic diagnosis, history of glaucoma, previous ocular surgery, and medication history. All patients underwent a detailed ocular examination including measurements of best-corrected visual acuity (BCVA) and applanation intraocular pressure (IOP). Patients demonstrated normal B-scan ultrasonography results, light projection results, and red colour perception before KPro surgery.
The operative protocol was reviewed. Patients were evaluated clinically on postoperative day 1, weekly for 4 weeks, and every 3 months thereafter. BCVA and digital palpation for IOP detection were assessed at each visit. Clinically important improvement in BCVA was defined as a change from counting fingers or worse before surgery to 20/200 or better after surgery. If preoperative BCVA was better than counting fingers, VA improvement was defined as a 2-line gain in Snellen VA after surgery. The most recent cup-to-disc ratio was recorded (most often as noted by a glaucoma specialist). Visual fields (VFs) were performed after surgery and were repeated at the treating doctor’s discretion using automated perimetry with the 24-2 Humphrey Swedish Interactive Threshold Algorithm Fast system (SITA Fast; Humphrey Systems, Dublin, California, USA) in collaborating patients or with Goldmann perimetry in others. All complications and ocular pathologic features limiting visual acuity or fields were noted. A glaucoma specialist followed up glaucoma patients concurrently.
The operative procedure included implantation of the Boston type I KPro along with either a fresh or frozen corneal graft, performed according to a standard surgical technique. All KPro surgeries were performed using the new threadless design by the same surgeon (M.H.-D.). Extracapsular lens extraction was performed when patients were phakic, and anterior vitrectomy was performed in patients without a posterior chamber lens. Sphincterotomy and iridectomy were performed in nonaniridic patients. After surgery, patients received a regimen of topical moxifloxacin (Alcon Canada Inc., Mississauga, Ontario, Canada) and prednisolone acetate 1% (Sandoz Canada Inc., Boucherville, Quebec, Canada), both 4 times daily. Any preoperative topical glaucoma medications were continued after surgery. Any additional topical or systemic glaucoma medications were added as needed based on IOP, cup-to-disc ratio, and VFs.
Data Analysis
Categorical variables are expressed as frequencies and percentages. Continuous variables are presented as mean ± standard deviation. Comparisons were performed using the Pearson chi-square test for categorical data and the Student t test for continuous data (Analyse-It; Analyse-it Software, Ltd., Leeds, United Kingdom). All comparisons were 2-tailed, and a P value of less than .05 was considered statistically significant.
Definition of Glaucoma Outcomes
Patients were deemed to have pre-existing glaucoma if they were taking IOP-lowering medications before surgery, if they had a clear history of glaucoma, or if they had undergone previous glaucoma surgery. A glaucoma specialist diagnosed glaucoma after surgery if the study eye displayed a glaucomatous-appearing optic nerve with increased cup-to-disc ratio, if medications were needed to control IOP, or if VF defects characteristic of glaucoma were apparent (such as an arcuate defect, paracentral scotoma, or nasal step). Patients demonstrating no improvement in BCVA after surgery with advanced optic nerve cupping (≥ 0.85) and a severely restricted VF were presumed to have pre-existing terminal glaucoma.
Definite glaucoma progression was determined clinically by a glaucoma specialist based on the presence of 1 of the following 4 criteria: (1) a Goldmann VF defect that widened by more than 15 degrees in any direction in a pattern characteristic of glaucoma (e.g., widening of a nasal step or progression of arcuate defect to a hemifield defect), (2) the mean defect worsened by more than 10 decibels on a SITA Fast VF, (3) a paracentral scotoma extended centrally with decreased VA and fixation loss, or (4) glaucoma surgery was required for high IOP on maximal medical therapy.
Results
Preoperative Clinical Characteristics
Thirty-eight eyes (19 left, 19 right) in 38 consecutive patients underwent Boston type 1 KPro surgery between October 2008 and November 2009. All 38 eyes were included in this review. The mean age was 60.5 ± 14.8 years (range, 30 to 95 years). Most patients (27/38, 71%) were male. Table 1 summarizes the baseline diagnoses, presence of baseline glaucoma, and glaucoma progression in all patients. Indications for KPro included those with previous PK failure, significant deep corneal vascularization, severe limbal stem cell deficiency, and autoimmune disease. The most common preoperative diagnoses were congenital aniridia (11/38, 29%), posttraumatic scar (4/38, 11%), and chemical burn (3/38, 8%). Most patients were white (29/38, 76%), whereas the remainder were black (5/38, 13%), Middle Eastern (3/38, 8%), and Asian (1/38, 3%). Mean axial length was 23.6 ± 2.9 mm (range, 20.7 to 31.5 mm). Twenty-five patients (66%) had a history of failed PK. The mean number of previous PKs in these eyes was 2.1 ± 1.3 (range, 1 to 5). One hundred percent KPro retention was obtained in this series of patients. There were no cases of extrusion, corneal melt, or endophthalmitis during a mean follow-up time of 16.5 ± 4.7 months.
| Corneal Diagnosis (n) | Glaucoma Prevalence (n, (%)) a | Glaucoma Progression (n, (%)) |
|---|---|---|
| Failed PK (25) | ||
| Aniridia (6) | 6 (100%) | 0 |
| Chemical burn (3) | 3 (100%) | 1 (33%) |
| Trauma (3) | 1 (33%) | 0 |
| Congenital glaucoma (2) | 2 (100%) | 1 (50%) |
| CHED (2) | 2 (100%) | 1 (50%) |
| HSV keratitis (2) | 2 (100%) | 1 (50%) |
| PBK (2) | 2 (100%) | 0 |
| Lattice dystrophy (1) | 1 (100%) | 1 (100%) |
| Unknown dystrophy (1) | 1 (100%) | 1 (100%) |
| Congenital cataract (1) | 1 (100%) | 0 |
| Chronic uveitis (1) | 1 (100%) | 0 |
| Bacterial keratitis* (1) | 1 (100%) | 0 |
| Total (25) | 22 (88%) | 6 (24%) |
| Primary KPro (13) | ||
| Aniridia (5) | 5 (100%) | 0 |
| SJS (1) | 1 (100%) | 1 (100%) |
| Trauma (1) | 1 (100%) | 0 |
| HSV keratitis (1) | 0 | 0 |
| PBK (1) | 1 (100%) | 0 |
| ABK (1) | 1 (100%) | 0 |
| Anesthetic abuse (1) | 1 (100%) | 0 |
| Bacterial keratitis (1) | 1 (100%) | 1 (100%) |
| LSCD dystrophy (1) | 1 (100%) | 0 |
| Total (13) | 12 (92%) | 2 (15%) |
| Total (38) | 34 (89%) | 8 (21%) |
a Represented as a percentage of the subgroup of patients with this particular diagnosis who have glaucoma. For example, 3 of 3 patients with failed PK and an underlying diagnosis of chemical burn have glaucoma (100%) and 1 of 3 had glaucoma progression (33%).
Visual Acuity Outcomes
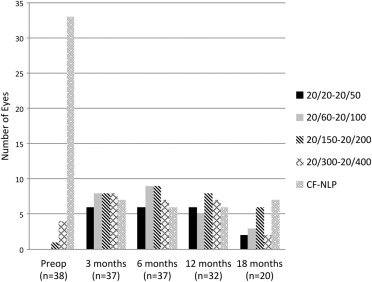
Preoperative BCVA in study eyes ranged from 20/150 to light perception, with 92% (n = 35) of patients seeing 20/400 or worse. Twenty-seven patients (71%) had a BCVA ranging from 20/200 to no light perception in their fellow, nonoperated eye at the time of KPro surgery. The remaining 11 patients (29%) had vision ranging from 20/20 to 20/100 in their fellow eye. Thirty-one eyes (82%) that underwent KPro surgery displayed postoperative BCVA improvement. Eyes with no demonstrated improvement in BCVA after surgery (n = 7) had pre-existing terminal glaucoma (n = 4), macular atrophy after previous retinal detachment (n = 1), myopic maculopathy (n = 1), and possible pre-existing terminal glaucoma (n = 1) that could not be confirmed because of loss to follow-up. VA outcomes are summarized in Figure 1 .
Lens Status
The relative proportion of aphakia increased from 24% (n = 9) before surgery to 87% (n = 33) after surgery. All phakic eyes (n = 18) became aphakic at the time of KPro surgery, and 6 of 11 pseudophakic patients underwent intraocular lens explantation as a result of the presence of an anterior chamber intraocular lens or instability of a posterior chamber lens.
Glaucoma Outcomes
Glaucoma was known before surgery in 29 patients (76%) and was diagnosed after surgery in 34 patients (89%). Glaucoma outcomes are summarized in Table 2 . Fourteen patients (37%) had undergone at least 1 previous glaucoma surgery. The mean number of previous glaucoma surgeries in these patients was 1.4 ± 0.5. Eleven patients (29%) were known to have glaucoma in their fellow eye before surgery. The number of patients taking IOP-lowering medications increased from 19 (50%) before surgery (including 16 patients receiving drops and 3 receiving oral acetazolamide) to 28 (76%) after surgery (including 29 patients receiving drops and 9 receiving oral acetazolamide; P = .017). Twenty-four patients (63%) were taking at least 1 additional glaucoma medication at their most recent postoperative visit (as compared with their preoperative medications). The average number of drops per patient increased from 0.89 ± 1.2 before surgery to 1.97 ± 1.6 after surgery ( P = .001). The treating physician had increased IOP-lowering medication as a result of VF progression, discovery of a limited VF, advanced cupping with borderline IOP, or high IOP. Eight patients (21%) experienced a hypertensive spike defined as an IOP of more than 25 mm Hg in the first 4 weeks after surgery. Twenty-five patients (66%) displayed VF defects secondary to glaucoma. The mean postoperative SITA Fast 24-2 mean defect was −20.3 ± 8.8 decibels (range, −30.8 to −5.0 decibels; n = 18). Fifteen patients (40%) had a cup-to-disc ratio of 0.85 or greater as determined by a glaucoma specialist.
| Preoperative | Postoperative | P Value | |
|---|---|---|---|
| Eyes with glaucoma | 29 (76%) | 34 (89%) | .13 |
| Eyes using IOP-lowering medication | 19 (50%) | 29 (76%) | .017 |
| Mean no. glaucoma drops per eye ± SD (minimum, maximum) | 0.89 ± 1.2 (0, 4) | 1.97 ± 1.6 (0, 5) | .001 |
| Eyes with previous glaucoma surgery | 14 (37%) | NA | |
| Eyes requiring increase in IOP-lowering medication (from preoperative baseline) | NA | 24 (63%) | |
| Eyes with IOP spike within 4 wks (estimated at > 25 mm Hg) | NA | 8 (21%) | |
| Eyes with VF limited by glaucoma | NA | 25 (66%) | |
| Mean SITA Fast 24-2 mean defect ± SD (minimum, maximum), dB | NA | −20.3 ± 8.8 (−30.8, −5.0) | |
| Eyes with cup-to-disc ratio ? 0.85 | NA | 15 (40%) | |
| Eyes with VA limited by glaucoma | NA | 14 (37%) | |
| Eyes with pre-existing terminal glaucoma | NA | 4 (11%) | |
| Eyes with dramatic VA improvement that then lost fixation because of glaucoma progression | NA | 5 (13%) | |
| Eyes with definite glaucoma progression | NA | 8 (21%) | |
| Eyes that underwent post-KPro glaucoma surgery | NA | 5 (13%) | |
| Ahmed tube shunt alone | NA | 1 (3%) | |
| Ahmed tube shunt followed by ECP and PPV | NA | 2 (5%) | |
| Trans-scleral CPC | NA | 1 (3%) | |
| PPV in eye with pre-existing tube shunt | NA | 1 (3%) | |
| Hypotensive complications after KPro | |||
| Choroidal detachment (after PPV with pre-existing tube shunt) | NA | 1 (3%) | |
| Suprachoroidal hemorrhage (in patient with pre-existing tube shunt) | NA | 1 (3%) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


