Purpose
To compare the long-term results of the efficacy of photodynamic therapy (PDT) with or without intravitreal bevacizumab (IVB) injections for polypoidal choroidal vasculopathy.
Design
Retrospective, comparative, interventional case series.
Methods
We included 69 eyes of 69 patients with macula-involved polypoidal choroidal vasculopathy. All patients were followed up for more than 2 years. We compared the treatment outcomes between groups and investigated the factors influencing visual improvement at 24 months of follow-up.
Results
Thirty-six patients received PDT combined with IVB and 33 patients received PDT monotherapy. At 3 months, the mean logarithm of minimal angle of resolution (logMAR) best-corrected visual acuity (BCVA) improved from 0.73 to 0.53 in the combined therapy group ( P < .001) and from 0.79 to 0.72 in the PDT monotherapy group ( P = .02), with a significant difference in treatment efficacy between the 2 groups ( P < .001). However, the improvements in BCVA were not statistically significant after 21 months in the combined therapy group and 15 months in the monotherapy group. The difference in treatment efficacy between the 2 groups was not significant after 6 months. Initial BCVA ( P = .005), lesion size ( P = .011), patient age ( P = .018), and location of polyps ( P = .006) significantly predicted the final visual outcome rather than treatment modality ( P = .243).
Conclusions
PDT combined with IVB for symptomatic PCV was temporarily superior to PDT monotherapy, and the treatment efficacy decreased with time. Initial BCVA, lesion size, and location were more significant than treatment modality as the factors influencing final visual improvement.
Polypoidal choroidal vasculopathy (PCV) is characterized by peculiar choroidal vascular networks terminating in aneurysmal or polypoidal lesions. These lesions often leak extensively and produce subretinal fluid (SRF), intraretinal fluid (IRF), and retinal pigment epithelium detachment (RPED). Large, established polyps look like orange-red protruding nodules on fundus examination, but more frequently the smaller polyps may be identified only on indocyanine green angiography (ICGA) or optical coherence tomography (OCT). The prevalence of this disease is relatively high in Asian populations, especially Japanese.
Although several treatment strategies have been proposed, there is still no consensus about the most effective treatment for macula-involved PCV. Among these treatment modalities, photodynamic therapy (PDT) and anti–vascular endothelial growth factor (VEGF) have relatively higher safety and better efficacy. The combination therapy of PDT with anti-VEGF also has good treatment effects, according to several short-term studies.
PDT with verteporfin (Visudyne; Novartis Pharma AG, Basel, Switzerland) has been proven to stabilize the visual acuity of most PCV patients, but some limitations and potential side effects of PDT were found in several reports. First, massive subretinal hemorrhaging may occur after treatment, leading to vitreous hemorrhaging. Second, PDT itself can cause damage resulting in complications such as retinal pigment epithelium (RPE) tearing, retinal atrophy, and scarring. Third, recurrent or newly developed lesions are not infrequent, affecting visual acuity over time.
Intravitreal injection of anti-VEGF, such as bevacizumab (Avastin; Genentech, South San Francisco, California, USA) and ranibizumab (Lucentis, Genentech), is another treatment option for PCV. This treatment has been found to be effective in reducing the fluid from PCV lesions, but the choroidal lesions were unaffected by this treatment alone. The effect of anti-VEGF after intravitreal injections is temporary because the drug is washed out with time. Some potential complications may also occur after intravitreal injections, such as endophthalmitis and retinal detachment.
Combination therapy of PDT and anti-VEGF drugs is another treatment choice for PCV. Although patients could get the benefits of both treatments, the postoperative complications of PDT and anti-VEGF, such as subretinal hemorrhage, retinal scarring, and endophthalmitis, may also happen. On the other hand, the efficacy and safety of combination therapy have not been evaluated sufficiently until recently. Because of the high recurrence rate of PCV, long-term results provide a better understanding of the treatment effects. Most previous studies investigating PDT combined with anti-VEGF have only had a follow-up period of 1 year. In this study, we report our 2-year results of PDT with or without intravitreal injections of bevacizumab (IVB) for PCV.
Methods
Retrospective chart review was performed in this study. Patients with treatment-naïve macula-involved PCV who received PDT alone or PDT combined with IVB in our hospital from January 1, 2007 to January 31, 2011 were enrolled in this study. Four ophthalmologists (C.H.Y., C.M.Y., T.C.H., C.P.L.) in our hospital performed the treatment; 2 of them (C.H.Y. and C.P.L.) routinely gave PDT only and the other 2 doctors (C.M.Y. and T.C.H.) routinely gave combination therapy. Patients were referred to different doctors randomly and received different treatments according to physician preference. The diagnosis of PCV was made based on the finding of characteristic polyp-like hyperfluorescence with or without a branching vascular network on ICGA. The inclusion criteria were as follows: 1) juxtafoveal, subfoveal, or extrafoveal active macular polypoidal lesions on ICGA; 2) macula-involved active lesions, such as submacular fluid, recent hemorrhage, lipid exudates, and macular edema as evidenced by OCT or fluorescein angiography (FAG); 3) initial best-corrected visual acuity worse than 20/32 (0.2 logarithm of minimal angle of resolution [logMAR]); 4) greatest linear dimension of the lesion of 5400 μm or less; and 5) follow-up of more than 24 months. The exclusion criteria were: 1) other ocular disease, such as epiretinal membrane, intraocular inflammation or infection, or diabetic retinopathy; 2) previous treatment for PCV; 3) any systemic contraindication to IVB, verteporfin, or angiographic dyes, such as uncontrolled hypertension, porphyria, or recent myocardial infarction; 4) severe systemic disease, such as a cerebral vascular accident or liver disease; and 5) scar tissue accounting for more than half of the PCV lesion.
Best-corrected visual acuity (BCVA), tonometry, and funduscopy were performed before treatment and at each follow-up visit. OCT, FAG, and ICGA were performed before treatment and at 3-month intervals routinely. Follow-up visits were arranged 1 week after treatment and then monthly. Additional OCT, FAG, and ICGA would be arranged as necessary at each follow-up visit. The BCVA measurement used a Snellen chart and was then converted to logMAR values. The patients in the PDT monotherapy group received 1 session of PDT at baseline. If leaking polyps were found on ICGA, additional sessions of PDT every 3 months were performed until they disappeared. The patients in the combined therapy group were treated with IVB followed by 1 session of PDT 1 week after IVB. These patients also received additional IVB each month over the next 2 months. If the patients in the combination therapy group needed re-treatment on the basis of the same criteria as in the monotherapy group, they also received 1 session of PDT 1 week after IVB and then received additional 2 treatments of IVB monthly over the next 2 months.
PDT with verteporfin infusion and laser application were performed using the full-fluence dose according to the Treatment of Age-related Macular Degeneration with Photodynamic Therapy protocol. In patients treated with combined therapy, 1.25 mg (0.05 mL) bevacizumab was injected intravitreously according to the treatment protocol. The IVB procedure was performed in an operating room with topical anesthesia. After strict aseptic techniques, bevacizumab was injected 3.5 to 4 mm posterior to the limbus using a 30-gauge needle. A topical antibiotic was prescribed 4 times daily for 3 days after the procedure.
The differences in BCVA values between baseline and 3-, 6-, 9-, 12-, 15-, 18-, 21-, and 24-month follow-up time points were analyzed in the 2 treatment groups. The changes in BCVA at 3, 6, 9, 12, 15, 18, 21, and 24 months from baseline were also compared between 2 groups. An increase in BCVA of more than 3 lines (logMAR BCVA change ≥3 lines) was considered an improvement, and a decrease of more than 3 lines (logMAR scale) was considered an aggravation. The percentages of BCVA improvement and aggravation were compared at 3, 12, and 24 months. At the 24-month follow-up time point, treatment times and the proportion of lesions with no leakage on ICGA and with no subfoveal edema, hemorrhage, or fluid on OCT and FAG were also compared between the 2 treatment groups. The Wilcoxon signed rank test or Mann-Whitney U test was used to compare continuous variables, and Fisher exact test was used to analyze categorical variables. Furthermore, we used linear regression tests to investigate whether age, sex, lesion size, baseline BCVA, or treatment modality had a significant impact on final visual outcome after 2 years of follow-up. Additionally, whether the polyps involved the subfoveal area and if RPE detachment, subretinal hemorrhage, or subretinal or intraretinal fluid was present at baseline were also included as the variables in the analysis of linear regression. Statistical analysis was performed using SPSS version 11.5.1 for Windows (SPSS Inc, Chicago, Illinois, USA). A P value less than .05 was considered significant.
Results
From January 1, 2007 to January 31, 2011, 69 eyes of 69 patients treated for PCV in National Taiwan University Hospital were included in our study according to the criteria described previously. Thirty-six eyes of 36 patients were treated with combined therapy, and 33 eyes of 33 patients were treated with monotherapy. The patient characteristics of both groups are listed in Table 1 . None of the baseline features differed significantly, including sex, age, initial BCVA, lesion size, polyp location, and the condition of macular lesions.
| Combined PDT With IVB (n = 36) | PDT Monotherapy (n = 33) | P Value | |
|---|---|---|---|
| Sex | |||
| Male, no. (%) | 21 (58.3%) | 18 (54.5%) | .76 |
| Female, no. (%) | 15 (41.7%) | 15 (45.5%) | |
| Age (years) | |||
| Mean ± SD | 67.8 ± 9.8 | 65.6 ± 9.5 | .35 |
| Baseline greatest linear dimension of lesion (ìm) | |||
| Mean ± SD | 2619 ± 843 | 2842 ± 1092 | .34 |
| Baseline logMAR BCVA | |||
| Mean ± SD | 0.73 ± 0.36 | 0.79 ± 0.37 | .48 |
| RPED, no. (%) | 27 (75%) | 26 (78.8%) | .71 |
| SRH, no. (%) | 20 (55.6%) | 21 (63.6%) | .50 |
| IRF or SRF, no. (%) | 33 (91.7%) | 31 (93.9%) | .72 |
| Location of polyps | |||
| Subfoveal | 9 (25%) | 7 (21.2%) | .71 |
| Juxtafoveal | 8 (22.2%) | 9 (27.3%) | .63 |
| Extrafoveal | 19 (52.8%) | 17 (51.5%) | .92 |
The mean BCVA scores in logMAR scale over time are shown in Figure 1 and Table 2 . In the combined therapy group, the mean BCVA at baseline was 0.73 ± 0.36. The mean BCVAs at 3, 6, 9, 12, 15, 18, 21, and 24 months posttreatment were 0.53 ± 0.35, 0.55 ± 0.40, 0.52 ± 0.37, 0.54 ± 0.38, 0.52 ± 0.40, 0.58 ± 0.43, 0.63 ± 0.45, and 0.61 ± 0.43, respectively. The improvements in BCVA were statistically significant at 3, 6, 9, 12, 15 (all P values < .001), and 18 months ( P = .02) after treatment. In the monotherapy group, the mean BCVA was 0.79 ± 0.37 at baseline and 0.72 ± 0.41, 0.70 ± 0.42, 0.68 ± 0.48, 0.68 ± 0.46, 0.71 ± 0.47, 0.73 ± 0.46, 0.72 ± 0.46, and 0.74 ± 0.48 at 3, 6, 9, 12, 15, 18, 21, and 24 months posttreatment, respectively. The improvements in BCVA were statistically significant at 3 ( P = .02), 6, 9, and 12 months (all P values = .01) after treatment.
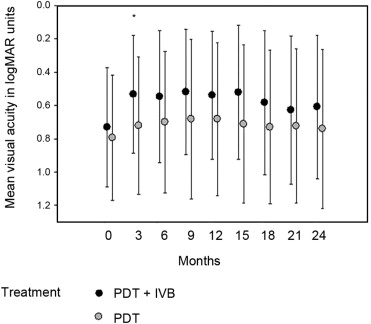
| Time From Initial Treatment (Mo) | PDT + IVB | PDT Alone | P Value (PDT + IVB vs PDT) | ||
|---|---|---|---|---|---|
| logMAR BCVA (Mean ± SD) | P Value (vs Baseline) | logMAR BCVA (Mean ± SD) | P Value (vs Baseline) | ||
| 0 | 0.73 ± 0.36 | 0.79 ± 0.37 | |||
| 3 | 0.53 ± 0.35 | <.001 | 0.72 ± 0.41 | .02 | <.001 |
| 6 | 0.55 ± 0.40 | <.001 | 0.70 ± 0.42 | .01 | .08 |
| 9 | 0.52 ± 0.37 | <.001 | 0.68 ± 0.48 | .01 | .11 |
| 12 | 0.54 ± 0.38 | <.001 | 0.68 ± 0.46 | .01 | .23 |
| 15 | 0.52 ± 0.40 | <.001 | 0.71 ± 0.47 | .08 | .08 |
| 18 | 0.58 ± 0.43 | .02 | 0.73 ± 0.46 | .17 | .33 |
| 21 | 0.63 ± 0.45 | .11 | 0.72 ± 0.46 | .17 | .68 |
| 24 | 0.61 ± 0.43 | .06 | 0.74 ± 0.48 | .30 | .41 |
Mean BCVA changes in logMAR scale were compared between the 2 treatment groups, and the difference was statistically significant at 3 months ( P < .001). Although the improvements were more apparent in the combined therapy group after 3 months, the difference was not statistically significant ( Table 2 ).
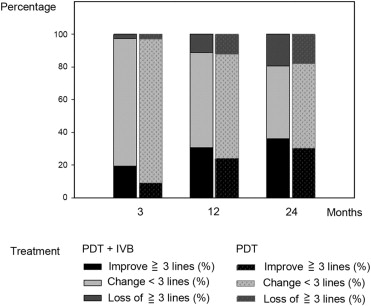
As shown in Figure 2 , at 3 months of follow-up, 7 of 36 patients (19.4%) in the combined therapy group and 3 of 33 patients (9.1%) in the monotherapy group gained more than 3 lines of vision ( P = .23). At 12 months and 24 months of follow-up, 11 of 36 (30.6%) and 13 of 36 (36.1%) patients in the combined therapy group and 8 of 33 (24.2%) and 10 of 33 (30.3%) patients in the monotherapy group gained more than 3 lines of vision ( P = .56 at 12 months, P = .62 at 24 months). On the other hand, at 3 months of follow-up, 1 of 36 patients (2.8%) in the combined therapy group and 1 of 33 patients (3.0%) in the monotherapy group lost more than 3 lines of vision ( P = .95). At 12 months and 24 months of follow-up, 4 of 36 (11.1%) and 7 of 36 (19.4%) patients in the combined therapy group and 4 of 33 (12.1%) and 6 of 33 (18.2%) patients in the monotherapy group lost more than 3 lines of vision ( P = .90 at 12 months, P = .89 at 24 months).
During the 2 years of follow-up, the patients in the combined therapy group received a mean of 2.25 treatments of PDT, whereas the patients in the monotherapy group received a mean of 2.55 treatments of PDT ( P = .149). We gave 4.33 and 2.42 bevacizumab injections on average, respectively, during the first and second year for patients in the combined therapy group. At 24 months of follow-up, 2 of 36 patients (5.6%) in the combined therapy group and 3 of 33 patients (9.1%) in the monotherapy group had residual leakage on ICGA ( P = .58), and 3 of 36 patients (8.3%) in the combined therapy group and 6 of 33 patients (18.2%) in the monotherapy group had lesions with residual subfoveal edema, hemorrhage, or fluid on OCT and FAG ( P = .23).
Based on the results of multivariate analysis, initial BCVA ( P = .005), lesion size ( P = .011), patient age ( P = .018), and whether the polyps involved the subfoveal area ( P = .006) significantly affected the final BCVA at 24 months. However, sex ( P = .465), treatment modality ( P = .243), and presence of RPE detachment ( P = .308), subretinal hemorrhage ( P = .215), or subretinal or intraretinal fluid ( P = .422) at baseline did not have a significant effect on the final BCVA change.
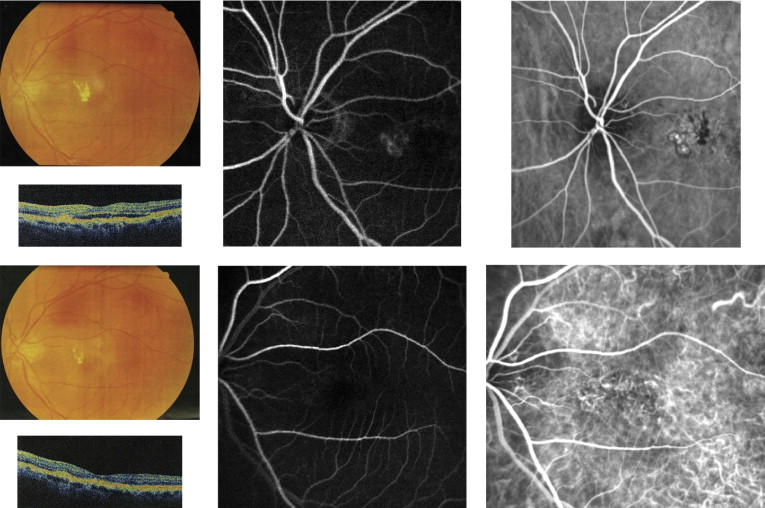
There were no complications such as infection, inflammation, or retinal detachment during follow-up in any of the patients. However, there were 9 eyes (9/36, 25%) in the combined therapy group and 7 eyes (7/33, 21.2%) in the monotherapy group that developed new hemorrhages after treatment during the 2-year period ( P = .71). Among them, massive subretinal hemorrhage or breakthrough vitreous hemorrhage developed in 6 of 36 eyes (16.7%) among the 36 patients treated with combined therapy and in 5 of 33 eyes (15.2%) in the 33 patients treated with PDT alone ( P = .87); the BCVA in all of these patients deteriorated severely. Examples of clinical changes after combined therapy and PDT monotherapy are shown in Figures 3 and 4 .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


