Purpose
To predict eyelid height after frontalis suspension using autogenous fascia lata for congenital ptosis.
Design
Retrospective, observational case series.
Methods
Eighty eyes of 54 children who underwent frontalis suspension using autogenous fascia lata were included. The amount of intraoperative eyelid lift and the postoperative change in eyelid height were assessed 6 months after surgery by reviews of photographs and medical records. The amount of operative eyelid lift was measured from 2 different baselines, and each amount was compared with the amount of real change in eyelid height after surgery. The difference between those was measured.
Results
The postoperative eyelid height stabilized 3 months after surgery. The average amount of operative eyelid lift was 5.91 mm with anesthesia-induced lagophthalmos and 3.51 mm without. The amount of real change in eyelid height after surgery was 3.24 ± 1.14 mm. In less severe ptosis (< 3 mm of lift), an average operative lift of 2.03 mm resulted in 2.53 mm of elevation, whereas in more severe ptosis (≥ 4 mm of lift), an average operative lift of 3.98 mm resulted in only 3.72 mm of elevation 6 months after surgery. The preoperative palpebral fissure ( P = .002) and anesthesia-induced lagophthalmos ( P < .001) were significant factors influencing postoperative eyelid height.
Conclusions
Postoperative eyelid height may predicted be more accurately by compensating for anesthesia-induced lagophthalmos and adjusting the palpebral fissure to be larger than the desired eyelid height for patients with more severe ptosis.
First introduced by Payer and Wright, frontalis suspension surgery was popularized by Crawford, and numerous modifications in both the surgical technique and materials have occurred. This procedure is not only effective, but also is one of the most commonly used surgical interventions for patients with congenital ptosis and poor levator muscle function (LF).
Postoperative undercorrection or overcorrection remains a problem because most congenital ptosis surgery in children requires general anesthesia, which decreases the predictability of the procedure. The eyelid contour, including the fissure height, in the anesthetized condition varies significantly from the eyelid contour in the conscious state because of the influence of anesthetics and muscle relaxants. Some surgeons consider a patient’s LF and the degree of ptosis to determine the amount of intraoperative eyelid lift, although surgeons often rely on personal experience, as well.
The purpose of this study was to observe the change in the palpebral fissure (PF) quantitatively after frontalis suspension using autogenous fascia lata and to elucidate the factors influencing the postoperative change after the adjustment of eyelid height during surgery under general anesthesia.
Methods
This is a retrospective, noncomparative case series of consecutive pediatric patients with congenital ptosis. All patients underwent frontalis suspension using autogenous fascia lata under general anesthesia between January 2002 and December 2005. Both unilateral and bilateral cases were recruited for this study.
Patients with the following conditions were excluded from the study: neuromuscular diseases, such as cerebral palsy or cranial nerve paralysis; blepharophimosis; Marcus Gunn jaw-winking synkinesis; strabismus; history of previous ptosis surgery; and fewer than 6 months of follow-up.
Along with a detailed history of the ptosis, each patient underwent complete ophthalmic examination to determine the type of ptosis and to measure the PF and the preoperative LF. The amount of lagophthalmos that developed under general anesthesia (anesthesia-induced lagophthalmos) and the PF after adjustment of the eyelid height during surgery were measured. All measurements during surgery were performed using a caliper in 0.5-mm scales.
Patients were examined at 1 week, 1 month, 3 months, and 6 months after surgery and were photographed with a digital camera to analyze the progressive change in eyelid height. A circular tape with a diameter of 8 mm was placed in the middle of the glabella and was used as a guideline for the analysis ( Figure 1 ) . Physicians obtained photographs of each patient in primary gaze position without brow fixation. The PF was calculated from the ratio of the photographed fissure height to the size of the circular tape. The difference between the amount of eyelid elevation during surgery and the actual amount of eyelid elevation observed after surgery was analyzed.

Determining the Baseline
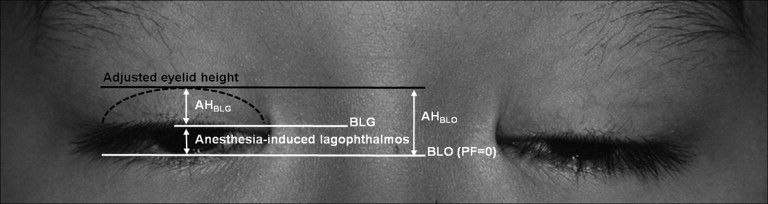
The preoperative baseline eyelid height initially was measured, followed by the amount of eyelid elevation during surgery. Two different baselines then were established: (1) at the level where the eye closed completely, which indicated a baseline PF of 0 (BLO), and (2) at the level of the anesthesia-induced lagophthalmos (BLG; Figure 2 ) .
Surgical Technique
All surgeries were performed according to a previously published technique using a direct tarsal and frontalis fixation using autogenous fascia lata. All surgeries were performed under general anesthesia with endotracheal intubation. The surgeon (S.Y.L.) determined the amount of intraoperative eyelid lift by the degree of ptosis. He adjusted the eyelid height of the ptotic eye for the difference of PF between the eye and contralateral nonptotic eye from the BLG in unilateral cases and from elevated eyelid height approximately 3 to 4 mm from the BLG in bilateral cases during surgery. The more severe the ptosis, the more eyelid lift was carried out. He placed the eyelid approximately 1 mm above the desired eyelid height for more severe degrees of ptosis based on his experience with less eyelid elevation in more severe ptosis.
Statistical Analysis
The amount of real change in eyelid height after surgery was calculated by subtracting the preoperative PF from the PF measured at the 6-month follow-up: ΔPF = (PF 6 months after surgery) − (preoperative PF). The amount of eyelid elevation performed during surgery was indicated by the adjusted eyelid height (AH). The AH with the baseline at BLO and BLG are indicated by AH BLO and AH BLG, respectively. The difference between the amount of intraoperative eyelid lift and the real change in PF after surgery is indicated by ΔPF − AH. A negative difference signifies that the real change in eyelid height 6 months after surgery was smaller than the amount of eyelid elevation performed during surgery, and a positive difference signifies that the postoperative change in eyelid height was larger than the adjusted amount during surgery.
Simple linear regression analysis was used to determine whether AH BLO or AH BLG better estimated the ΔPF. Postoperative PF changes were assessed by the paired t test. Univariate analysis was performed to identify the potential factors influencing the difference by the Wilcoxon signed-rank test. After confirming normality of the difference, multiple linear regression analysis was carried out to evaluate the factors influencing postoperative eyelid height. All statistical tests were 2-sided with an α level of 0.05 and were calculated using SPSS software version 13.0 (SPSS, Inc, Chicago, Illinois, USA).
Results
A total of 101 children underwent frontalis suspension using autogenous fascia lata during the study period, and 78 patients had at least 6 months of follow-up care. Among these, there were 20 patients with a history of ptosis surgery using polyfilament nylon (Supramid Extra; S. Jackson Inc, Alexandria, Virginia, USA) and 2 patients with undercorrection or overcorrection who were excluded. In addition, 2 more patients were excluded due to inadequate photographs. Finally, 80 eyes of 54 patients (53%), ranging in age from 3 to 14 years (mean, 5.6 years), were included in the study. Forty patients (74%) were male.
Twenty-eight patients had unilateral ptosis and 26 patients had bilateral ptosis. The mean preoperative PF and mean preoperative LF were 4.37 ± 1.25 mm and 2.67 ± 1.28 mm, respectively. The patients showed an average of 2.41 mm of anesthesia-induced lagophthalmos. Four patients had persistent corneal erosions secondary to lagophthalmos, 1 had eyelid inversion, and 1 had granuloma formation.
Anesthesia-induced lagophthalmos was noted in 75 eyes (94%), and the distribution is shown in Table 1 . The mean overall amount of lagophthalmos in those 75 eyes was 2.57 ± 1.09 mm. In bilateral cases, there was no significant difference between the amount of lagophthalmos in each eye ( P = .650). There were positive correlations of anesthesia-induced lagophthalmos with age ( r = 0.394; P < .001) and preoperative PF ( r = 0.337; P = .002), but no significant correlation with LF ( P = .371).
| Anesthesia-Induced Lagophthalmos (mm) | Eyes (n) | Age (y) | Gender (M:F) | Preoperative PF (mm) | Preoperative LF (mm) | |
|---|---|---|---|---|---|---|
| Intervals | Mean ± SD | |||||
| 0 | 0 | 5 | 4.40 ± 1.52 | 4:1 | 3.08 ± 0.73 | 2.10 ± 0.74 |
| 0.5 to 1 | 0.86 ± 0.24 | 7 | 4.14 ± 1.07 | 5:2 | 3.43 ± 1.53 | 3.14 ± 1.86 |
| 1.5 to 2 | 1.74 ± 0.26 | 25 | 4.72 ± 1.51 | 18:7 | 4.50 ± 1.23 | 2.82 ± 1.46 |
| 2.5 to 3 | 2.78 ± 0.25 | 23 | 6.17 ± 2.10 | 18:5 | 4.29 ± 1.16 | 2.80 ± 1.07 |
| 3.5 to 4 | 3.63 ± 0.23 | 15 | 6.60 ± 2.72 | 10:5 | 4.83 ± 1.05 | 2.30 ± 1.10 |
| 4.5 to 5 | 4.90 ± 0.22 | 5 | 7.40 ± 4.16 | 4:1 | 5.26 ± 0.84 | 2.30 ± 1.10 |
The mean AH BLO and the AH BLG were 5.91 ± 1.21 mm and 3.51 ± 1.00 mm, respectively, and the mean ΔPF was 3.24 ± 1.14 mm, which was closer to the AH BLG ( Figure 3 ) . In addition, explanatory powers ( R 2 ) of AH BLO and AH BLG for predicting ΔPF were 0.101 and 0.323 from simple linear regression analysis, respectively. These results showed that setting baseline eyelid height with BLG was more accurate than BLO for predicting postoperative eyelid height. From this point, the eyelid height was evaluated with BLG as a baseline. Two patients who underwent bilateral suspension are presented in Figure 4 . Their eyelids had been adjusted not from the baseline of the eye closed completely, but rather from the baseline of anesthesia-induced lagophthalmos during surgery, and the postoperative outcomes were excellent.
Figure 5 demonstrates the chronological change of PF and difference. Mean preoperative PF was 4.37 ± 1.25 mm, and mean postoperative PFs were as follows: 6.94 ± 1.11 mm at 1 week, 7.47 ± 1.05 mm at 1 month, 7.61 ± 1.03 mm at 3 months, and 7.61 ± 1.04 mm at 6 months. The PF showed a trend of significant increases until 3 months after surgery ( P < .001 between PFs at 1 week and 1 month after surgery; P < .001 between 1 month and 3 months after surgery), and thereafter, the eyelid height stabilized ( P = .914 between 3 and 6 months after surgery).
The overall difference was −0.27 mm (95% confidence interval, −0.49 to −0.05]. Statistically, the real eyelid height change 6 months after surgery showed a significant difference from the intraoperative eyelid lift ( P = .019); however, the actual difference was only 0.27 mm.
The ΔPF changes over time depending on the AH BLG are presented in Table 2 . In eyes with relatively less severe ptosis elevating less than 3 mm of AH BLG (mean, 2.03 mm), ΔPF tended to be larger than AH BLG after surgery ( P = .029). However, in eyes with more severe ptosis elevating more than 4 mm of AH BLG (mean, 4.35 mm), ΔPF tended to be smaller than AH BLG after surgery ( P = .002).
| AH BLG (mm) | |||
| Interval | AH < 3 | 3 ≤ AH < 4 | 4 ≤ AH |
| Mean ± SD | 2.03 ± 0.77 | 3.18 ± 0.24 | 4.35 ± 0.45 |
| Eyes (n) | 15 | 28 | 37 |
| Preoperative values (mm) | |||
| PF | 4.95 ± 1.26 | 4.56 ± 0.99 | 3.98 ± 1.32 |
| LF | 3.13 ± 1.96 | 2.41 ± 1.09 | 2.68 ± 1.02 |
| Lagophthalmos a | 3.23 ± 1.13 | 2.82 ± 1.14 | 1.76 ± 0.98 |
| ΔPF (mm) | |||
| Postoperative 1 wk | 1.99 ± 1.26 | 2.33 ± 1.04 | 2.99 ± 1.25 |
| Postoperative 1 mo | 2.41 ± 1.16 | 2.84 ± 0.88 | 3.58 ± 1.02 |
| Postoperative 3 mos | 2.51 ± 1.14 | 2.97 ± 0.85 | 3.74 ± 1.12 |
| Postoperative 6 mos | 2.53 ± 1.13 | 2.98 ± 0.87 | 3.72 ± 1.14 |
| P value b | .029 | .263 | .002 |
a Anesthesia-induced lagophthalmos.
b P value between ΔPF and AH BLG by Wilcoxon signed-rank test.
Statistical analysis was carried out to identify which factors may influence the surgical outcome. The univariate analysis showed that gender ( P = .003 for female), preoperative PF ( P = .042 for 5 mm ≤ PF < 6 mm), preoperative LF ( P = .024 for 3 mm ≤ LF < 4 mm), and anesthesia-induced lagophthalmos ( P = .014 for 2 mm ≤ BLG < 3 mm) could be potential factors influencing the difference, and these potential factors were recategorized based on statistical and clinical significance for the multivariate analysis ( Table 3 ). Multiple linear regression analysis with adjustments for gender, preoperative PF, preoperative LF, and anesthesia-induced lagophthalmos showed that the preoperative PF ( P = .002) and anesthesia-induced lagophthalmos ( P < .001) were statistically significant factors influencing postoperative eyelid height. In cases of preoperative PF of at least 4 mm or anesthesia-induced lagophthalmos of less than 3 mm, the real heights of the eyelids after surgery were lower than the surgically adjusted levels (β = −0.321 and −0.386, respectively; Table 4 ).
| No. of Eyes | Difference (mm) a | P Value between ΔPF and AH BLG b | |
|---|---|---|---|
| Age (y) | |||
| < 4 | 15 | −0.20 (−1.00 to 1.00) | .841 |
| 4 to 5 | 13 | −0.50 (−1.05 to −0.15) | .116 |
| 5 to 6 | 16 | −0.40 (−1.40 to 0.38) | .078 |
| 6 to 7 | 14 | 0.00 (−0.43 to 0.23) | .683 |
| 7+ | 22 | −0.30 (−1.05 to 0.60) | .269 |
| Gender | |||
| Male | 59 | 0.00 (−1.00 to 0.60) | .233 |
| Female | 21 | −0.50 (−1.00 to −0.05) | .003 |
| Laterality | |||
| Unilateral | 28 | −0.05 (−1.18 to 0.40) | .175 |
| Bilateral | 52 | −0.35 (−1.00 to 0.38) | .090 |
| Preoperative PF (mm) | |||
| < 3 | 7 | 1.00 (−0.90 to 1.00) | .307 |
| 3 to 4 | 18 | 0.50 (−0.63 to 0.73) | 1.000 |
| 4 to 5 | 27 | −0.40 (−1.00 to 0.30) | .078 |
| 5 to 6 | 18 | −0.50 (−1.20 to 0.33) | .042 |
| 6+ | 10 | −0.55 (−1.63 to 0.08) | .123 |
| < 4 c | 25 | 0.20 (−0.65 to 1.00) | .587 |
| 4+ c | 55 | −0.40 (−1.00 to 0.30) | .002 |
| Preoperative LF (mm) | |||
| < 2 | 9 | 0.40 (0.10 to 1.00) | .123 |
| 2 to 3 | 36 | −0.30 (−0.98 to 0.38) | .111 |
| 3 to 4 | 20 | −0.85 (−1.48 to 0.23) | .024 |
| 4+ | 15 | −0.30 (−1.00 to 0.40) | .258 |
| < 3 c | 45 | 0.00 (−0.70 to 0.50) | .491 |
| 3+ c | 35 | −0.50 (−1.40 to 0.30) | .012 |
| BLG: anesthesia–induced lagophthalmos (mm) | |||
| < 1 | 7 | −1.10 (−1.10 to 0.10) | .061 |
| 1 to 2 | 18 | −0.40 (−0.78 to 0.48) | .319 |
| 2 to 3 | 22 | −1.00 (−1.43 to −0.23) | .014 |
| 3 to 4 | 24 | 0.10 (−0.28 to 0.83) | .191 |
| 4+ | 9 | 0.00 (−0.75 to 0.40) | .889 |
| < 3 c | 47 | −0.60 (−1.10 to 0.20) | .001 |
| 3+ c | 33 | 0.00 (−0.40 to 0.60) | .309 |
| Total | 80 | −0.27 ± 1.00 (−0.49 to −0.05) d | .019 e |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


