Purpose
To survey the prevalence of reticular pseudodrusen in late age-related macular degeneration (AMD) using multiple imaging methods, and to investigate the association between reticular pseudodrusen and polymorphisms in complement factor H ( CFH ) and age-related maculopathy susceptibility 2 ( ARMS2 ) genes.
Design
Retrospective case series.
Methods
This study included 216 consecutive patients with late AMD (typical AMD, polypoidal choroidal vasculopathy [PCV], retinal angiomatous proliferation [RAP], or geographic atrophy). Eyes were assessed for reticular pseudodrusen using the blue channel of color fundus photography, infrared reflectance, fundus autofluorescence, and spectral-domain optical coherence tomography. The major AMD-associated single nucleotide polymorphisms ( CFH Y402 rs1061170, CFH I62 V rs800292, and ARMS2 A69S rs10490924) were genotyped.
Results
Forty-nine eyes of 30 patients had a reticular pattern in ≥2 imaging modalities and were diagnosed with reticular pseudodrusen. Of these, 16 had bilateral late AMD, whereas 32 of 186 patients without reticular pseudodrusen had bilateral late AMD ( P < .001). The prevalence of reticular pseudodrusen was 83% in RAP, 50% in geographic atrophy, 9% in typical AMD, and 2% in PCV. The frequency of the T allele in ARMS2 A69S in patients with and without reticular pseudodrusen was 78.6% and 59.9%, respectively ( P = .007).
Conclusions
The prevalence of reticular pseudodrusen was low in PCV cases. About 50% of patients with reticular pseudodrusen had bilateral late AMD. The connection of ARMS2 risk allele and reticular pseudodrusen was confirmed in a Japanese population.
Reticular drusen, described in the Wisconsin Grading System as one type of drusen that form ill-defined networks of broad interlacing ribbons, were first identified using blue-light fundus photography. Arnold and associates described a yellowish interlacing network of oval-shaped or roundish lesions, termed reticular pseudodrusen, with a diameter of 125–250 μm that were seen in red-free fundus photography and infrared scanning-laser ophthalmoscopy (SLO). Recently, reticular pseudodrusen have been recognized as an additional distinctive morphologic feature observed in age-related macular degeneration (AMD). Furthermore, several reports have suggested that reticular pseudodrusen are associated with a high risk of progression to late AMD. In the longitudinal Beaver Dam Eye Study, reticular pseudodrusen were found to confer a high risk of progression to late-stage AMD, with twice the risk compared with eyes with soft drusen.
The development of new imaging methods, such as confocal SLO and spectral-domain optical coherence tomography (SD OCT), has led to improvements in diagnosing reticular pseudodrusen. Previous reports showed that near-infrared reflectance (IR), fundus autofluorescence (FAF), and SD OCT were more useful than conventional fundus photography to detect reticular pseudodrusen and suggested that the assessment of reticular pseudodrusen should involve multiple imaging methods.
Existing evidence suggests an association of AMD with polymorphisms in the complement factor H ( CFH ) gene and age-related maculopathy susceptibility 2 ( ARMS2 ) gene. Among the various polymorphisms, the Y402H and I62V variants in the CFH gene and the A69S variant in the ARMS2 gene have been reported to show an association with AMD. Recently an association between reticular pseudodrusen and polymorphisms in these genes has been reported. Klein and associates showed that the prevalence of reticular pseudodrusen was higher in those homozygous (CC) or heterozygous (TC) for CFH Y402H than in those without this variant (TT). On the other hand, Smith and associates demonstrated that CFH Y402H risk variant was significantly associated with the absence of reticular macular disease but enhanced risk for reticular macular disease was conferred by the ARMS2 A69S risk allele. Thus, to date, the association between reticular pseudodrusen and genomic background has not reached a consensus. In addition, little is known about the distribution of reticular pseudodrusen in each AMD subtype.
The purpose of this study was to survey the prevalence of reticular pseudodrusen in late AMD using multiple imaging methods and, moreover, to investigate the association of high-risk alleles in the CFH (Y402H, rs1061170 and I62V, rs800292) and ARMS2 (A69S, rs10490924) genes with reticular pseudodrusen. Several terminologies have been used to describe this clinical feature. In this report, we use the term “reticular pseudodrusen” according to the nomenclature by Arnold and associates.
Methods
We retrospectively reviewed the medical records of 249 consecutive patients with newly diagnosed late AMD who first visited the Macular Service at Kyoto University Hospital between August 3, 2009 and July 21, 2011. Subjects included in this study were ≥50 years of age and had either typical AMD, polypoidal choroidal vasculopathy (PCV), retinal angiomatous proliferation (RAP), or geographic atrophy. The diagnosis of PCV was based on the indocyanine green angiography (IA) showing a branching vascular network terminating in polypoidal swelling. The diagnosis of RAP was based on the criteria of Yannuzzi and associates via fundus photography, fluorescein angiography (FA), IA, and SD OCT. Neovascular AMD other than PCV or RAP was defined as typical AMD. Geographic atrophy was defined using color fundus photography as a sharply delineated area (at least 175 μm in diameter) of hypopigmentation, depigmentation, or apparent absence of the retinal pigment epithelium (RPE) in which choroidal vessels were clearly visible. Eyes with other macular abnormalities (ie, pathologic myopia, idiopathic choroidal neovascularization, presumed ocular histoplasmosis, angioid streaks, other secondary choroidal neovascularization, central serous chorioretinopathy, epiretinal membrane, or retinal arterial macroaneurysm) were excluded from this study. All diagnoses were made by 3 retinal specialists (S.O., K.Y., and A.T.) who observed the images together and discussed each case; however, a fourth specialist (N.Y.) was consulted in case of a disagreement between the 3 initial reviewers. The fourth specialist made a decision in 13 of the 249 patients (5.2%). Patients were included only if at least 3 specialists agreed on the diagnosis.
All study investigations adhered to the tenets of the Declaration of Helsinki, and the study protocol was approved by the Institutional Review Board and the Ethics Committee of Kyoto University Graduate School of Medicine prior to the study. Written informed consent was obtained from all patients who were genotyped. Because this was a retrospective study, written informed consent for research participation was not obtained, but the nature of this study was explained on our website.
Multimodal Imaging Methods
All patients underwent a complete ophthalmologic examination, including measurement of best-corrected visual acuity, determination of intraocular pressure, indirect ophthalmoscopy, slit-lamp biomicroscopy with a noncontact lens, color fundus photography, SD OCT, IR, FAF, FA, and IA.
Color fundus photographs (field, 30-40 degrees) were obtained digitally using a Topcon TRC NW6S nonmydriatic retinal camera (Topcon, Tokyo, Japan) after medical dilation of the pupil (phenylephrine 0.5% and tropicamide 0.5%). To examine the blue channel of the color photography, ImageJ software (National Institutes of Health, Bethesda, Maryland, USA) was used to display the individual color channels (red, green, and blue) of the obtained photographs. In ImageJ, the command path of Image > Color > Split Channels was used. Subsequently, the command path of Image > Adjust > Brightness/Contrast was used if needed. Adjustment was performed automatically using the ImageJ software before grading.
IR, FAF, FA, and IA images were acquired using a confocal SLO (Spectralis HRA+OCT; Heidelberg Engineering, Heidelberg, Germany). The IR images were obtained using a light stimulus of 820 nm. The FAF images were obtained using an excitation light of 488 nm and a barrier filter beginning at 500 nm. The field of view was set to 30 × 30 degrees centered on the macula.
SD OCT was conducted using a Spectralis HRA+OCT (Heidelberg Engineering). First, horizontal and vertical line scans through the fovea center were obtained at a 30-degree angle, followed by serial horizontal scans with an examination field size ranging from 30 × 10 degrees to 30 × 25 degrees, depending on the case. At each location of interest on the retina, 50 SD OCT images were acquired and averaged to reduce speckle noise.
Definition of the Reticular Pseudodrusen Using Multimodal Imaging
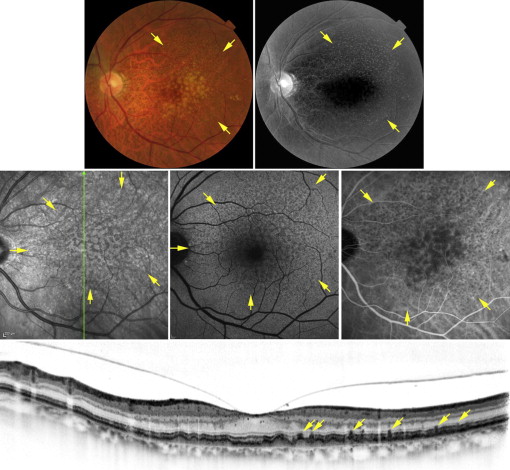
First, the quality of each image was evaluated by an experienced ophthalmologist (N.U.A.) and patients with adequate image quality in both eyes were included. Image quality was evaluated twice on all other days, and only images having an eligible quality during both evaluations were used. All these images were evaluated for the detection of reticular pseudodrusen by 2 independent experienced ophthalmologists (N.U.A. and S.O.). The evaluation of each image was performed referring to the corresponding images obtained from other imaging modalities. FA images were also referred to in order to distinguish reticular drusen from other lesions such as basal laminar drusen. In case of any discrepancy, a third experienced ophthalmologist (A.T.) was asked to arbitrate. In the current study, eyes diagnosed as having reticular pseudodrusen were those with reticular patterns in more than 2 of the following: the blue channel image of color fundus photography, IR, FAF, or SD OCT. For the blue channel of contrast-enhanced color fundus photography, a reticular pattern was identified as light interlacing networks that were 125-250 μm wide ( Figure 1 ). Reticular autofluorescence was defined as a group of ill-defined, hypofluorescent lesions against a background of mildly elevated AF ( Figure 1 ). Reticular IR was defined as a group of hyporeflectant lesions against a background of mild hyperreflectance with analogous characteristics ( Figure 1 ). SD OCT reticular lesions were defined as ≥5 hyperreflective mounds or triangular lesions above the RPE in ≥1 B-scan ( Figure 1 ).
Genotyping
Genomic DNA was prepared from leukocytes of peripheral blood with a DNA extraction kit (QuickGene-610L; Fujifilm, Tokyo, Japan). Of the 216 patients who met the inclusion criteria, genomic data from 11 patients were not available because of the following reasons: (1) consensus of blood extraction was not achieved; (2) genotyping was not possible because of the preservation state. Thus, analyses for genomic data were limited to 205 patients. We genotyped the major AMD-associated single nucleotide polymorphism (SNP), CFH Y402 rs1061170, I62 V rs800292, and ARMS2 A69S rs10490924. The SNPs were genotyped using TaqMan SNP assays with the ABI PRISM 7700 system (Applied Biosystems Inc, Foster City, California, USA), according to the manufacturer’s instructions.
Statistical Analysis
Statistical analysis was performed using SPSS 17 software (SPSS Inc, Chicago, Illinois, USA). All values are presented as a mean ± standard deviation (SD). For statistical analysis, visual acuity measured using a Landolt chart was converted to the logarithm of the minimal angle of resolution (logMAR). Mann-Whitney U tests were used to compare data from 2 groups in which normal distributions were not verified. To compare ratios between the 2 groups, χ 2 tests were used. P < .05 was considered statistically significant.
Results
In this study, data of 249 consecutive patients with late AMD were retrospectively reviewed; however, 5 patients with an eye with phthisis bulbi and 28 patients with poor image quality were excluded. (The intraobserver agreement for grading of image quality was 94.6%.) Thus, 216 patients were included in this study. All patients were Japanese. The patients comprised 161 men and 55 women, aged 51-92 years (mean ± SD, 73.9 ± 8.7). Among them, 97 patients (44.9%) had typical AMD, 87 (40.2%) had PCV, 12 (5.6%) had RAP, and 12 (5.6%) had geographic atrophy. Eight patients had a different type of late AMD in both eyes that was defined as “combined.” (Four patients had typical AMD in 1 eye and PCV in the other eye. The other combinations were typical AMD and geographic atrophy, typical AMD and RAP, geographic atrophy and PCV, and geographic atrophy and RAP. The visual acuity of these patients ranged from 20/2000 to 20/12 (mean logMAR = 0.33 ± 0.52). Spherical equivalent refractive error ranged from -5.50 diopters (D) to +4.50 D in the eyes with late AMD, and ranged from -18.375 D to +3.875 D in the fellow eyes without late AMD (4 eyes with high myopia [<-6 D] were included in the fellow eyes). Sixty-eight eyes had pseudophakia. The characteristics of the participants are summarized in Table 1 .
| Typical AMD | PCV | RAP | Geographic Atrophy | Combined a | Total | |
|---|---|---|---|---|---|---|
| No. of patients (%) | 97 (44.9) | 87 (40.2) | 12 (5.6) | 12 (5.6) | 8 (3.7) | 216 (100) |
| Sex, n (%) | ||||||
| Men | 76 (78) | 70 (80) | 4 (33) | 7 (58) | 4 (50) | 161 (75) |
| Women | 21 (22) | 17 (20) | 8 (67) | 5 (42) | 4 (50) | 55 (25) |
| No. of affected eyes (%) | ||||||
| Two | 17 (18) | 9 (10) | 5 (42) | 9 (75) | 8 | 48 (22) |
| One | 80 (82) | 78 (90) | 7 (58) | 3 (25) | — | 168 (78) |
| Age (mean ± SD) | 74.8 ± 8.3 | 71.5 ± 8.4 | 81.3 ± 8.2 | 72.3 ± 9.3 | 82.3 ± 2.9 | 73.9 ± 8.7 |
a Patients with typical AMD, PCV, RAP, or geographic atrophy in 1 eye and another type of AMD in the other eye (4 typical AMD and PCV, 1 typical AMD and RAP, 1 typical AMD and geographic atrophy, 1 geographic atrophy and RAP, and 1 geographic atrophy and PCV).
Using color fundus photography, IR, FAF, or SD OCT, it was determined that out of 432 eyes, 30 eyes (6.9%), 65 eyes (15.0%), 45 eyes (10.4%), and 47 eyes (10.9%), respectively, had a reticular pattern. (Inter- and intraobserver agreements for grading for the detection of reticular pseudodrusen are shown in Table 2 .) Furthermore, 49 eyes (11.3%) of 30 patients had a reticular pattern according to ≥2 imaging modalities, and were defined as having reticular pseudodrusen. Reticular pseudodrusen was confirmed bilaterally in 19 of these 30 patients (63.3%) and unilaterally in 11 patients (36.7%). In all 11 patients with unilateral reticular pseudodrusen, the other eye had neovascular AMD (4 were RAP, 6 were typical AMD, and 1 was PCV). In 38 of 49 eyes (77.6%) with reticular pseudodrusen, a pattern of hyporeflective dots was detected in the middle- and late-phase IA corresponding to the reticular pattern detected in IR and FAF ( Figure 1 ).
| Blue Channel a | IR | FAF | SD OCT | |
|---|---|---|---|---|
| Intraobserver agreements | ||||
| Accordance rate (%) | 96.9 | 94.6 | 95.3 | 98.3 |
| Kappa coefficient (95% confidence interval) | 0.72 (0.57-0.86) | 0.78 (0.69-0.86) | 0.74 (0.63-0.85) | 0.91 (0.85-0.98) |
| Interobserver agreements | ||||
| Accordance rate (%) | 94.7 | 91.4 | 91.2 | 97.9 |
| Kappa coefficient (95% confidence interval) | 0.62 (0.47-0.76) | 0.64 (0.54-0.75) | 0.61 (0.50-0.72) | 0.89 (0.81-0.96) |
The characteristics of patients with reticular pseudodrusen (30 patients [13.9%]) and patients without reticular pseudodrusen (186 patients) are summarized in Tables 3 and 4 , respectively. Of the 30 patients with reticular pseudodrusen, 19 (63.3%) were women, whereas only 36 of 186 patients without reticular pseudodrusen (19.4%) were women ( P < .001, χ 2 test). The mean age of the patients with reticular pseudodrusen was 80.6 ± 6.8 years (range, 65-92 years), which was significantly higher than that of patients without reticular pseudodrusen (72.8 ± 8.5 years; range, 51-92 years; P < .001, Mann-Whitney test). In addition, 16 of 30 patients with reticular pseudodrusen (53.3%) had bilateral late AMD, whereas only 32 of 186 patients without reticular pseudodrusen (17.2%) had bilateral late AMD ( P < .001, χ 2 test). In patients over 70 years old, 15 of 28 patients with reticular pseudodrusen (53.6%) had bilateral late AMD, whereas 26 of 118 patients without reticular pseudodrusen (22.0%) had bilateral late AMD ( P = .001, χ 2 test).
| Typical AMD | PCV | RAP | Geographic Atrophy | Combined a | Total | |
|---|---|---|---|---|---|---|
| No. of patients | 9 | 2 | 10 | 6 | 3 | 30 |
| Sex, n (%) | ||||||
| Men | 5 (56) | 0 | 3 (30) | 2 (33) | 1 (33) | 11 (37) |
| Women | 4 (44) | 2 (100) | 7 (70) | 4 (67) | 2 (67) | 19 (63) |
| No. of eyes with AMD (%) | ||||||
| Two | 3 (33) | 0 (0) | 4 (40) | 6 (100) | 3 | 16 (53) |
| One | 6 (67) | 2 (100) | 6 (60) | 0 (0) | — | 14 (47) |
| Age (mean ± SD) | 79.1 ± 6.6 | 82.0 ± 4.2 | 82.4 ± 7.7 | 78.3 ± 8.0 | 83.0 ± 2.6 | 80.6 ± 6.8 |
a Patients with typical AMD, PCV, RAP, or geographic atrophy in 1 eye and another type of AMD in the other eye (1 RAP and GA, 1 AMD and RAP, and 1 AMD and PCV).
| Typical AMD | PCV | RAP | Geographic Atrophy | Combined a | Total | |
|---|---|---|---|---|---|---|
| No. of patients | 88 | 85 | 2 | 6 | 5 | 186 |
| Sex, n (%) | ||||||
| Men | 71 (81) | 70 (82) | 1 (50) | 5 (83) | 3 (60) | 150 (81) |
| Women | 17 (19) | 15 (18) | 1 (50) | 1 (17) | 2 (40) | 36 (19) |
| No. of eyes with AMD (%) | ||||||
| Two | 14 (16) | 9 (11) | 1 (50) | 3 (50) | 5 (100) | 32 (17) |
| One | 74 (84) | 76 (89) | 1 (50) | 3 (50) | — | 154 (83) |
| Age (mean ± SD) | 74.2 ± 8.3 | 71.3 ± 8.4 | 76.0 ± 11.3 | 66.2 ± 6.2 | 81.8 ± 3.3 | 72.8 ± 8.5 |
a Patients with typical AMD, PCV, RAP, or geographic atrophy in 1 eye and another type of AMD in the other eye (1 RAP and geographic atrophy, 1 AMD and RAP, and 1 AMD and PCV).
The prevalence rate of reticular pseudodrusen was different according to the disease type of late AMD: 10 of 12 patients with RAP (83.3%), 6 of 12 patients with geographic atrophy (50.0%), 9 of 97 patients with typical AMD (9.2%), 2 of 87 patients with PCV (2.2%), and 3 of 8 patients with combined subtype ( Table 5 ). In patients over 70 years old, the prevalence of reticular pseudodrusen was 10 of 11 patients with RAP (90.9%), 5 of 7 patients with geographic atrophy (71.4%), 8 of 67 patients with typical AMD (11.9%), and 2 of 53 patients with PCV (3.8%) ( Supplemental Table , available at AJO.com ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


