Purpose
To evaluate a polyethylene glycol–based hydrogel bandage for its ability to secure sutureless pars plana vitrectomy sclerotomies.
Design
Laboratory investigation.
Methods
Twenty-gauge (20-G) and twenty-three gauge (23-G) sclerotomies were constructed in human cadaveric eyes. A total of 24 sclerotomies were constructed in 6 eyes. Four sclerotomies per eye were constructed. Two were straight 20-G incisions, of which 1 was sutured and 1 was covered with the bandage. The other 2 were 23-G beveled incisions, of which 1 was left bare and the other was closed with the hydrogel bandage. India ink was applied over the sclerotomy sites while the intraocular pressure (IOP) was varied. The presence of India ink particles along incisions was evaluated by histologic analysis.
Results
The hydrogel bandage prevented the entry of ink particles in all covered incisions after IOP modulation and incision manipulation. One 20-G sutured incision showed partial ink ingress. Four uncovered 23-G incisions showed the presence of ink within the inner aspect of the incisions ( P = .0455 relative to 23-G sealed incisions). Twenty-two out of 24 incisions were evaluated, as 2 incisions could not be identified on histologic analysis.
Conclusions
The use of a hydrogel bandage to close sutureless sclerotomies is a practical alternative to sutures. Closure of sutureless sclerotomies may reduce the entry of ocular surface fluid into these incisions as well as prevent leakage of intraocular fluid in the immediate postoperative period. Incision closure may reduce the incidence of postoperative endophthalmitis and hypotony in sutureless vitreous surgery.
Since its introduction, 25- and 23-gauge (G) microincisional vitrectomy surgery (MIVS) has evolved into a well established procedure. The indications for MIVS have expanded to include most posterior segment surgical situations as instrumentation has improved to rival traditional 20-G vitrectomy surgery. During MIVS, when required, 1 vitrectomy port is enlarged to accommodate a 20-G instrument in cases where certain instrumentation is lacking (silicone oil removal or phacofragmatome).
The widespread use of MIVS systems is evident by their popularity. In the 2008 Preferences and Trends survey (PAT survey) conducted by the American Society of Retina Specialists, approximately 71% of respondents used a MIVS system (23 or 25 G) 80% to 100% of the time when managing an epiretinal membrane without any other coexistent retinal abnormalities (Mittra RA, Pollack JS: ASRS Preferences and Trends Survey, 2008).
Although sutureless MIVS offers the patient clear advantages such as reduced procedure duration, quicker visual recovery from decreased corneal astigmatism, reduced anterior segment inflammation, reduced postoperative discomfort, and early patient rehabilitation, potential adverse postoperative events such as early hypotony and endophthalmitis are still concerns.
Endophthalmitis and hypotony are attributed to entry of ocular surface fluid or leakage of intraocular fluid via the vitrectomy incisions in the early postoperative period. Surgeons recognize this as a possible drawback when MIVS is used. As reported in the 2009 PAT survey, 36.48% of retinal surgeon respondents suture at least 1 of the sclerotomies in 23-G surgery 1% to 25% of the time and 15.05% of respondents place a suture 26% to 50% of the time (Mittra RA, Pollack JS: ASRS Preferences and Trends Survey, 2009).
In order to overcome potential complications related to wound leakage, wound closure with sutures, cyanoacrylate glue, tissue fibrin glue, and other complex adhesives have been suggested.
Suture placement prolongs operative time, requires conjunctival incisions, and induces corneal astigmatism, possibly delaying visual recovery. Furthermore, suture foreign body sensation compromises patient comfort. Cyanoacrylate glue produces heat and settles rapidly into an inflexible and friable material. Patients experience discomfort from the rough and anhydrous surface of cyanoacrylate glue, necessitating the use of a bandage contact lens when used for corneal indications. Tissue fibrin glue (Tisseel, Baxter AG, Vienna, Austria) has been used as an alternative to sutures in a small surgical case series for closure of MIVS and 20-G vitrectomy incisions. Fibrin glue carries the theoretical risk of anaphylaxis and disease transmission.
In situ polymerizing synthetic polymers containing polyethylene glycol are approved for use as dura mater sealants, lung sealants, and abdominopelvic adhesion barriers. These compounds can be engineered to form adherent hydrogel coatings of varying absorption, consistency, and flexibility depending on the indication of use.
We designed an in vitro study using fresh human cadaveric eyes to test a polyethylene glycol–based synthetic hydrogel ocular bandage (ReSure Ocular Bandage; Ocular Therapeutix Inc, Bedford, Massachusetts, USA) as a device to seal sutureless 23-G vitrectomy incisions as well as test the device’s ability to seal 20-G vitrectomy incisions that have traditionally been closed with sutures. India ink was used as a surrogate for bacteria as ink particles have comparable sizes to common ocular surface fluid microorganisms. Ink particles are also easily identified on histologic examination.
Methods
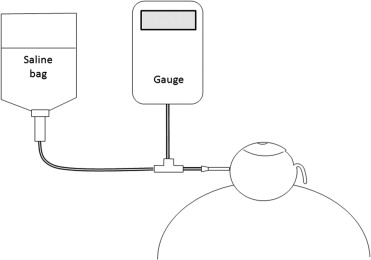
Six fresh intact whole human globes were obtained from the Michigan Eye Bank and were examined for the absence of conjunctiva. The experimental set-up consisted of a 16-G needle (BD 305197) inserted into the side of each globe and secured with cyanoacrylate glue (Permabond 910FS; Permabond Engineering Adhesives, Pottstown, Pennsylvania, USA) to prevent leakage. This was attached to a 3-way connector that communicated with a pressure gauge (Comark ITX-20; Comark Ltd, Hertfordshire, United Kingdom) and a saline-filled bag ( Figure 1 ).
All surgical procedures on the eyes were performed by an experienced vitreoretinal surgeon (S.M.H.). After ensuring physiological intraocular eye pressures, the globes were secured in a styrofoam dummy head mount. One 8-0 silk partial-thickness marker suture was placed in each quadrant, 6 mm posterior to the limbus, to facilitate incision identification during histologic processing. One incision in each quadrant was fashioned, 2 mm anterior from the marker suture, for a total of 4 incisions in each eye. Of these 4, 2 incisions were standard, straight 20-G vitrectomy incisions constructed with an MVR blade (EG-5560; Eagle Laboratories, Rancho Cucamonga, California, USA), of which 1 was sutured with 7-0 vicryl suture (Ethicon, Inc, Cornelia, Georgia, USA) and 1 was covered with hydrogel bandage. The other 2 incisions were beveled MIVS 23-G incisions (Alcon, Fort Worth, Texas, USA), of which 1 was covered with hydrogel and the other was left bare (no sutures or hydrogel bandage) ( Figure 2 ). In this manner, 4 groups of incisions with variable interventions were studied.

To investigate the potential for fluid ingress into the scleral wounds, 4 × 4-mm cut Weck-Cel sponges (Medtronic, Jacksonville, Florida, USA) were soaked in India ink (Sanford Corp, Bellwood, Illinois, USA) and placed over each of the 4 sclerotomy sites ( Figure 2 ). The ink concentration in the sponges was maintained by adding drops of ink onto the sponge with a syringe. The intraocular pressure (IOP) was then modulated between 0 and 30 mm Hg, 10 times, by raising and lowering the saline bag for a duration of 5 seconds at each pressure point in order to simulate lid blinking and lid manipulation. Following pressure modulation, all incisions were directly manipulated using the Weck-Cel sponge tip by applying pressure around the incision when the pressure was at zero. In this manner the incisions were exposed to the ink-soaked sponges for a total duration of approximately 5 minutes.
After the globes were subjected to the above-described IOP changes, the ink-soaked sponges were removed and the ocular surface was irrigated with saline to remove all surface ink particles. A dry Weck-Cel was used to confirm that no free India ink remained on the ocular surface.
The sclerotomy sites from each globe were excised and placed in individually marked formaldehyde-filled containers. Hematoxylin-eosin-stained sections of the specimen were made for light microscopy examination. The incisions from all groups were examined and photographed using a color digital photomicroscope (Olympus BX 41; Olympus Optical Co. Ltd, Nagano, Japan) at low (4×) and high (10×) magnification. An independent ophthalmic pathologist (M.H.) reviewed the slides in a masked fashion to determine the presence of India ink particles in the incision.
The difference in the ink ingress rate between groups was evaluated using the nonparametric McNemar test for paired data (NCSS Software, Kaysville, Utah, USA). A P value of less than .05 was viewed as statistically significant.
Results
The data from all groups is tabulated in the Table .
| Incisions Created | Gauge | Intervention | Ink in Incision on Histology |
|---|---|---|---|
| 6 a | 20 G | Suture only | 1/5 (20%) |
| 6 | 20 G | Hydrogel bandage only | 0/6 (0%) |
| 6 | 23 G | None (bare) | 4/6 (67%) b |
| 6 a | 23 G | Hydrogel bandage only | 0/5 (0%) b |
a Only 5 of 6 of the incisions were located in the histologic sections.
b Difference of ink ingress rates between 23-G bare incisions and 23-G sealed incisions was statistically significant ( P = .0455).
20-G Sclerotomy Sites With Sutures (No Hydrogel Bandage)
On histologic examination, 5 sclerotomies out of 6 were identified. Four of the samples had no ink in the incision, while 1 sample had ink particles up to the point of where the suture passed through the incision ( Figure 3 , Top).



