Purpose
To determine postoperative risk factors that influence long-term corneal graft survival.
Design
Prospective cohort study.
Methods
Nine-hundred one consecutive penetrating keratoplasty procedures for optical, therapeutic, or tectonic indications from the Singapore Corneal Transplant Study. Univariate and multivariate analysis was performed for postoperative risk factors; Cox proportional hazards regression with a time-dependent covariate was used for preoperative, intraoperative, donor, and postoperative risk factors in a combined model.
Results
Raised intraocular pressure (20.7%) was the most common complication, followed by rejection (18.2%), whereas glaucoma surgery (7.9%) and repeat grafting (7.3%) were the most common procedures after penetrating keratoplasty. The primary graft failure rate was 1.4%, and late failure was seen in 9.4% of eyes. In the combined regression model, rejection (hazard ratio [HR], 3.4; P = .00), microbial keratitis (HR, 3.6; P = .00), endophthalmitis (HR, 7.7; P = .00), primary disease recurrence (HR, 73.9; P = .00), wound dehiscence (HR, 2.8; P = .02), lid surgery (HR, 2.3; P = .02), glaucoma surgery (HR, 2.46; P = .02), and repeat grafting (HR, 3.2; P = .00) were the significant postoperative failure predictors; the significant preoperative and intraoperative factors identified were female gender, graft size of less than 7 mm and more than 9 mm, primary diagnosis, preoperative inflammation, and preexisting perforation.
Conclusions
Postoperative complications and operative procedures after grafting have an adverse effect on graft survival.
Preoperative, intraoperative, and postoperative risk factors affecting corneal graft survival have been described in numerous studies, mostly in white populations, but most studies evaluating postoperative risk factors assess risk factors individually, and there is a paucity of data from multivariate analyses on the interactions between the postoperative risk factors and preoperative or intraoperative factors that may predict graft survival.
The Singapore Corneal Transplant Study is an ongoing, prospective cohort study of all corneal transplantations performed at a tertiary care center in Singapore, and we recently reported on the indications, long-term survival rates, and preoperative and intraoperative risk factors for penetrating keratoplasty (PK) graft survival in the Singapore Corneal Transplant Study. The aims of this study were to determine possible postoperative complications and operative procedures that also may affect long-term graft survival and to assess their interactions with other previously reported risk factors for graft survival, so as to enable appropriate postoperative management or preventive strategies to be implemented in transplant patients to reduce graft failure rates.
Methods
The Singapore Corneal Transplant Study is an ongoing prospective cohort study spanning 18 years (1991 onward) and tracking more than 2750 consecutive corneal transplantations performed at the Singapore National Eye Centre, an ophthalmic tertiary referral center in Singapore that performs approximately 80% of all corneal transplantations in Singapore. Details of the study population and database composition have been described in an earlier publication evaluating only preoperative and intraoperative risk factors.
PK procedures performed before January 1, 2004 (total, 1130 consecutive cases) were included in the study to ensure sufficient follow-up with regard to graft survival analysis. To allow for accurate statistical analysis, only one graft per patient was selected randomly, leaving a total of 901 grafts. Randomization was performed using an Excel (Microsoft, Redmond, Washington, USA) random number generator. PK was defined as all grafting procedures involving full-thickness replacement of corneal tissue. All other forms of transplantation procedures were excluded from the analysis.
Generally, all patients with missing follow-up data were recalled for examination when possible. Cloudy graft or graft failure was defined as irreversible loss of optical clarity, with the date of onset of clouding selected at the time point of graft failure, with the precise clinical cause of failure as recorded by the surgeon in the case notes.
Postoperative Therapeutic Regimen
The general postoperative therapeutic regimen for the grafts involved commencement of topical prednisolone acetate 1% or dexamethasone phosphate 0.1% at 3-hour intervals along with either topical tobramycin, levofloxacin, or moxifloxacin. Topical cyclosporine generally was used as additional immunosuppression in high-risk cases (multiple grafts, therapeutic grafts where steroids were withheld for the first few weeks, eyes with significant vascularization, glaucoma, ocular surface disease), or as a steroid-sparing agent in cases of ocular hypertension. Topical steroids were tapered gradually to once daily by the end of 1 year, with antibiotic use in tandem stopped when steroid dosage was reduced to a twice-daily regimen (antibiotics were continued beyond 6 months in view of a greater risk of the occurrence of infective keratitis in our graft patients when they were concurrently receiving topical steroids). In low-risk grafts (eg, grafts performed for keratoconus, corneal scars, anterior stromal dystrophies), topical steroids were continued for at least 1 year, whereas in immunologically high-risk grafts, low-dose steroids were continued indefinitely without antibiotics. In cases of tectonic and therapeutic grafts, topical steroids generally were withheld for at least 1 week after surgery with the aim of reducing the risk of exacerbating a recurrence of infection.
Oral steroids were commenced in the perioperative period in immunologically high-risk grafts (vascularized corneas, repeat grafts) in those patients who consented and were fit for oral steroids and were tapered over 2 to 3 weeks in the postoperative period. In selected high-risk cases (based on individual surgeon preference, patient acceptance of therapy, as well as patient systemic fitness) and with appropriate risk-to-benefit ratio assessment and counseling, oral cyclosporine (2 to 4 mg/kg daily) was commenced after surgery and maintained empirically for 12 months unless systemic toxicities developed in the patient. Systemic mycophenolate mofetil was used in patients with contraindication to systemic cyclosporine or in patients in whom side effects from cyclosporine developed. Patients with clinical evidence of rejection were managed aggressively with a combination of oral prednisolone (1 mg/kg body weight) and topical prednisolone acetate 1% given at 1- to 2-hour intervals, with rapid tapering after resolution of rejection.
Risk Factors Analyzed
A total of 17 potential postoperative risk factors were identified. These included 9 postoperative graft complications (epithelial problems, wound dehiscence, suture abscess, endophthalmitis, microbial keratitis, reactivation of herpes simplex infection, recurrence of primary disease, glaucoma or raised intraocular pressure [IOP], and allograft rejection) and 8 postoperative surgical or laser procedures (glaucoma surgery or laser procedures, repeat corneal grafting, graft resuturing, various forms of graft refractive surgery, cataract surgery, eyelid procedures, yttrium–aluminum–garnet capsulotomy, and vitreoretinal surgery). In addition, multivariate analysis involving inclusion of other preoperative and intraoperative risk factors identified in an earlier study were combined with these postoperative risk factors for a final overall analysis.
Statistical Analysis
Kaplan-Meier survival analysis was conducted to analyze graft survival times for postoperative factors. Postoperative follow-up factors were categorized, highlighting reference categories for comparisons. The Kaplan-Meier product limit method was applied to generate individual survival curves with corresponding survival rates. To avoid time-dependent bias, Cox proportional hazards regression with time-dependent covariates was used to analyze follow-up risk factors (eg, complications and second surgery) associated with risk of graft failure. Proportional hazards assumption was tested to identify variables over time. The identified variables that violated the proportional hazards were controlled in the model during the analyses. In the combined preoperative, intraoperative, and postoperative follow-up model, age was tested for the proportional hazard assumption. Because age violated the assumption, in the final model, age was no longer treated as a fixed variable and was controlled for. Univariate analyses were conducted for each variable to assess the significance. The effect of each individual risk factor was quantified and reported as a hazard ratio (HR) compared with a referent group. The final models were adjusted for age, sex, and time-dependent factors that violated proportional hazard assumptions. The final models also were checked for colinearity among variables by inspecting the standard errors associated with each variable. The first model was tested for postoperative factors only, and the second model was tested for combined preoperative and postoperative factors. In the preoperative and postoperative factors, multivariate analysis age and primary diagnosis interaction also were taken into account as identified in the first article. A P value (2-tailed) of less than .05 was considered to be statistically significant. All analyses were conducted using Statistical Package for Social Sciences version 15.0 (SPSS, Inc, Chicago, Illinois, USA).
Results
Data on baseline demographic characteristics, follow-up duration, indications for surgery and preoperative diagnoses, and preoperative and intraoperative risk factors have been described in an earlier publication from the Singapore Corneal Transplant Study. The incidence of postoperative complications and surgical procedures performed after PK is summarized in Table 1 . Glaucoma or raised IOP was the most common complication in the postoperative period (187 eyes; 20.7%), followed by allograft rejection (164 eyes; 18.2%) and epithelial problems (141 eyes; 15.6%). Primary graft failure was seen in 13 (1.4%) cases.
| Frequency (n) | Percent (%) | |
|---|---|---|
| Complication | ||
| Glaucoma/raised intraocular pressure | 187 | 20.7 |
| Allograft rejection | 164 | 18.2 |
| Epithelial problems | 141 | 15.6 |
| Late graft failure | 85 | 9.4 |
| Microbial keratitis | 48 | 5.3 |
| Cataract formation | 32 | 3.5 |
| Wound dehiscence | 27 | 3.0 |
| Vitreoretinal (retinal detachment, macular pathologic features, diabetic retinopathy) | 26 | 2.9 |
| Posterior capsular opacity | 24 | 2.3 |
| Primary graft failure | 13 | 1.4 |
| Suture abscess | 12 | 1.3 |
| Activation of herpes simplex infection | 10 | 1.1 |
| Endophthalmitis | 6 | 0.7 |
| Recurrence of primary disease | 5 | 0.5 |
| Others | 5 | 0.5 |
| Surgical procedure | ||
| Glaucoma surgery | 71 | 7.7 |
| Repeat corneal graft | 66 | 7.3 |
| Graft resuturing | 51 | 5.7 |
| Refractive surgery | 36 | 4.0 |
| Cataract surgery | 34 | 3.8 |
| Lid procedures | 25 | 2.8 |
| YAG capsulotomy | 16 | 1.8 |
| Others: retinal laser (n = 9), vitreoretinal surgery (n = 8), ocular surface procedures (n = 10) | 27 | 3.0 |
The most common surgical procedure performed was glaucoma surgery (71 eyes; 7.7%). Of these, trabeculectomy (augmented with 5-fluorouracil or mitomycin C) was performed in 38 eyes (56.7%), glaucoma drainage device implantation was performed in 16 eyes (23.9%), and trans-scleral cyclophotocoagulation was performed in 12 eyes (17.9%). For 6 eyes, data on the type of glaucoma surgery were not available. Sixty-six eyes (7.3%) underwent repeat grafting, and 51 eyes (5.7%) required graft resuturing. Of the various laser procedures, neodymium:yttrium–aluminum–garnet laser capsulotomy was the most common, accounting for 1.8% of cases.
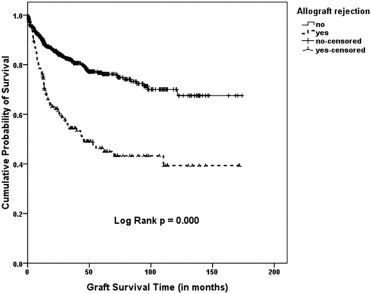
The presence of one or more postoperative risk factors reduced graft survival significantly ( P ≤ .001). The 1-, 3-, 5-, and 10-year survival rates for eyes without postoperative risk factors were 96.4%, 90.8%, 87.7%, and 85.3%, respectively, whereas for eyes with one or more postoperative risk factors, these were 78.8%, 58.6%, 48%, and 34.2%, respectively. In univariate analyses of postoperative risk factors, endophthalmitis, microbial keratitis, recurrence of primary disease, allograft rejection, regrafts, glaucoma surgery, and lid surgery were found to be significant predictors of graft failure, as depicted in the Kaplan-Meier survival curves ( Figures 1 and 2 ).
Postoperative risk factors significant in the univariate model were subjected to multivariate analyses using the Cox regression model. We further combined the previously described preoperative and intraoperative factors with the postoperative risk factors in a time covariate-dependent Cox regression model to determine risk factors of significance. The potential preoperative, intraoperative, and postoperative risk factors that were evaluated in this combined model are enumerated in Table 2 .
| Potential preoperative and intraoperative risk factors |
| Recipient gender |
| Recipient graft size |
| Primary diagnosis |
| Donor endothelial cell count |
| Pre-existing inflammation |
| Pre-existing glaucoma |
| Corneal neovascularization |
| Pre-existing corneal perforation |
| Potential postoperative risk factors |
| Postoperative infection/microbial keratitis |
| Endophthalmitis |
| Activation of herpes simplex virus |
| Glaucoma/raised intraocular pressure after penetrating keratoplasty |
| Recurrence of primary disease |
| Wound dehiscence |
| Allograft rejection |
| Cataract formation |
| Repeat corneal graft |
| Glaucoma surgery |
| Lid surgery |
| Refractive surgery |
| Nd:YAG laser capsulotomy |
In the final combined analysis ( Table 3 ), 13 risk factors were identified to be significant: female gender, primary diagnosis or indication for corneal graft, recipient graft size less than 7 mm and more than 9 mm, preoperative inflammation and perforation, postoperative microbial keratitis, endophthalmitis, recurrence of primary disease, allograft rejection, wound dehiscence, repeat corneal graft, glaucoma surgery, and lid surgery.
| 95% Confidence Interval for Hazard Ratio | ||||
|---|---|---|---|---|
| Risk Factor | P Value | Hazard Ratio | Lower | Upper |
| Recipient gender (female) | .00 | 1.64 | 1.18 | 2.29 |
| Recipient age | .94 | 1.00 | .83 | 1.22 |
| Recipient graft size (mm) | .00 | |||
| 7.5 to 7.9 | .00 | 5.15 | 2.01 | 13.23 |
| < 7 | .68 | 1.10 | .69 | 1.76 |
| 7 to 7.4 | .42 | 1.22 | .75 | 1.99 |
| 8 to 8.4 | .09 | .41 | .15 | 1.15 |
| 8.5 to 8.9 | .11 | 1.60 | .90 | 2.87 |
| Primary diagnosis | .00 | |||
| Keratoconus | 1 | |||
| Fuchs dystrophy | .01 | 14.83 | 1.85 | 118.61 |
| PBK/ABK | .00 | 22.95 | 3.03 | 174.14 |
| Active keratitis | .00 | 18.76 | 2.39 | 146.81 |
| Postinfection scar | .02 | 12.01 | 1.56 | 92.79 |
| Mechanical trauma | .01 | 13.91 | 1.78 | 109.09 |
| Regraft | .00 | 29.73 | 3.97 | 222.79 |
| Glaucoma | .01 | 17.52 | 2.08 | 147.76 |
| Others | .01 | 17.05 | 2.27 | 127.87 |
| Microbial keratitis (yes/no) | .00 | 3.64 | 2.19 | 6.06 |
| Activation of herpes simplex virus (yes/no) | .34 | .47 | .10 | 2.23 |
| Endophthalmitis (yes/no) | .00 | 6.74 | 2.43 | 18.70 |
| Glaucoma/raised intraocular pressure (yes/no) | .49 | .82 | .47 | 1.44 |
| Cataract formation (yes/no) | .00 | .15 | .035 | .62 |
| Allograft rejection (yes/no) | .00 | 3.45 | 2.42 | 4.92 |
| Wound dehiscence (yes) | .02 | 2.83 | 1.19 | 6.71 |
| Repeat corneal graft (yes/no) | .00 | 3.22 | 1.87 | 5.53 |
| Repeat wound suture (yes/no) | .64 | 1.19 | .57 | 2.45 |
| Glaucoma surgery (yes/no) | .02 | 2.46 | 1.12 | 5.40 |
| Cataract surgery (yes/no) | .02 | .23 | .07 | .77 |
| Nd:YAG capsulotomy (yes/no) | 0.02 | 0.29 | 0.00 | 0.83 |
| Lid surgery (yes/no) | .02 | 2.31 | 1.162 | 4.61 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


