Purpose
Adjunctive laser trabeculoplasty (LT) is an alternative to topical medications for open-angle glaucoma (OAG). The purpose was to: (1) identify predictors of LT vs glaucoma medication treatment; and (2) estimate the resource utilization and short-term costs associated with LT vs medication management.
Design
Retrospective administrative claims analysis.
Methods
Medical and pharmacy claims data between 2007 and 2012 were analyzed to identify prostaglandin analogue monotherapy OAG patients with an index date LT claim or second medication class claim. Patients were followed for 12 months pre-index and 24 months post-index. Predictive LT attributes included age, sex, employment status, medication adherence, comorbidity status, and geographic region. Short-term costs included glaucoma-specific and comprehensive healthcare encounters. Cohort comparisons were analyzed using χ 2 and Student t tests, logistic regression (predictive), and generalized linear models (cost).
Results
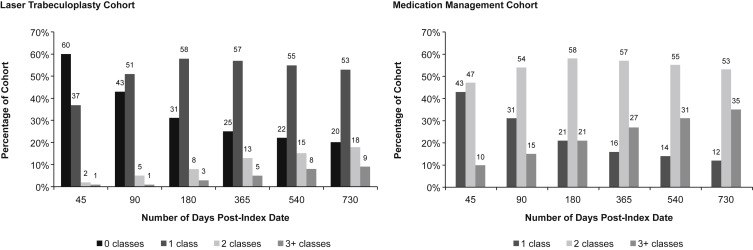
The study included 4743 LT and 16 484 medication patients. Baseline demographics were similar but significant differences were identified for comorbidities, adherence, and geography. Younger age (odds ratio [OR]: 1.21; P < .001), low adherence (OR: 1.18; P = .001), high comorbidities (OR: 1.12; P = .006), and region (OR: 1.50; P < .001) significantly predicted LT receipt. Within LT patients, 60% did not have a pharmacy claim 45 days post-index; by 2 years, this reduced to 20%. LT attributed significantly higher medical ($2684 vs $1980; P < .0001), lower pharmacy ($807 vs $1467; P < .0001), and greater overall costs ($3441 vs $3408; P = .325).
Conclusions
Poor adherence, younger age, and more comorbidities were predictors of receiving LT. Despite the potential for LT to address adherence, most patients had a medication claim within 2 years. Overall, LT does not provide glaucoma-specific cost savings.
Glaucoma is the world’s second-leading cause of blindness and affected nearly 45 million people in 2010. Owing to the world’s aging population, glaucoma is positioned to grow disproportionately, with estimates as high as 70-80 million cases by 2020. A recent study conducted in 2010 estimated glaucoma to be responsible for 8.5 million cases of blindness worldwide, and projections estimate this number will increase to 11.5 million by 2020. In North America, according to population data from the 2010 United States (US) Census, glaucoma affected nearly 2.22 million Americans and is expected to increase to 3.36 million by 2020. Owing to the aging US population, and the chronic nature of the disease, the future clinical and economic burden to the healthcare system is expected to increase.
Open-angle glaucoma (OAG) is the most prevalent form of the disease and is commonly associated with increased intraocular pressure (IOP) and visual field deterioration. OAG has several risk factors, but IOP is consistently targeted in disease screening protocols and pharmaceutical-based treatment algorithms. Disease management with topical drops is currently the predominant form of initial treatment, but advancements in ancillary procedures such as laser trabeculoplasty (LT) have provided clinicians more options. The procedure uses a laser to modify the framework of the trabecular meshwork to improve ocular outflow and decrease IOP. Even though studies have highlighted LT as a successful alternative to topical drops for lowering IOP, long-term efficacy remains questionable. The success rate of IOP-lowering effect at 4 years following the initial LT procedure ranges between 24% and 58%. Additionally, the success of repeat LT procedures is uncertain, with potential long-term implications of reverting back to topical medication therapy with disease progression.
Research and clinical practice guidelines have suggested LT to be a viable alternative for patients with poor medication adherence or incomplete response to topical therapy because it offers a similar efficacy profile. However, there is little published information concerning what type of patients are receiving LT in routine clinical practice. Additionally, the patient-level and healthcare system economic impact of LT has not been consistently reported. Seider and associates found LT to be a cost-saving alternative to pharmaceutical therapy, and it remains a procedure that is reimbursed by the US Medicare insurance system. In contrast, Pasquale and associates determined that LT patients incurred more healthcare costs overall. The uncertainty of real-world utilization, clinical effectiveness, and short-term economic impact has limited the understanding of LT utility in clinical practice.
The purpose of this study was 2-fold: (1) to examine patient-level predictors and outcomes associated with the receipt of LT vs being treated with strictly topical glaucoma medications (Rx) for patients who have failed monotherapy with prostaglandin analogue (PGA), and (2) to estimate resource utilization and costs associated with patients who receive LT compared with topical medication management.
Methods
Data Source and Time Period
The study design is a retrospective cohort claims analysis of administrative data from the Truven Health MarketScan Commercial Claims and Encounters Database. This study used inpatient, outpatient, and pharmacy between the time periods of January 1, 2007 to December 31, 2012. This source is composed of de-identified Health Insurance Portability and Accountability Act–compliant patient-level data, including inpatient, outpatient, pharmacy, laboratory, and dental claims; and insurance plan benefit design that covers both commercial insurance and Medicare supplemental insurance beneficiaries. The database encompasses approximately 150 million lives and is a conglomeration of almost 100 private sector, government, and public organization payers from all 50 United States. The comprehensive attributes of the database permit investigation of patient-specific clinical utilization, expenditures, and enrollment status across all areas of the healthcare delivery system. This analysis did not require human subjects review or institutional review board approval.
Patient Selection Criteria
Eligible study patients were required to be aged 18 years or older and maintain ≥36 months of continuous insurance coverage during the study. Patients were allocated to 2 study cohorts: (1) PGA monotherapy plus LT; or (2) PGA monotherapy plus the addition/switch to alternative glaucoma medication class. The patient-specific index date varied depending on the study cohort. The index date for LT cohort was defined by the first claim of LT (defined by Current Procedural Terminology [CPT] code 65855); the comparison cohort had an index date defined by the addition/switch to an alternative glaucoma medication class within 15 days of the last dispensed PGA.
The pre-index period had a defined length of 12 months and the post-index period was 24 months ( Figure 1 ). All patients were required to only have pharmacy claims for PGA monotherapy in the pre-index period. Study-specific inclusion criteria required at least 2 records of an OAG diagnosis, defined by International Classification of Diseases, Ninth Revision-Clinical Modification (ICD-9-CM), codes (365.01, 365.10, 365.11, 365.12, 365.13, 365.15) a minimum of 1 week apart in the pre-index period.

Outcome Measures
The outcome measures can be divided into the following 3 categories: resource utilization, predictive factors for LT, and economic outcomes. The resource utilization analyses described LT and Rx cohort treatment patterns over a 2-year post-index period. For LT cohort patients, the patient-specific quantity of LT claims and location of the procedure(s) were captured and categorized based on service location (physician office, ambulatory surgery center, outpatient hospital, or other). Additionally, cohort-specific medication utilization patterns were calculated and analyzed at various time points throughout the post-index period. The glaucoma medication classes were categorized into the following 7 categories: alpha agonists (AA), beta-blockers (BB), carbonic-anhydrase inhibitors (CAI), PGAs, fixed combinations, cholinergic, and “other.”
Predictive analyses sought to identify clinical and patient-level factors that may predict clinicians or patients to preferentially use LT over strictly medication management. Based on variables available in the dataset, factors included age, sex, geographic region, Charlson comorbidity index (CCI) score (categorized as 0, 1-2, or ≥3), and glaucoma medication adherence (calculated using proportion days covered [PDC] and defined as high [≥80%], moderate [≥20% to <80%], and low adherence [<20%]).
Economic outcomes analyses estimated medical, pharmacy, and total (medical plus pharmacy) short-term costs per patient throughout the 24-month post-index period. Costs were classified as glaucoma-specific (GS) and comprehensive; post-index date costs included index date costs. Comprehensive costs included all (medical or pharmacy) claims associated with each patient with respect to all healthcare-related claims (eg diabetes, heart failure, glaucoma, etc). GS costs were a proportion of comprehensive claims and only related to glaucoma diagnosis, maintenance, or treatment. These costs included pharmacy claims for glaucoma medications and outpatient medical claims defined by glaucoma-associated CPT codes ( Supplemental Table ; Supplemental Material available at AJO.com ). All costs were adjusted to 2015 dollars using the Medical Care Component of the Consumer Price Index.
Statistical Analyses
Baseline demographic patient characteristics were used to describe the cohorts and as covariates in multivariate regression models ( Table 1 ). Summary statistics (mean, standard deviation, proportions) were used to compare baseline demographic and resource utilization cohort characteristics. Statistically significant differences in demographics, resource utilization, and medication adherence were analyzed using χ 2 tests for proportions or Student t test for means; a P value ≤ .05 was defined as the type I error rate for statistical significance.
| Patient Characteristics | Laser Trabeculoplasty (n = 4743) | Medication Management (n = 16 484) | P Value |
|---|---|---|---|
| Age | |||
| <65 years | 48% | 47% | |
| ≥65 years | 52% | 53% | .31 |
| Mean (SD) | 65.6 (12.36) | 65.8 (12.63) | .46 |
| Sex | |||
| Male | 46% | 47% | |
| Female | 54% | 53% | .19 |
| Region | |||
| Northeast | 13% | 14% | |
| North Central | 41% | 30% | |
| South | 32% | 37% | |
| West | 14% | 19% | |
| Unknown | <1% | <1% | .001 |
| Employment status | |||
| Employed | 26% | 26% | |
| Retired | 74% | 74% | .63 |
| Insurance plan type | |||
| Comprehensive | 32% | 30% | |
| HMO a | 10% | 13% | |
| POS | 8% | 8% | |
| PPO | 49% | 48% | |
| CDHP/HDHP/EPO | 1% | 1% | .001 |
| CCI score b | |||
| 0 | 31% | 34% | |
| 1-2 | 45% | 44% | |
| ≥3 | 24% | 21% | .001 |
| Patient medication adherence c | |||
| <20% | 25% | 24% | |
| 20%-80% | 42% | 41% | |
| >80% | 32% | 34% | .01 |
| Comprehensive d | |||
| Medical (SD) | $6481 ($12 798) | $7405 ($18 937) | .0016 |
| Pharmacy (SD) | $3089 ($3921) | $2853 ($3671) | .001 |
| Glaucoma-specific e | |||
| Medical (SD) | $987 ($689) | $961 ($842) | .047 |
| Pharmacy (SD) | $414 ($279) | $402 ($288) | .0137 |
a Excluded in economic outcome models/estimates due to MarketScan cost estimation.
b Calculated at baseline using the CCI score.
c Medication adherence calculated in pre-index and post-index periods with the proportion days covered equation.
d All claims associated with each patient in pre-index period.
e Proportion of comprehensive costs specific to glaucoma disease management.
Pharmaceutical claims for the 7 glaucoma therapy classes were counted by patient within cohort at various time points in the post-index period, and reported as the cumulative proportion of unique glaucoma medication classes ( Figure 2 ). Multivariate logistic models examined the ability of patient characteristics to predict treatment utilization (LT or Rx); results of the logistic regression model were reported as odds ratios (OR) ( Table 2 ). Logistic regression model covariates included age, sex, employment status, geographic region, insurance plan type, PDC medication adherence, and CCI score categories. Generalized linear models (GLM) with a gamma distribution and log-link function were developed to predict the comprehensive and GS costs; results were reported as predicted patient-level costs ( Figure 3 ). Covariates in the GLM models were identical to those in the logistic regression model, but also included pre-index medical or pharmacy costs as presented in Table 1 .