Ménière syndrome is an inner ear disorder characterized by spontaneous attacks of vertigo, fluctuating low-frequency sensorineural hearing loss, aural fullness and tinnitus. When the syndrome is idiopathic and cannot be attributed to any other cause (eg, syphilis, immune-mediated inner ear disease, surgical trauma), it is referred to as Ménière disease. This article reviews the physiologic effects of Ménière disease on vestibular function, as measured by caloric, head impulse, and vestibular-evoked myogenic potential testing.
Meniere’s syndrome is an inner ear disorder characterized by spontaneous attacks of vertigo, fluctuating low-frequency sensorineural hearing loss, aural fullness, and tinnitus. When the syndrome is idiopathic and cannot be attributed to any other cause (eg, syphilis, immune-mediated inner ear disease, surgical trauma), it is referred to as Meniere’s disease. Meniere’s syndrome exhibits a relapsing-remitting pattern, with episodic attacks terminated by periods of restitution to normal auditory and vestibular function. In addition, the natural history of Meniere’s syndrome is such that auditory and vestibular function typically decline with time.
Prosper Ménière first described this constellation of symptoms in 1861, and given the co-occurrence of auditory and vestibular phenomena, he proposed that the pathologic locus was the labyrinth. Subsequent investigations have corroborated his hypothesis: postmortem temporal bone analyses of individuals with Meniere’s syndrome showed histopathologic abnormalities in the labyrinth. In addition, physiologic tests of labyrinthine function were also found to be abnormal in these patients. This article reviews the physiologic effects of Meniere’s disease on vestibular function, as measured by caloric, head-impulse, and vestibular-evoked myogenic potential (VEMP) testing. The article begins by briefly outlining the central pathologic hypothesis behind Meniere’s disease (endolymphatic hydrops) insofar as this contributes to our understanding and interpretation of vestibular physiologic tests in Meniere’s disease.
Endolymphatic hydrops
Endolymphatic hydrops has long been held to be the pathologic basis for Meniere’s disease. Endolymph, the potassium-enriched fluid in the inner ear, may be either excessively synthesized or inadequately resorbed, resulting in expansion of the endolymphatic space. Surgical ablation of the endolymphatic sac in experimental animals has reproduced the histopathologic finding of endolymphatic hydrops seen in temporal bone specimens of individuals with Meniere’s disease, although these animals do not seem to experience the classic signs and symptoms associated with Meniere’s disease in humans.
Endolymphatic hydrops typically involves the pars inferior of the labyrinth (comprising the saccule and cochlea). Saccular hydrops may range from mild to severe, based on the degree of membrane distension toward the stapes footplate. Cochlear hydrops is typified by bowing of the Reissner membrane into the scala vestibuli; severity of cochlear hydrops also varies according to the degree of convexity toward the scalar wall of the modiolus. The pars superior (utricle and semicircular canals) may also be involved in endolymphatic hydrops, although changes tend to be less dramatic and occur less frequently.
Several mechanisms have been suggested to explain how endolymphatic hydrops may produce the spontaneous attacks of vertigo characteristic of Meniere’s disease. The most prominent theory holds that hydropic distension of the endolymphatic duct causes rupture of the distended membranes, a phenomenon that has been observed throughout the labyrinth. Membrane rupture allows the potassium-rich endolymph to leak into the perilymphatic space and contact the basal surface of the hair cells as well as the eighth cranial nerve. Initial excitation then subsequent inhibition of the hair cells manifest as a direction-changing nystagmus and may underlie the clinical phenotype of episodic vertigo.
Long-term declines in auditory and vestibular function may be the result of repeated exposure of the vestibular hair cells to toxic levels of potassium-enriched perilymph. The differential susceptibility of type I and type II hair cells in Meniere’s disease supports the hypothesis that chronic perilymph toxicity may cause neurosensory dysfunction. The vestibular neuroepithelium consists of type I and type II hair cells as well as supporting cells. Both hair cell types have cuticular plates and stereociliary bundles, reflecting their role in mechanosensory signal transduction. However, the 2 hair cell types can be distinguished based on other morphologic characteristics: Type I hair cells are flask-shaped, have a round nucleus, and are enveloped on their basal surface by an afferent nerve chalice. In contrast, type II hair cells are cylindrical, and have oval nuclei and small bouton-type nerve terminals from afferent and efferent nerve endings. The sparse nerve endings on the basal surface of type II hair cells may provide decreased protection against harmful ionic changes in the perilymph. The physiologic and functional implications of the selective depletion of type II hair cells in Meniere’s disease are still poorly understood.
Alternatively, it has been postulated that hydrops itself may occur in an episodic manner, as a result of sudden increases in the secretory function of the stria vascularis or of spontaneous obstruction of the endolymphatic sac. Hydropic distension may then cause a mechanical deflection of the macula and crista of the otoliths and semicircular canals, respectively, and thus vestibular hair cell depolarization, leading to the sensation of vertigo. Long-term changes to the neurosensory function of the vestibular apparatus may be the consequence of increased hydrodynamic pressure, causing increased vascular resistance, compromised blood flow, and chronic ischemic injury.
Several lines of evidence challenge the primacy of endolymphatic hydrops in the pathophysiology of Meniere’s disease. As mentioned previously, experimentally induced endolymphatic hydrops in animal models does not produce the clinical phenotype of Meniere’s disease in these animals. Moreover, a double-blind study of temporal bone specimens and associated clinical histories reported that all individuals with Meniere’s syndrome diagnosed during life had evidence of endolymphatic hydrops on postmortem examination of their temporal bones; however, not all individuals with histopathologic evidence of endolymphatic hydrops had clinical histories consistent with Meniere’s disease. If endolymphatic hydrops was central to the development of Meniere’s disease, one would expect the correlation between the clinical manifestations of Meniere’s disease and endolymphatic hydrops to be absolute.
Alternatively, studies increasingly suggest that endolymphatic hydrops may be a marker of some other pathologic process that causes Meniere’s disease, such as disordered cochlear homeostasis. Emerging evidence implicates the fibrocytes of the spiral ligament, which play a crucial role in maintaining cochlear fluid homeostasis; dysregulation of these cells seems to precede the development of hydrops. Triggers for cytologic changes in the fibrocytes remain elusive, although this line of inquiry shows promise for yielding the true pathologic basis for Meniere’s disease.
Caloric and head impulse testing in Meniere’s disease
Caloric and head impulse testing are both tests of semicircular canal function. In caloric testing, bithermal irrigation is applied to the external auditory canals, which causes a convective movement of endolymph within the ipsilateral horizontal semicircular canal. The movement of fluid within the horizontal canal results in excitatory or inhibitory deflection of the cupula (depending on the direction of endolymph flow). Motion of the cupula then leads to hair cell excitation or inhibition with a corresponding change in the discharge rate of vestibular-nerve afferents. Compensatory eye movements are thereby elicited (corresponding to the slow phases of nystagmus), followed by rapid corrective saccades (corresponding to the fast phase of nystagmus). The maximum velocities of the slow phases of nystagmus are compared bilaterally and used to compute unilateral weakness or caloric asymmetry. A caloric asymmetry of 20% or greater is usually considered to indicate unilateral peripheral vestibular hypofunction.
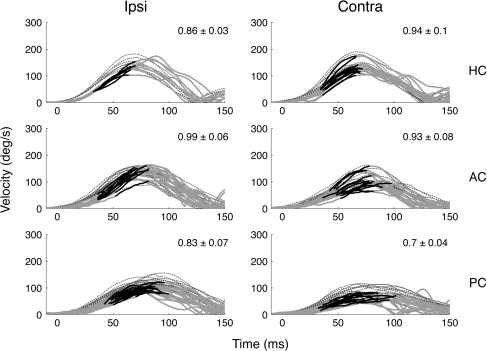
Head impulse (or head thrust) testing assesses the integrity of the three-dimensional angular vestibuloocular reflex (AVOR). Magnetic search coils are used to record head and eye movements during high-velocity, high-acceleration rotary head impulses in the plane excitatory for each of the 6 semicircular canals. Normal subjects are able to maintain visual fixation on a target during rapid head movement and thus have gain values (computed as the ratio of eye velocity to head velocity) close to 1.0.
A significant reduction in the caloric response of affected ears has been observed in 42% to 79% of individuals with unilateral Meniere’s disease, and caloric asymmetries of 100% (ie, absent caloric response in the affected ear) have been noted in 6% to 11% of patients. In contrast, abnormalities of the AVOR in Meniere’s disease are less prevalent. A study comparing caloric and head impulse testing in individuals with Meniere’s disease observed caloric testing abnormalities in 42% of subjects but AVOR abnormalities in only 13% of patients, although a significant linear correlation was noted between head impulse test gain asymmetry and caloric unilateral weakness percentage ( Fig. 1 ).
The results of caloric and head impulse testing in Meniere’s disease are informative. First, although caloric testing is pathologic, the normal AVOR gains in Meniere’s disease suggest that there is substantial preservation of semicircular canal function in these patients. In addition, although caloric and head impulse testing are measures of semicircular canal function, they seem to capture distinct phenomena. Caloric irrigation causes a slow convective flow of endolymph and provides a low-frequency stimulus to the vestibular system. In contrast, high-velocity rotary head thrusts cause rapid endolymph movement and generate a high-frequency input to vestibular afferents. It is possible that Meniere’s disease preferentially impairs the ability of the vestibular apparatus to process low-frequency signals. The low-frequency caloric stimulus is a nonphysiologic input, whereas the high-frequency head thrust does approximate a commonly occurring stimulus. Thus it is also possible that mechanisms of central adaptation can be established only for physiologic stimuli (leading to normal responses to head impulse testing) but not for inputs outside the normal range (ie, caloric stimuli).
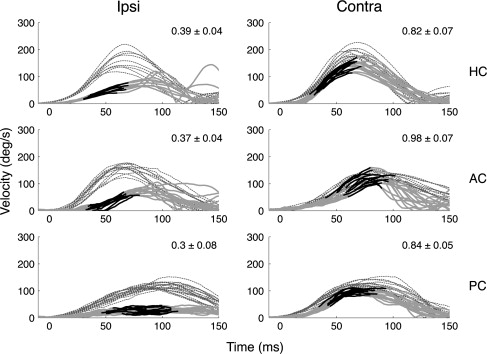
Further insight into the physiologic mechanisms of Meniere’s disease comes from studies of the effect of chemical ablation of the peripheral vestibular apparatus using intratympanic gentamicin. Studies suggest that successful and enduring ablative therapy indicates vertigo control: patients who sustained decreases in AVOR gain and increases in caloric weakness following intratympanic gentamicin were found to have fewer episodes of posttreatment vertigo and were less likely to require repeat therapy ( Fig. 2 ). However, the correlation between the loss of semicircular function and symptom control is not absolute. It is possible that the natural history of Meniere’s disease (typified by a high spontaneous remission rate) may obscure an association between decreased vestibular function and relief from vertigo symptoms. Alternatively, recurrent vertigo may in part reflect otolith function, which is not captured by caloric or head impulse testing.
Caloric and head impulse testing in Meniere’s disease
Caloric and head impulse testing are both tests of semicircular canal function. In caloric testing, bithermal irrigation is applied to the external auditory canals, which causes a convective movement of endolymph within the ipsilateral horizontal semicircular canal. The movement of fluid within the horizontal canal results in excitatory or inhibitory deflection of the cupula (depending on the direction of endolymph flow). Motion of the cupula then leads to hair cell excitation or inhibition with a corresponding change in the discharge rate of vestibular-nerve afferents. Compensatory eye movements are thereby elicited (corresponding to the slow phases of nystagmus), followed by rapid corrective saccades (corresponding to the fast phase of nystagmus). The maximum velocities of the slow phases of nystagmus are compared bilaterally and used to compute unilateral weakness or caloric asymmetry. A caloric asymmetry of 20% or greater is usually considered to indicate unilateral peripheral vestibular hypofunction.
Head impulse (or head thrust) testing assesses the integrity of the three-dimensional angular vestibuloocular reflex (AVOR). Magnetic search coils are used to record head and eye movements during high-velocity, high-acceleration rotary head impulses in the plane excitatory for each of the 6 semicircular canals. Normal subjects are able to maintain visual fixation on a target during rapid head movement and thus have gain values (computed as the ratio of eye velocity to head velocity) close to 1.0.
A significant reduction in the caloric response of affected ears has been observed in 42% to 79% of individuals with unilateral Meniere’s disease, and caloric asymmetries of 100% (ie, absent caloric response in the affected ear) have been noted in 6% to 11% of patients. In contrast, abnormalities of the AVOR in Meniere’s disease are less prevalent. A study comparing caloric and head impulse testing in individuals with Meniere’s disease observed caloric testing abnormalities in 42% of subjects but AVOR abnormalities in only 13% of patients, although a significant linear correlation was noted between head impulse test gain asymmetry and caloric unilateral weakness percentage ( Fig. 1 ).



