Purpose
To evaluate the prevalence of dry eye syndrome (DES) and its associated risk factors in a US Veterans Affairs population receiving ocular care services.
Design
Retrospective study.
Methods
settings: Patients were seen in the Miami and Broward Veterans Affairs eye clinics between 2005 and 2010. patients population: Patients were divided into cases and controls with regard to their dry eye status (cases = ICD9 code for DES plus dry eye therapy; controls = patients without ICD9 code plus no therapy). main outcome measures: The prevalence of DES and its associated risk factors.
Results
A total of 16 862 patients were identified as either a dry eye case (n = 2056) or control (n = 14 806). Overall, 12% of male and 22% of female patients had a diagnosis of DES, with female gender imparting a 2.40 increased risk (95% confidence interval [CI] 2.04–2.81) over male gender. Several medical conditions were found to increase DES risk including post-traumatic stress disorder (odds ratio [OR] 1.97, 95% CI 1.75–2.23), depression (OR 1.91, 95% CI 1.73–2.10), thyroid disease (OR 1.81, 95% CI 1.46–2.26), and sleep apnea (OR 2.20, 95% CI 1.97–2.46) (all analyses adjusted for gender and age). The use of several systemic medications, including anti-depressant medications (OR 1.97, 95% CI 1.79–2.17), anti-anxiety medication (OR 1.74, 95% CI 1.58–1.91), and anti–benign prostatic hyperplasia medications (OR 1.68, 95% CI 1.51–1.86), was likewise associated with an increased risk of DES.
Conclusions
The prevalence of DES was found to be high in both men and women in our eye care population. This is the first study to demonstrate that in a veteran population, several diagnoses were significantly associated with DES, including post-traumatic stress disorder and depression.
Dry eye syndrome (DES) has recently gained recognition as a public health problem. Part of this recognition came from several United States (US) and international population-based studies that identified the condition in 5% to 30% of the population aged 50 years or older. These estimates suggest that DES is more prevalent than diabetes (∼8% of US population), cancer (∼3% of US population), and heart disease (∼7% of US population). Another part of the recognition came from understanding that the symptoms of DES, which include constant irritation, foreign body sensation, and blurred vision, interfere with the ability to work and carry out daily functions. A study using the Impact of Dry Eye Living Questionnaire (IDEEL) found that severe dry eye symptoms were correlated with difficulties in physical, social, and mental functioning. A case-control study assessing the impact of dry eye symptoms on everyday activities found that patients with DES had difficulties with reading, carrying out professional work, watching television, and driving. These studies illustrate how significantly dry eye symptoms can impact a patient’s functioning.
Similar to worldwide experience, we believe that this condition presents a serious health problem within the Veterans Affairs population as many of the known risk factors associated with DES are common in veterans, namely older age, tobacco use, and use of systemic medications (eg, antidepressants, blood pressure medications). However, there is a paucity of data on DES in populations such as ours as prior DES research has focused predominantly on women and/or non-Hispanic whites. The Veterans Affairs administrative database provides a unique opportunity to study the epidemiology of DES as it has demographic, diagnosis, and medication information on a large number of patients. The goal of this study was to evaluate the prevalence of DES and its associated risk factors in a US veteran population and to compare these factors with those in the published literature.
Methods
Study Population
Patients seen in the Miami and Broward Veterans Affairs eye clinics between July 15, 2005 and July 15, 2010 were included in this analysis. Patients seen in Veterans Affairs clinics consist of ex-military personnel but do not include or represent all former military recruits. Patients seen in other Veterans Affairs outpatient clinics during this time period were not included as a preliminary analysis revealed that non–eye care professionals did not use the ICD9 code for DES. Patients were divided into cases and controls with regard to their dry eye status (cases included patients with an International Classification of Disease code [ICD9] for DES [375.15] who received some form of dry eye therapy [n = 2056]; controls included patients without an ICD9 code for DES who did not receive any form of dry eye therapy [n = 14 806]). Dry eye therapies included any type of artificial tear, gel, or ointment; topical cyclosporine 0.05% (Restasis); or punctal plugging procedure (Current Procedural Terminology code 68760 and 68761). Patients were excluded from the risk factor analysis if they had discordant dry eye information (eg, an ICD9 diagnosis but no dry eye therapy [n = 608] or no ICD9 diagnosis but with dry eye therapy [n = 3261]). The Miami Veterans Affairs Institutional Review Board reviewed and approved this study, which was conducted in accordance with the principles of the Declaration of Helsinki.
Data Collection
All data were extracted from the Veterans Affairs administrative database by an expert programmer (D.C.) and automatically converted into an Excel format. The data used for this analysis included demographic information (date of birth, gender, race, ethnicity), medical diagnosis information (extracted based on ICD9 codes), and use of systemic therapy (extracted based on pharmacy codes). The date at which DES was first diagnosed (if applicable) and the date of last visit were also extracted from the database.
Main Outcome Measures
The main outcome measure was prevalence of DES and its associated risk factors.
Statistical Analysis
All statistical analyses were performed using SPSS 18.0 (SPSS Inc, Chicago, Illinois, USA) statistical package. All P values are 2-sided and nominal. A crude period prevalence was calculated by dividing the number of dry eye cases identified over the 5-year period (ICD9 375.15 and dry eye therapy) over all patients seen during that time period. As it is likely that some patients with discordant ICD9 code/medication status information were misclassified dry eye cases, these patients were not included in the risk factor analyses. The exclusion of such discordant cases did have the effect of inflating the prevalence estimate in the risk factor analysis over the crude estimate. For the risk factor analysis, continuous variables were compared between the groups using the Student t test and categorical variables were compared using the χ 2 test. Multivariate logistic regression analyses (using the presence of DES as the dependent variable) were used to evaluate the effect of various risk factors on DES. All multivariate analyses were adjusted for gender and age.
Results
DES Prevalence
The crude period prevalence (number of dry eye cases over 5-year period divided by all patients seen during that time period) of dry eye syndrome in our veteran population was 10% (n = 2056/20 731).
Risk Factor Analysis of Demographic Characteristics
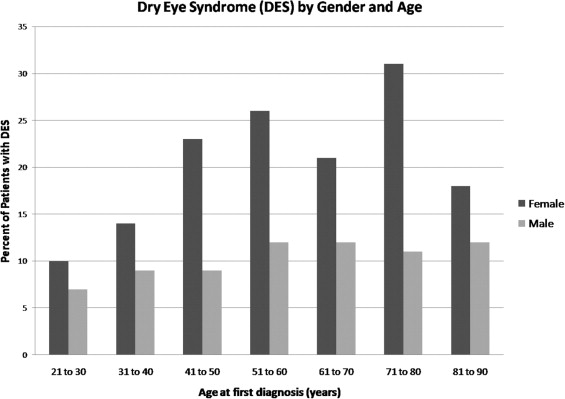
Excluding discordant cases (n = 3869), a total of 16 862 patients were identified as being either a dry eye case (n = 2056) or control (n = 14 806). The period prevalence for these patients (number of dry eye cases over 5-year period divided by a denominator, which excluded patients with discordant information) was 12% (n = 2056/16 862). Demographic characteristics of these patients are summarized in Table 1 . Overall, 12% of male subjects and 22% of female subjects had a diagnosis of DES, with female gender imparting a 2.40 increased risk of DES (95% confidence interval [CI] 2.04–2.81) over male gender, P < .0001. The Figure depicts the percentage of patients with DES by decade of age and gender; female patients had a higher percentage of DES in each age group compared to male patients and the overall risk of DES increased by 1.06 for each increasing decade (95% CI 1.02–1.10). The Veterans Affairs administrative database did not have complete information on race and ethnicity (information on race and ethnicity was available for approximately 30% of patients). With this limitation, black patients had a slightly increased prevalence over white patients (20% vs 18%, odds ratio [OR] 1.42, 95% CI 1.21–1.66) and Hispanic ethnicity had a slightly increased prevalence over non-Hispanic ethnicity. A sensitivity analysis was performed to determine if the exclusion of patients with discordant ICD9 and treatment information affected these demographic findings. Four such analyses were performed by including each excluded group (positive ICD9 but no therapy and absent ICD9 but with therapy) into both the DES and the no-DES categories. Results of the analyses revealed small changes in the magnitude of risk but no significant changes in its direction ( Table 2 ).
| Patient Characteristic | Number a | Prevalence | Odds Ratio b | P Value |
|---|---|---|---|---|
| Gender | ||||
| Male | 1831 | 12% | 1.00 | <.0001 |
| Female | 225 | 22% | 2.40 (2.04–2.81) | |
| Race | ||||
| White | 596 | 18% | 1.00 | <.0001 |
| Black | 341 | 20% | 1.42 (1.21–1.66) | |
| Other | 1 | 4% | N/A c | |
| Ethnicity | ||||
| Hispanic | 139 | 21% | 1.00 | .032 |
| Not Hispanic | 799 | 18% | 0.80 (0.65–0.98) |
a Number of patients with dry eye syndrome (present if ICD9 code 375.15 and received some form of dry eye therapy; absent if no ICD9 code 375.15 and received no form of dry eye therapy).
b Odds ratio adjusted for gender and age. A risk ratio greater than 1 represents an increased likelihood of dry eye disease.
| Inclusion of Patients With Discordant ICD9/Medication Status | Patient Characteristic | Number a | Prevalence | Odds Ratio b | P Value |
|---|---|---|---|---|---|
| ICD9 yes ; therapy no included in DES group (total N = 17 470) | Male | 2358 | 14% | 1.00 | <.0001 |
| Female | 306 | 28% | 2.50 (2.17–2.89) | ||
| ICD9 yes ; therapy no included in no-DES group (total N = 17 470) | Male | 1831 | 11% | 1.00 | <.0001 |
| Female | 225 | 20% | 2.25 (1.92–2.64) | ||
| ICD9 no ; therapy yes included in DES group (total N = 20 123) | Male | 4882 | 26% | 1.00 | <.0001 |
| Female | 435 | 35% | 1.71 (1.51–1.94) | ||
| ICD9 no ; therapy yes included in no-DES group (total N = 20 123) | Male | 1831 | 10% | 1.00 | <.0001 |
| Female | 225 | 18% | 2.27 (1.94–2.65) |
a Number of patients with DES.
b A risk ratio greater than 1 represents an increased likelihood of dry eye disease.
Risk Factor Analysis of Medical Conditions
Systemic diagnoses were identified in the administrative database using ICD9 codes. After adjusting for gender and age, several medical conditions were found to increase DES risk in our population ( Table 3 ). The magnitude of the increased risk was high in patients with psychiatric diagnoses. Nineteen percent of patients with a diagnosis of post-traumatic stress disorder (PTSD) carried a concomitant diagnosis of DES as opposed to 11% of patients without this diagnosis (OR 1.97, 95% CI 1.75–2.23). Likewise, 17% of patients with a diagnosis of depression had DES as opposed to 10% without this diagnosis (OR 1.91, 95% CI 1.73–2.10). Other factors associated with a similar increased risk of DES included autoimmune conditions (OR 1.96, 95% CI 1.74–2.20), non-autoimmune arthritis (OR 2.23, 95% CI 2.02–2.45), thyroid diseases (OR 1.81, 95% CI 1.46–2.26), and sleep apnea (OR 2.20, 95% CI 1.97–2.46). In a forward stepwise regression model considering age, gender, and all medical diagnosis, the presence of a psychiatric diagnosis (OR 1.54) and PTSD (OR 1.34) remained significant predictors of DES risk.
| Medical Condition (ICD9 Codes Used) | Number | Prevalence | Odds Ratio a | P Value |
|---|---|---|---|---|
| Vascular | ||||
| Diabetes mellitus (250) | ||||
| Yes | 692 | 10% | 0.68 (0.62–0.75) | <.0001 |
| No | 1364 | 14% | 1.00 | |
| Hypertension (401–405) | ||||
| Yes | 1520 | 13% | 1.35 (1.21–1.51) | <.0001 |
| No | 536 | 10% | 1.00 | |
| Lipid metabolism disorder (272) | ||||
| Yes | 1458 | 13% | 1.28 (1.16–1.42) | <.0001 |
| No | 598 | 10% | 1.00 | <.0001 |
| Ischemic heart disease (410–414) | ||||
| Yes | 605 | 13% | 1.09 (0.98–1.21) | .13 |
| No | 1451 | 12% | 1.00 | |
| Cerebral vascular disease (430–438) | ||||
| Yes | 341 | 16% | 1.37 (1.21–1.56) | <.0001 |
| No | 1715 | 12% | 1.00 | |
| Psychiatric | ||||
| Psychiatric illness (291–2, 294–301) | ||||
| Yes | 1021 | 17% | 2.08 (1.90–2.29) | <.0001 |
| No | 1035 | 9% | 1.00 | |
| Post-traumatic stress disorder (309.81) | ||||
| Yes | 414 | 19% | 1.97 (1.75–2.23) | <.0001 |
| No | 1642 | 11% | 1.00 | |
| Depression (300.4, 296) | ||||
| Yes | 873 | 17% | 1.91 (1.73–2.10) | <.0001 |
| No | 1183 | 10% | 1.00 | |
| Alcohol dependence (291, 303) | ||||
| Yes | 209 | 15% | 1.49 (1.27–1.74) | <.0001 |
| No | 1847 | 12% | 1.00 | |
| Drug dependence (292, 304, 305) | ||||
| Yes | 651 | 13% | 1.28 (1.15–1.41) | <.0001 |
| No | 1405 | 12% | 1.00 | |
| Autoimmune & arthritis | ||||
| Autoimmune diseases b | ||||
| Yes | 428 | 20% | 1.96 (1.74–2.20) | <.0001 |
| No | 1628 | 11% | 1.00 | |
| Non-autoimmune arthritis (715, 716) | ||||
| Yes | 939 | 19% | 2.23 (2.02–2.45) | <.0001 |
| No | 1117 | 9% | 1.00 | |
| Gout (274) | ||||
| Yes | 153 | 15% | 1.37 (1.14–1.64) | .001 |
| No | 1903 | 12% | 1.00 | |
| Thyroid diseases (241, 242, 245, 246) | ||||
| Yes | 109 | 21% | 1.81 (1.46–2.26) | <.0001 |
| No | 1947 | 12% | 1.00 | |
| Prostate | ||||
| Benign prostatic hyperplasia (600) | ||||
| Yes | 646 | 16% | 1.62 (1.46–1.81) | <.0001 |
| No | 1410 | 11% | 1.00 | |
| Prostate cancer (185) | ||||
| Yes | 186 | 14% | 1.13 (0.96–1.33) | .16 |
| No | 1870 | 12% | 1.00 | |
| Miscellaneous | ||||
| Sleep apnea (327.2, 780.51, 780.53) | ||||
| Yes | 524 | 20% | 2.20 (1.97–2.46) | <.0001 |
| No | 1532 | 11% | 1.00 | |
| Rosacea (695.3) | ||||
| Yes | 72 | 21% | 1.85 (1.42–2.41) | <.0001 |
| No | 1984 | 12% | 1.00 | |
| Human immunodeficiency virus (V08, 042) | ||||
| Yes | 63 | 16% | 1.52 (1.15–2.00) | .003 |
| No | 1993 | 12% | 1.00 | |
| Ocular | ||||
| Glaucoma (365) | ||||
| Yes | 587 | 14% | 1.22 (1.10–1.36) | <.0001 |
| No | 1469 | 12% | 1.00 | |
a Odds ratio adjusted for gender and age. A risk ratio greater than 1 represents an increased likelihood of dry eye disease.
b Autoimmune diseases include: Behcet syndrome, autoimmune disease, sarcoid, systemic lupus erythomatosis, rheumatoid arthritis, Wegner granulomatosis, vasculitis, vitiligo, psoriasis, ankylosing spondylitis, inflammatory bowel disease, Reiter syndrome, autoimmune hepatitis, collagen vascular diseases (136.1, 279.4, 135, 710.0-5, 695, 714, 446.4, 447.6, 446, 709.01, 696, 720, 555, 556, 558, 099.3, 711.1, 571.42, 710.9).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


