Purpose
To determine whether a significant correlation exists between the presence of a bulge in the photoreceptor inner segment/outer segment (IS/OS) line and the best-corrected visual acuity (BCVA) in eyes with resolved macular edema associated with branch retinal vein occlusion (BRVO).
Design
Retrospective, observational case series.
Methods
We retrospectively reviewed the medical records of patients who had a complete resolution of macular edema and had an intact IS/OS line in the central fovea in the spectral-domain optical coherence tomographic (SDOCT) images. Thirty-one eyes with macular edema associated with BRVO (BRVO group) and 31 unaffected fellow eyes (control group) of 31 patients were evaluated. In normal eyes, the intact IS/OS line determined by SDOCT has a bulge at the central fovea, called the foveal bulge. The eyes in the BRVO group were classified by the presence or absence of foveal bulge, and the characteristics of the 2 groups were compared.
Results
A foveal bulge was present in 7 of 31 eyes in the BRVO group. The incidence of a foveal bulge was significantly lower in the BRVO group (22.6%) than in the control group (100%; P < .0001). All 7 eyes with foveal bulge had a decimal BCVA of ≥1.0 at the final visit. The incidence of a foveal bulge was significantly higher in eyes with BCVA of ≥1.0 (77.8%) than in the eyes with BCVA of <1.0 (0%; P < .0001).
Conclusions
The foveal bulge is a good marker of the functional properties of the fovea in eyes with resolved macular edema associated with BRVO.
Macular edema is a major complication associated with branch retinal vein occlusion (BRVO). The macular edema occasionally resolves spontaneously, but it can also remain for a long period and lead to a decrease in visual acuity. Thus, various treatments have been used to try to reduce macular edema, such as grid laser photocoagulation, pars plana vitrectomy combined with internal limiting membrane peeling, intravitreal injections of triamcinolone acetonide, and intravitreal injections of bevacizumab or ranibizumab. After resolution of the macular edema, the visual acuity of most of the eyes recovers to a relatively good level. However some patients have poor visual acuity in spite of a complete resolution of the macular edema.
The reason for this lack of complete recovery was partially answered by the results of recent studies using spectral-domain optical coherence tomography (SDOCT). The SDOCT images showed that the photoreceptor inner and outer segment (IS/OS) line was disrupted at the central fovea in the eyes of patients who had poor visual acuity despite complete resolution of the macular edema. It has also been shown that the integrity of the IS/OS line was significantly and positively correlated with visual acuity in eyes with resolved macular edema associated with BRVO. However, we have examined patients who had only limited visual improvement, although their eyes had an intact IS/OS line at the central fovea after resolution of the macular edema. We were not able to determine why the visual acuity did not completely recover in these eyes.
Careful examination of the SDOCT images of normal eyes shows that the IS/OS line has a bulge at the central fovea, named a foveal bulge. Recent OCT studies have shown that the presence or absence of a foveal bulge at the central fovea was significantly correlated with visual acuity in eyes with albinism, occult macular dystrophy, and amblyopia. However, as best we know, no study has reported on the presence or absence of a foveal bulge in eyes with BRVO.
Thus, the purpose of this study was to determine whether the foveal bulge was significantly correlated with visual acuity after resolution of the macular edema associated with BRVO. In addition, we studied the macular status at the initial visit and assessed the factors related to visual acuity after resolution of the macular edema.
Patients and Methods
Procedures and Patients
The procedures used in this study conformed to the tenets of the Declaration of Helsinki. Treatment of an intravitreal injection of bevacizumab was approved by the Institutional Review Board for Nara Medical University. An informed consent was obtained from all of the patients after an explanation of the procedures to be used and possible complications.
We studied the medical records of patients with a resolved macular edema associated with BRVO and with an intact IS/OS line at the central fovea in the SDOCT images. All of the patients were examined at the Nara Medical University Hospital from June 1, 2011 to April 30, 2013. Eyes with coexisting ocular diseases (eg, epiretinal membrane, glaucoma, diabetic retinopathy, vitreous hemorrhage, vitreous opacity, and senile cataract) were excluded. In the end, 31 eyes of 31 patients with macular edema associated with BRVO (BRVO group) were studied. We also studied the 31 unaffected fellow eyes as controls (control group). Twenty-seven of the 31 affected eyes received an intravitreal injection of bevacizumab and a posterior sub-Tenon injection of triamcinolone acetonide to treat the macular edema. The macular edema resolved spontaneously in the other 4 eyes. All of the patients underwent a complete ophthalmic examination including the measurement of the best-corrected visual acuity (BCVA), slit-lamp biomicroscopy, fundus examination including slit-lamp biomicroscopy with a noncontact fundus lens, fundus photography, and SDOCT.
Evaluation of Optical Coherence Tomographic Images
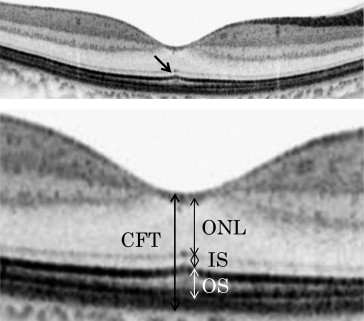
The Spectralis SDOCT (Heidelberg Engineering, Heidelberg, Germany) was used to obtain the SDOCT images. We evaluated the horizontal cross-sectional images that were recorded at the initial and final visit after resolution of the macular edema. The central foveal thickness (CFT) was measured as the distance between the internal limiting membrane (ILM) and the outer border of the retinal pigment epithelium (RPE) at the central fovea. The CFT was measured automatically with the caliper measurement tool embedded in the SDOCT system ( Figure 1 ). We also measured the outer nuclear layer (ONL) thickness as the distance between the outer border of the ILM and the external limiting membrane (ELM), and the photoreceptor inner segment (IS) length as the distance between the ELM and the inner border of the highly reflective line representing the IS/OS line at the central fovea. The photoreceptor outer segment (OS) length was measured as the distance between the IS/OS line and the inner border of the RPE at the center of the fovea ( Figure 1 ). The ONL thickness and the photoreceptor IS and OS lengths were measured manually by 2 of the authors (T.H. and M.O.), who were masked to the visual acuity and other information of the eyes. The values obtained by the 2 authors were averaged for the statistical analyses. The intraclass correlation coefficient (ICC) was calculated as an interobserver reproducibility measure.
We focused on the foveal bulge as seen in normal eyes ( Figure 1 ) in the 31 BRVO eyes of 31 patients. The eyes were classified into those with a foveal bulge and those without a foveal bulge. The same retinal specialists (T.H. and M.O.) evaluated the foveal shape in the OCT images and were masked to the clinical characteristics of the eyes, and a third reviewer (T.U.), who was also masked to the patients’ data, made the final decision regarding the presence or absence of a foveal bulge in cases of disagreement.
Statistical Analyses
Statistical analyses were performed using StatView software (version 5.0; SAS Institute, Cary, North Carolina, USA). The BCVA was measured with a Landolt chart, and the decimal acuities were converted to the logarithm of the minimal angle of resolution (logMAR) for the statistical analyses. All values are presented as the means ± standard deviations. The Mann-Whitney U test was used to determine the significance of differences in the patient characteristics and the retinal thicknesses. The significance of the differences in the incidence of an intact the ELM, presence of serous retinal detachment (SRD), and foveal bulge was analyzed with the Fisher exact probability test. A P value <.05 was considered statistically significant.
Results
The interobserver ICC for the measurement of the ONL thickness was 0.957, for the photoreceptor IS length was 0.871, and for the photoreceptor OS length was 0.970. These findings suggest that the measurement of each retinal layer had good reproducibility.
The average age of the 31 patients (15 men and 16 women) was 67.3 ± 8.6 years, with a range of 49-81 years. At the initial visit, all 31 affected eyes had macular edema associated with BRVO, and the macular edema had resolved completely and an intact IS/OS line was observed at the central fovea in the SDOCT images in all of the cases.
Comparisons Between Control Group and Branch Retinal Vein Occlusion Group
The clinical characteristics of the eyes in the BRVO group and control fellow eyes at the final visit are summarized in Table 1 . In the BRVO group, the mean BCVA was 0.18 ± 0.22 logMAR units with a range of −0.08 to 0.52 logMAR units, the mean CFT was 221.8 ± 20.5 μm, and the mean photoreceptor OS length at the central fovea was 47.3 ± 9.4 μm. For the eyes in the control group, the mean BCVA was −0.03 ± 0.05 logMAR units, the mean CFT was 221.2 ± 15.9 μm, and the mean photoreceptor OS length was 58.5 ± 4.2 μm. The BCVA in eyes of the control group was significantly better than that in eyes of the BRVO group ( P < .0001). The photoreceptor OS length in eyes of the BRVO group was significantly shorter than that in eyes of the control group ( P < .0001), but the CFT, ONL thickness, and photoreceptor IS length were not significantly different between the eyes of the 2 groups.
| BRVO Group (n = 31) | Control Group (n = 31) | P Value | |
|---|---|---|---|
| Age (y) | 67.3 ± 8.6 | ||
| Follow-up period (mo) | 7.5 ± 4.3 | ||
| LogMAR | 0.18 ± 0.22 | −0.03 ± 0.05 | <.0001 |
| CFT (μm) | 221.8 ± 20.5 | 221.2 ± 15.9 | .8880 |
| ONL thickness (μm) | 106.3 ± 11.8 | 101.6 ± 15.5 | .1314 |
| Photoreceptor IS length (μm) | 28.1 ± 1.6 | 28.0 ± 2.8 | .5375 |
| Photoreceptor OS length (μm) | 47.3 ± 9.4 | 58.5 ± 4.2 | <.0001 |
| Detection of foveal bulge n (%) | 7 (22.6%) | 31 (100%) | <.0001 |
In the control group, a foveal bulge was present in all 31 eyes (100%) at the final visit, but a foveal bulge was present in 7 eyes (22.6%) and absent in 24 (77.4%) in the BRVO group at the final visit. This difference in the incidence of a foveal bulge at the final visit was significant ( P < .0001).
Comparisons of Eyes With or Without Foveal Bulge in Branch Retinal Vein Occlusion Group
At the final visit, a foveal bulge was present in 7 and not present in 24 eyes of the BRVO group. The clinical characteristics of the eyes in the foveal bulge (+) group (n = 7) and foveal bulge (−) group (n = 24) are presented in Table 2 . At the final visit in the foveal bulge (+) group, the mean BCVA was −0.06 ± 0.04 logMAR units, the mean CFT was 237.0 ± 17.7 μm, and the mean photoreceptor OS length at the central fovea was 58.6 ± 3.8 μm. In the foveal bulge (−) group, the mean BCVA was 0.24 ± 0.21 logMAR units, the mean CFT was 217.3 ± 19.3 μm, and the mean photoreceptor OS length was 44.0 ± 7.8 μm at the final visit. At the final visit, the BCVA was significantly better in the foveal bulge (+) group than in the foveal bulge (−) group ( P < .0001). The CFT was significantly thicker and the photoreceptor OS length was significantly longer in the foveal bulge (+) group than in the foveal bulge (−) group ( P = .0248, P = .0001, respectively). On the other hand, the ONL thickness and photoreceptor IS length were not significantly different in the 2 groups.
| Foveal Bulge (+) (n = 7) | Foveal Bulge (−) (n = 24) | P Value | |
|---|---|---|---|
| Age (years) | 59.1 ± 12.1 | 69.7 ± 5.6 | .0440 |
| Follow-up period (months) | 8.4 ± 5.4 | 7.3 ± 4.0 | .7210 |
| Initial examination | |||
| LogMAR | 0.14 ± 0.13 | 0.45 ± 0.27 | .0034 |
| CFT (μm) | 300.4 ± 76.3 | 560.1 ± 168.6 | .0011 |
| Disrupted ELM n (%) | 1 (14.3%) | 17 (70.8%) | .0124 |
| Detection of SRD n (%) | 1 (14.3%) | 20 (83.3%) | .0017 |
| Detection of foveal bulge n (%) | 6 (85.7%) | 1 (4.2%) | <.0001 |
| Final examination | |||
| LogMAR | −0.06 ± 0.04 | 0.24 ± 0.21 | <.0001 |
| CFT (μm) | 237.0 ± 17.7 | 217.3 ± 19.3 | .0248 |
| ONL thickness (μm) | 110.5 ± 10.7 | 105.0 ± 12.1 | .3443 |
| Photoreceptor IS length (μm) | 28.8 ± 1.6 | 27.9 ± 1.6 | .2631 |
| Photoreceptor OS length (μm) | 58.6 ± 3.8 | 44.0 ± 7.8 | .0001 |
We also studied the differences in the age, BCVA, and OCT findings at the initial examination between the foveal bulge (+) group and the foveal bulge (−) group. The patients in the foveal bulge (+) group were significantly younger than those in the foveal bulge (−) group ( P = .044). The BCVA was significantly better and the CFT was significantly thinner in the foveal bulge (+) group than that in the foveal bulge (−) group ( P = .0034, P = .0011, respectively). At the initial visit, a disrupted ELM was present in 1 of 7 eyes (14.3%) in the foveal bulge (+) group but was disrupted in 17 of 24 eyes (70.8%) in the foveal bulge (−) group. In addition, an SRD was detected beneath the fovea in only 1 of 7 eyes (14.3%) in the foveal bulge (+) group, but in 20 of 24 eyes (83.3%) in the foveal bulge (−) group. The incidence of a disrupted ELM in the foveal bulge (+) group was significantly lower than that in the foveal bulge (−) group ( P = .0124), and the incidence of an SRD in the foveal bulge (+) group was also significantly lower than that in the foveal bulge (−) group ( P = .0017). At the initial visit, the foveal bulge could be detected in 6 of 7 eyes (85.7%) in the foveal bulge (+) group, but the foveal bulge could be detected in only 1 of the 24 eyes (4.2%) in the foveal bulge (−) group ( P < .0001).
Correlations Between Clinical Characteristics and Final Visual Acuity
We classified 31 BRVO eyes into eyes with a decimal BCVA of ≥1.0 (n = 9) and eyes with a decimal BCVA of <1.0 (n = 22; Table 3 ). Seven of 9 eyes (77.8%) with a decimal BCVA of ≥1.0 had a foveal bulge after resolution of the macular edema. In eyes with a decimal BCVA of <1.0, none had a foveal bulge. This difference in the number of eyes with a foveal bulge after resolution of the macular edema was significant ( P < .0001). Furthermore, the initial clinical characteristics (eg, age, BCVA, CFT, integrity of the ELM, SRD, and foveal bulge) were significantly different in the eyes with a decimal BCVA of ≥1.0 and the eyes with BCVA of <1.0.
| Decimal BCVA of ≥1.0 (n = 9) | Decimal BCVA of <1.0 (n = 22) | P Value | |
|---|---|---|---|
| Age (y) | 59.8 ± 10.6 | 70.4 ± 5.2 | .0088 |
| Follow-up period (mo) | 7.9 ± 4.8 | 7.3 ± 4.1 | .8780 |
| Initial examination | |||
| LogMAR | 0.14 ± 0.14 | 0.48 ± 0.27 | .0005 |
| CFT (μm) | 343.0 ± 167.8 | 566.3 ± 155.9 | .0017 |
| Disrupted ELM n (%) | 2 (22.2%) | 16 (72.7%) | .0166 |
| Detection of SRD n (%) | 2 (22.2%) | 19 (86.4%) | .0013 |
| Detection of foveal bulge n (%) | 6 (66.7%) | 1 (4.5%) | .0007 |
| Final examination | |||
| LogMAR | −0.04 ± 0.04 | 0.27 ± 0.21 | <.0001 |
| CFT (μm) | 232.9 ± 18.0 | 217.2 ± 20.0 | .0476 |
| ONL thickness (μm) | 109.3 ± 9.6 | 105.1 ± 12.6 | .5136 |
| Photoreceptor IS length (μm) | 28.5 ± 1.5 | 28.0 ± 1.6 | .4558 |
| Photoreceptor OS length (μm) | 56.6 ± 6.1 | 43.5 ± 7.6 | .0002 |
| Detection of foveal bulge n (%) | 7 (77.8%) | 0 (0%) | <.0001 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


